Purpose
To evaluate endothelial changes after excimer laser-assisted lamellar keratoplasty.
Design
Retrospective, interventional case series.
Methods
Seven eyes of 7 keratoconus patients were evaluated for 1 year after pachymetry-guided lamellar keratoplasty, performed using the iRES Laser (Ligi Tecnologie Medicali S.p.A.), with the Corneal Lamellar Ablation for Transplantation software (Ligi Tecnologie Medicali S.p.A.) procedure. Both anterior segment optical coherence tomography (Visante OCT; Carl Zeiss Meditec, Inc) and in vivo confocal microscopy (Corneal Confocal Microscope CS4; NIDEK Technologies) images were collected.
Results
Changes in morphologic features were investigated and the endothelium was assessed quantitatively in all 7 patients. In 6 eyes, we measured a mean residual bed thickness of 151.3 ± 5.46 μm, and a mean endothelial cell density loss of 5.38% at 1 year after surgery, as compared with preoperative values. The mean percentage hexagonality change was 15.67%, and the mean coefficient of variation change was −21.11%. In 1 eye, a residual bed thickness of 72 μm was found and endothelial loss after 1 year was 72.26%; assessment of the coefficient of variation and percentage hexagonality by manual Confoscan4 software (NIDEK Technologies) was not practicable in this case.
Conclusions
Our results showed that the Corneal Lamellar Ablation for Transplantation procedure induced mild changes to the endothelium in corneas with a mean residual bed thickness of 151.3 ± 5.46 μm, but serious damage in one eye with a residual bed thickness of 72 μm.
Anterior lamellar keratoplasty seems to be a safe alternative to penetrating keratoplasty in patients with keratoconus, ectasia after refractive surgery, and opacities not involving the full thickness of the cornea. Despite many advantages (extraocular surgery, thus decreasing the risk of intraocular damage, a reduced rate of graft failure resulting from endothelial rejection, reduced IOP disturbances, and lesser endothelial cell loss ), one of the main problems of anterior lamellar keratoplasty is still the visual outcome, which often is worse than that after penetrating keratoplasty. Interface scarring and irregularities are the main reasons proposed to explain the poorer optical results obtained after lamellar keratoplasty as compared with penetrating keratoplasty. To solve the interface problems, several authors have proposed different surgical techniques to remove the stroma as close to the Descemet membrane as possible and to obtain the smoothest possible recipient bed for the graft button.
Excimer laser-assisted lamellar keratoplasty may offer a further possibility in this field. In this surgical technique, a uniformly smooth posterior layer in the recipient cornea is prepared by excimer laser, and either a dehydrated lenticula with parallel faces and with a pre-established thickness and diameter or fresh cornea is placed inside the bed. Adverse effects of excimer laser on the corneal endothelium have been investigated after photorefractive keratectomy and laser in situ keratomileusis, but, to our knowledge, there are no published data about endothelial damage after laser-assisted lamellar keratoplasty in human cornea. In this study, we analyzed the quantitative and morphologic features of the endothelium in 7 keratoconic eyes that underwent excimer laser-assisted lamellar keratoplasty, using Corneal Lamellar Ablation for Transplantation (CLAT; Ligi Tecnologie Medicali S.p.A., Taranto, Italy) software and the iRES Laser (Ligi Tecnologie Medicali S.p.A.), with the aim of assessing the potential for endothelial damage when the excimer laser works close to the endothelium layer.
Methods
Patients
During the first 6 months of 2007, excimer laser-assisted lamellar keratoplasty using CLAT software for progressive keratoconus (Krumeich staging II to III) was performed at the Department of Ophthalmology and Otorhinolaryngology of the University of Bari, Bari, Italy, in 7 eyes (4 right and 3 left) of 7 patients (6 males and 1 female) ranging in age between 20 and 43 years (mean, 31 years; standard deviation [SD], 8.9 years). Progression of the keratoconus, based on serial differential topography, was defined as an increase in the apex keratometry by more than 1.0 to 1.5 diopters (D) and a corresponding change (>1.0 to 1.5 D) in the refractive cylinder in the previous 6 months. Follow-up lasted 12 months. No patient had general health problems. Patients could not tolerate contact lenses or the cylindrical correction in their spectacles or contact lenses. None of the 7 eyes had glaucoma, uveitis, or a history of ocular trauma or previous ocular surgery. The study protocol was approved by the local ethics committee and each subject gave written informed consent after receiving a thorough explanation of the surgery and its attendant risks.
Clinical Examination
A comprehensive preoperative and postoperative ophthalmic examination was made of all the eyes, including slit-lamp biomicroscopy evaluation, uncorrected visual acuity and best spectacle-corrected visual acuity (BSCVA), manifest refraction spherical equivalent, corneal topography, applanation tonometry, indirect ophthalmoscopy, tomographic evaluation (anterior segment optical coherence tomography [AS OCT]; Visante OCT; Carl Zeiss Meditec, Inc, Dublin, California, USA) and in vivo confocal microscopy (Corneal Confocal Microscope CS4; NIDEK Technologies, Erlangen, Germany). Visual acuity was assessed using the Early Treatment Diabetic Retinopathy Study chart. We evaluated subjective refraction because of the difficulty in making an objective assessment of refraction in patients with an irregular corneal surface. Mean central K readings, minimum corneal thickness, and a corneal pachymetry map were obtained by means of the Precisio tomographer (Ligi Tecnologie Medicali S.p.A.). The postoperative follow-up visits were at 1, 3, 6, and 12 months.
Anterior-Segment Optical Coherence Tomography Analysis
With the AS OCT Visante, we evaluated the preoperative minimum corneal thickness and the postoperative recipient bed thickness. Only one type of scan pattern was used throughout the study, namely the high-resolution corneal pattern horizontal scan. Three flap tools were placed manually in positions 0.00, −2.00, and +2.00 mm with respect to the corneal vertex. Four consecutive frames were saved at each scanning session.
Confocal Microscopy Analysis
Images of the central corneal endothelium were acquired and the NAVIS Endo Cell Analysis Software (NIDEK Technologies) was used to perform an automated endothelium evaluation. In the selected region of interest (ROI), the main outcome measures were the endothelial cell count (ECD), coefficient of variation (to evaluate polymegathism), and the percentage of hexagonal cells (6-sided cells [6SC] to evaluate polymorphism). In all patients but one (Patient 7), we selected a region of interest area of 0.0345 mm 2 . In Patient 7, a region of interest area of 0.09 mm 2 was selected. The minimum number of cells entered in the calculation was 66 in the first 6 eyes. In Patient 7, the minimum cell number was 35. The mean of 3 consecutive measurements was recorded.
Surgical Technique
The CLAT is a paradigm shift that allows the surgeon to execute a totally automated custom lamellar transplantation of the cornea. Unlike keratome or laser keratome lamellar surgeries, which use the anterior surface as reference and provide cuts of constant thickness, this procedure removes corneal irregularities as a preparation to inserting the matched uniform thickness donor lenticula. Both the corneal bed and the donor lenticula are prepared using CLAT software and excimer laser.
The first step is to acquire the pachymetric map, obtained by means of Precisio tomographer (Ligi Tecnologie Medicali S.p.A.). Using a Scheimpflug rotating camera, this device provides 3-dimensional elevation data from the anterior and posterior corneal surface and anterior chamber dimensions, with a repeatability of less than 3 μm. In 1 second, 50 high-resolution images are acquired for assessment of 39 000 points on each surface. An integrated infrared passive-active and torsional eye-tracker system (the latter based on perilimbal and iris vessels) is installed. The data obtained are processed by CLAT software. The receiving bed is created by calculating the intersection of the acquired pachymetric map and the ideal corneal bed for the patient, that is, a uniform thickness receiving bed that takes into account the standard physiologic pachymetric gradient of the cornea, calculated by CLAT software on a statistical basis. After the ideal corneal bed has been created, the ablation is planned on the donor button. The CLAT will calculate an ablation profile to create a peripheral saddle that, after being placed, will ensure a better matching of the lamella with the patient’s corneal bed. We adopt a donor lenticula with a saddle that has a planned peripheral flange tissue 1 mm wide and 100 μm thick.
The processed data were transferred to the iRES laser to execute the ablations on both the patient and the donor lamella. This device is a dual flying-spot excimer laser, with a Gaussian microspot of 650 μm, an effective frequency of 1000 Hz, and a fluence of 250 mJ/cm 2 .
In all 7 patients, we used plane dehydrated lenticulae in a silicon gel, provided by the eye bank Fondazione Banca degli Occhi del Veneto ONLUS, Venezia, Italy. The thickness of the lamella ranged between 330 and 390 μm, and the diameter measured between 8.5 and 9.5 mm. These buttons were rehydrated in balanced salt solution for 10 minutes before surgery.
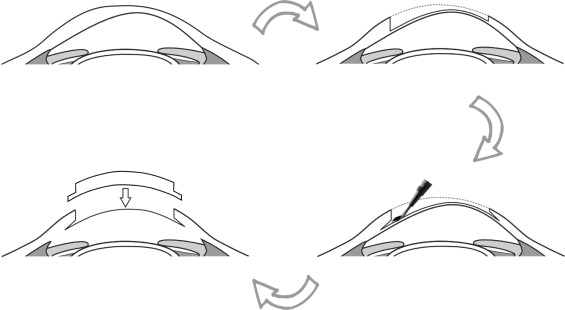
All surgery was performed by the same experienced surgeon (G.A.), administering lidocaine 4% eye drops as topical anesthesia. The surgical process was begun by placing a laser-opaque ring with the same diameter as the selected ablation zone onto the host cornea; this ensures peripheral sharp edges. The total ablation time was 90 to 120 seconds because of the 1-kHz frequency. After recipient bed creation, in all patients the excimer laser was used in phototherapeutic keratectomy mode (an ablation diameter of 8 mm and a depth of 30 μm) with masking fluid (sodium hyaluronate 0.25% [Laservis; TRB Chemedica AG, Haar, Munchen, Germany]) to remove residual stromal irregularities and to smooth the corneal surface. Surgical steps are pictured in Figure 1 . After ablation, a 1-mm pocket was created around the circumference of the ablated area and then the donor button was positioned, inserting the edges into the created pocket. Last, the corneal lenticula was sutured into place with a single running 24-bites 10-0 nylon suture. During surgery, the corneal astigmatism was evaluated using a keratoscope (Asti Disc Type 00Asti; Morcher GmbH, Stuttgart, Germany) to adjust sutures as required.
At the end of surgery, a bandage contact lens was applied. Postoperative treatment consisted of homatropine eyedrops twice daily and ofloxacin eyedrops 4 times daily until the epithelium healed. The contact lens was removed 4 days after surgery in all cases. When epithelialization was complete, only topical dexamethasone was continued, tapered over 3 months at the surgeon’s discretion. In all patients, the corneal sutures were removed at least 3 months after surgery (mean ± SD, 4.3 ± 1.8 months).
Results
In all patients but one, the treatment aimed to leave a recipient bed thickness of 150 μm, and 3 months after surgery, the AS OCT Visante system showed agreement between the predicted and the obtained bed thickness (mean, 151.3 μm; range, 145 to 159 μm; SD, 5.46 μm). In Patient 7, the treatment was planned so as to leave a residual central corneal bed of 100 μm, but at 3 months, the measured bed thickness in the central cornea was significantly lower (28%), being equal to only 72 μm.
Visual Acuity and Refractive Results
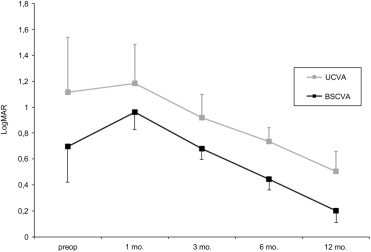
Figure 2 shows the changes in both uncorrected visual acuity and BSCVA over time. At 12 months, the BSCVA had improved by 1 line in 2 eyes (28.5%) and by 3 lines or more in 5 eyes (71.4%). No eye lost Snellen lines of BSCVA. Table 1 shows the preoperative and postoperative (1-year) uncorrected visual acuity, BSCVA, mean central K readings, and mean manifest refraction spherical equivalent, together with the preoperative minimum corneal thickness (evaluated by both the AS OCT Visante and Precisio tomographer).
| Preoperative | Postoperative (12 mos) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Case No. | Age (yrs) | MCKR | MCT, Visante OCT (μm) | Precisio (μm) | UCVA | BSCVA | MRSE (D) | MCKR | UCVA | BSCVA | MRSE |
| 1 | 20 | 52.50 | 355 | 360 | 20/200 | 20/100 | –6 | 44.35 | 20/70 | 20/30 | −2.5 |
| 2 | 31 | 53.28 | 431 | 426 | 20/160 | 20/80 | –2 | 45.56 | 20/40 | 20/25 | 1.75 |
| 3 | 43 | 51.75 | 414 | 426 | 20/125 | 20/60 | –9 | 46.12 | 20/60 | 20/30 | −2 |
| 4 | 24 | 54.36 | 402 | 407 | 20/125 | 20/70 | –7 | 47.75 | 20/50 | 20/30 | −3 |
| 5 | 28 | 55.08 | 350 | 364 | 20/400 | 20/200 | –9.5 | 45,34 | 20/70 | 20/30 | 2 |
| 6 | 28 | 54.89 | 320 | 325 | 20/2000 | 20/300 | –10.5 | 45.25 | 20/60 | 20/30 | 1.75 |
| 7 | 43 | 51.06 | 398 | 412 | 20/200 | 20/70 | –6.75 | 49.26 | 20/125 | 20/50 | −2.75 |
Anterior-Segment Optical Coherence Tomography Analysis
In all patients, the AS OCT revealed a complete graft apposition, producing a good anatomic result. In the first 6 eyes, the treatment was planned to leave a residual central bed thickness of 150 μm ( Figure 3 , Top). The Visante OCT showed that the predicted bed thickness corresponded to the measured bed thickness in the central cornea ( Table 1 ). We preferred to measure the thickness 3 months after surgery to avoid errors resulting from postoperative stromal edema. In the seventh eye, the Visante OCT system revealed a residual bed thickness of 72 μm ( Figure 3 , Bottom).
Endothelial Results
Assessment of the morphologic appearance and the morphometric parameters of the endothelium induced by excimer laser-assisted lamellar keratoplasty was performed by in vivo confocal microscopy. We report the first 6 patients and Patient 7 separately, because in the latter we obtained very different results.
Qualitative analysis of the endothelial layer is shown in Figure 4 , for 1 sample of the first 6 eyes (all very similar) and for the seventh eye. Comparisons between the preoperative and postoperative ECD, coefficient of variation, and 6SC for the 7 eyes at 1, 3, 6, and 12 months after treatment are summarized in Tables 2 and 3 , respectively. Mean ECD was 2963.16/mm 2 (range, 2376 to 3365/mm 2 ; SD, 355.8/mm 2 ) before surgery, 2707.33/mm 2 (range, 2432 to 2926/mm 2 ; SD, 187.7/mm 2 ) 1 month after surgery, and 2803.67/mm 2 (range, 2487 to 3017/mm 2 ; SD, 175.25/mm 2 ) at 12 months ( Table 2 ). Our results showed that in these eyes, the mean endothelial cell loss from preoperative values to 1 month after surgery was 8.63%, and from preoperative values to 12 months after surgery, it was 5.38%.
| Postoperative (mos) | |||||
|---|---|---|---|---|---|
| Eye No. | Preoperative | 1 | 3 | 6 | 12 |
| 1 | 2915 ± 19.1 | 2812 ± 22 | 2883 ± 26.1 | 2891±17.7 | 2872 ± 19.1 |
| 2 | 2901 ± 23.7 | 2742 ± 21.3 | 2835 ± 23.4 | 2840 ± 19.9 | 2811 ± 22.4 |
| 3 | 2376 ± 32.1 | 2530 ± 25.4 | 2545 ± 21.1 | 2742 ± 20.6 | 2781 ± 24.8 |
| 4 | 2915 ± 18.2 | 2432 ± 18.6 | 2504 ± 19.5 | 2881 ± 17.8 | 2487 ± 19.5 |
| 5 | 3307 ± 11.6 | 2926 ± 15.4 | N.A. | N.A. | 3017 ± 16.4 |
| 6 | 3365 ± 10.5 | 2802 ± 16.2 | N.A. | N.A. | 2854 ± 14.2 |
| 7 | 2840 ± 9.8 | 397.7 a ± 2.1 | 442.1 a ± 3.1 | 658.9 a ± 2.4 | 787.8 a ± 3.2 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


