The article focuses on the evidence basis for the management of benign paroxysmal positional vertigo, the most common diagnosis of vertigo in both primary care and subspecialty settings. An overview is presented, along with evidence-based clinical assessment, diagnosis, and management. Summaries of differential diagnosis of vertigo and outcomes are presented.
The following points list the level of evidence as based on Oxford Center for Evidence-Based Medicine.
- •
Benign paroxysmal positional vertigo (BPPV) is the most common diagnosis of vertigo (level 4).
- •
Dix-Hallpike maneuver is the diagnostic test for posterior canal BPPV (level 1).
- •
Supine roll test is the diagnostic test for lateral canal BPPV (level 2).
- •
Epley maneuver is the first-line treatment for posterior canal BPPV (level 1).
- •
Posterior semicircular canal occlusion is an effective treatment for recalcitrant posterior canal BPPV (level 4).
- •
Lateral canal BPPV can be treated with a variety of repositioning maneuvers (level 2).
OCEBM Levels of Evidence Working Group. a “The Oxford 2011 Levels of Evidence.” Oxford Center for Evidence-Based Medicine. http://www.cebm.net/index.aspx?o=5653 .
a OCEBM Levels of Evidence Working Group—Jeremy Howick, Iain Chalmers (James Lind Library), Paul Glasziou, Trish Greenhalgh, Carl Heneghan, Alessandro Liberati, Ivan Moschetti, Bob Phillips, Hazel Thornton, Olive Goddard, and Mary Hodgkinson.
Problem overview
Vertigo
Vertigo is a symptom, not a disease. Effective diagnosis and management of vertigo begin with understanding what the symptom may represent. A survey of the members of the American Otological Society and the American Neurotology Society revealed that 75% of respondents agreed or agreed strongly that the definition of vertigo in clinical practice should be more precise. Whereas 45% of respondents favored restricting vertigo to describe a sensation of spinning or turning only, 40% of respondent favored including any sensation of movement in the definition of vertigo. Since acute inner ear pathology typically produces a spinning sensation, the more restrictive definition of vertigo renders it a more specific clue for a possible otologic vestibular disorder. A narrow focus on spinning may not be sensitive to chronic or milder inner ear pathology, however, where sensation of movement other than spinning might be elicited. Even though a consensus has not been reached on the precise definition of vertigo, it is reasonable to infer from the survey results that the overwhelming majority of otologists would recognize vertigo as distinct from other flavors of dizziness, such as presyncopal lightheadedness, disequilibrium, or other unsettling sensations.
Epidemiologic surveys showed that 20% to 30% of the population may have experienced vertigo or dizziness in their lifetime. A German national telephone health survey followed by structured neurotologic interview identified the lifetime prevalence of vestibular vertigo to be 7.8%, with an annual incidence of 1.5%. In the United States, 1.7% of ambulatory medical care visits recorded vertigo or dizziness among the chief complaints. Vertigo or dizziness also accounted for 2.5% of presentations to US emergency department in the years 1995 to 2004.
Vertigo is a symptom in a wide range of disorders ( Table 1 ). The article focuses on the evidence basis for the management of benign paroxysmal positional vertigo (BPPV), the most common diagnosis of vertigo in both primary care and subspecialty settings.
| Otological Conditions | Neurological Conditions | Others |
|---|---|---|
| Benign paroxysmal positional vertigo | Migraine-associated vertigo | Postural hypotension |
| Vestibular neuritis/labyrinthitis | Vertebrobasillar insufficiency | Medication side effects |
| Meniere disease | Demyelinating diseases | Anxiety or panic disorder |
| Superior semicircular canal dehiscence | CNS lesions | Cervical vertigo |
Benign paroxysmal positional vertigo
BPPV is a disorder of the inner ear characterized by episodes of vertigo triggered by changes in head position. BPPV is thought to be caused by the presence of endolymphatic debris in 1 or more semicircular canals. Direct evidence of such debris or canaliths has been demonstrated for posterior canal BPPV. The presence of debris in lateral canal BPPV has not been demonstrated directly. However, treatment of posterior canal BPPV by repositioning the debris can lead to lateral canal BPPV. By inference, lateral canal BPPV can also be caused by endolymphatic debris.
A population-based study estimates BPPV has a life-time prevalence of 2.4% and accounts for 8% of the individuals with moderate-to-severe dizziness or vertigo.
Posterior canal BPPV account for about 90% of the cases, and lateral canal BPPV accounts for about 8% of the cases, according to a review of 10 series with a total of 3342 patients. In rare instances, the anterior canal or multiple canals might be involved.
Evidence-based clinical assessment
Diagnosis of Posterior Canal BPPV
The diagnosis of BPPV affecting the posterior semicircular canal is established by a history of episodic vertigo with changes in head position and the presence of characteristic nystagmus provoked by the Dix-Hallpike test according to a guideline from the American Academy of Otolaryngology-Head and Neck Surgery.
The Dix-Hallpike test ( Fig. 1 ) is generally considered the gold standard test for the diagnosis of posterior canal BPPV in that it is the most common diagnostic criterion required for entry into clinical trials and for inclusion of such trials in meta-analyses. The Dix-Hallpike test is not truly 100% sensitive, however, since BPPV is an intermittent condition, and variations in examiners’ technique and experience might affect the test outcome. The sensitivity of the Dix-Hallpike test has been estimated at 48% to 88% according to a structured review of published literature. The same review found that estimates for specificity are lacking. In the primary care setting, the Dix-Hallpike test reportedly has a negative predictive value of 52% for the diagnosis of BPPV. In a different series of 95 patients diagnosed and treated for posterior canal BPPV in a specialty clinic, 11 patients did not have a positive Dix-Hallpike on initial examination, and 28 presented with an atypical history that did not suggest BPPV. Given these considerations, the Dix-Hallpike test should be routinely performed if possible in the evaluation of vertigo/dizziness. Whereas a positive test should be considered sufficient for the diagnosis of BPPV in the clinical setting, a negative test should not rule out BPPV completely. Repeated testing in separate occasions may be necessary to avoid missing the diagnosis. Failure to diagnose BPPV may lead to costly diagnostic work-up.

Diagnosis of Lateral Canal BPPV
The diagnosis of BPPV affecting the lateral semicircular canal is established with a history of episodic vertigo with changes in head position and the presence of horizontal nystagmus provoked by the supine roll test according to a guideline from the American Academy of Otolaryngology-Head and Neck Surgery.
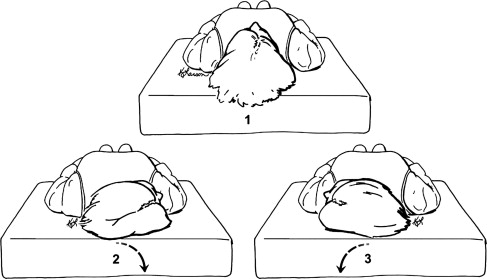
The supine roll test ( Fig. 2 ) is performed by rotating the patient’s head from neutral to one side while the patient is lying supine. After waiting for any nystagmus or vertigo to subside, the test is performed to the opposite side. In a positive test, horizontal nystagmus is observed, either beating toward the dependent ear (geotropic) or beating away from the dependent ear (apogeotropic) on both sides. For geotropic nystagmus, the side associated with the stronger nystagmus is likely the affected ear. For apogeotropic nystagmus, the side associated with the weaker nystagmus is the likely the affected ear. Geotropic nystagmus is more common and suggests that the canaliths are located in the long arm of the lateral canal far from the cupula. Apogeotropic nystagmus is less common and suggests that the canaliths are located very close to the cupula or possibly embedded in it. In a review of 9 series with a total of 257 patients with lateral canal BPPV, geotropic nystagmus accounted for about 70% of the cases, and apogeotropic nystagmus accounted for about 30% of the cases.
The supine roll test is the most commonly accepted criterion for the diagnosis of lateral canal BPPV in clinical trials. There is no literature on the sensitivity or specificity of this test in the diagnosis of lateral canal BPPV, partly because clinical history alone is often not sufficient for diagnosis, and there is no other gold-standard test to which the supine roll test can be compared.
Limitations of Diagnostic Maneuvers for BPPV
Patients with the following physical limitations may not be good candidate for Dix-Hallpike or supine head roll test: cervical stenosis, severe kyphoscoliosis, limited cervical range of motion, Down syndrome, severe rheumatoid arthritis, cervical radiculopathies, Paget disease, ankylosing spondylitis, low back dysfunction, spinal cord injuries, and morbid obesity. A power-driven, multiaxial positioning chair may facilitate testing of such patients. Alternatives to the Dix-Hallpike test for the diagnosis of posterior canal BPPV have not been well established.
Evidence-based clinical assessment
Diagnosis of Posterior Canal BPPV
The diagnosis of BPPV affecting the posterior semicircular canal is established by a history of episodic vertigo with changes in head position and the presence of characteristic nystagmus provoked by the Dix-Hallpike test according to a guideline from the American Academy of Otolaryngology-Head and Neck Surgery.
The Dix-Hallpike test ( Fig. 1 ) is generally considered the gold standard test for the diagnosis of posterior canal BPPV in that it is the most common diagnostic criterion required for entry into clinical trials and for inclusion of such trials in meta-analyses. The Dix-Hallpike test is not truly 100% sensitive, however, since BPPV is an intermittent condition, and variations in examiners’ technique and experience might affect the test outcome. The sensitivity of the Dix-Hallpike test has been estimated at 48% to 88% according to a structured review of published literature. The same review found that estimates for specificity are lacking. In the primary care setting, the Dix-Hallpike test reportedly has a negative predictive value of 52% for the diagnosis of BPPV. In a different series of 95 patients diagnosed and treated for posterior canal BPPV in a specialty clinic, 11 patients did not have a positive Dix-Hallpike on initial examination, and 28 presented with an atypical history that did not suggest BPPV. Given these considerations, the Dix-Hallpike test should be routinely performed if possible in the evaluation of vertigo/dizziness. Whereas a positive test should be considered sufficient for the diagnosis of BPPV in the clinical setting, a negative test should not rule out BPPV completely. Repeated testing in separate occasions may be necessary to avoid missing the diagnosis. Failure to diagnose BPPV may lead to costly diagnostic work-up.
Diagnosis of Lateral Canal BPPV
The diagnosis of BPPV affecting the lateral semicircular canal is established with a history of episodic vertigo with changes in head position and the presence of horizontal nystagmus provoked by the supine roll test according to a guideline from the American Academy of Otolaryngology-Head and Neck Surgery.
The supine roll test ( Fig. 2 ) is performed by rotating the patient’s head from neutral to one side while the patient is lying supine. After waiting for any nystagmus or vertigo to subside, the test is performed to the opposite side. In a positive test, horizontal nystagmus is observed, either beating toward the dependent ear (geotropic) or beating away from the dependent ear (apogeotropic) on both sides. For geotropic nystagmus, the side associated with the stronger nystagmus is likely the affected ear. For apogeotropic nystagmus, the side associated with the weaker nystagmus is the likely the affected ear. Geotropic nystagmus is more common and suggests that the canaliths are located in the long arm of the lateral canal far from the cupula. Apogeotropic nystagmus is less common and suggests that the canaliths are located very close to the cupula or possibly embedded in it. In a review of 9 series with a total of 257 patients with lateral canal BPPV, geotropic nystagmus accounted for about 70% of the cases, and apogeotropic nystagmus accounted for about 30% of the cases.
The supine roll test is the most commonly accepted criterion for the diagnosis of lateral canal BPPV in clinical trials. There is no literature on the sensitivity or specificity of this test in the diagnosis of lateral canal BPPV, partly because clinical history alone is often not sufficient for diagnosis, and there is no other gold-standard test to which the supine roll test can be compared.
Limitations of Diagnostic Maneuvers for BPPV
Patients with the following physical limitations may not be good candidate for Dix-Hallpike or supine head roll test: cervical stenosis, severe kyphoscoliosis, limited cervical range of motion, Down syndrome, severe rheumatoid arthritis, cervical radiculopathies, Paget disease, ankylosing spondylitis, low back dysfunction, spinal cord injuries, and morbid obesity. A power-driven, multiaxial positioning chair may facilitate testing of such patients. Alternatives to the Dix-Hallpike test for the diagnosis of posterior canal BPPV have not been well established.
Evidence-based medical and surgical management
Natural Remission of Vertigo in BPPV
BPPV is termed benign because it is a naturally resolving condition. In 70 patients with posterior canal BPPV who were observed without treatment, the average time to resolution of vertigo was 39 days, but it took up to 6 months in the extreme. In 16 patients with geotropic variant of lateral canal BPPV who were observed without treatment, the average time to resolution of vertigo was 16 days, and all were free of vertigo in 2.5 months. In 14 patients with apogeotropic variant of lateral canal BPPV, the average time to resolution of vertigo was 13 days, and maximum time was 35 days. Despite its favorable prognosis, BPPV is not an entirely benign condition, especially in the elderly, in whom it is often unrecognized and can lead to falls.
Repositioning Maneuvers for Posterior Canal BPPV
There are 2 effective particle repositioning methods for treatment of posterior canal BPPV: the Epley maneuver ( Fig. 3 ) and the Semont maneuver ( Fig. 4 ). Both are designed to move the endolymphatic debris from the posterior semicircular canal into the vestibule, where it does not cause vertigo. The Epley maneuver has been extensively studied and is recommended as the first-line treatment of posterior canal BPPV in guidelines from both the American Academy of Otolaryngology-Head and Neck Surgery and the American Academy of Neurology.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


