In spite of significant advances in the management of endophthalmitis over the past two decades, numerous issues remain unresolved. There is no doubt that approximately 20 years ago, the advent of intravitreal antibiotics paved the way for notably improved visual and anatomic outcomes. In the mid-1990s, the Endophthalmitis Vitrectomy Study (EVS) addressed the role of vitrectomy versus vitreous tap in the treatment of postoperative endophthalmitis, and documented that patients with hand motion or better vision fared equally well with either a complete pars plana vitrectomy or a vitreous tap.
1 In a subgroup analysis it was noted that in patients with a visual acuity of light perception the outcome was better in the vitrectomy group. Both procedures employed intravitreal antibiotics consisting of vancomycin and amikacin. This study provided ophthalmologists with evidence-based outcomes in the management of postoperative endophthalmitis for the first time.
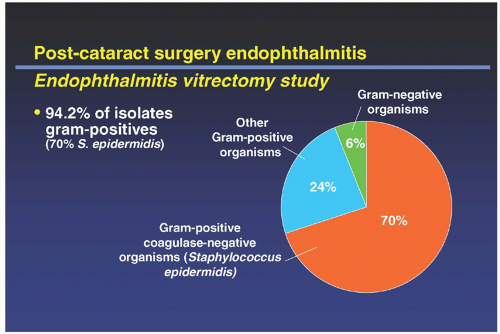
The EVS also provided ophthalmologists with very important data regarding the pathogens that most commonly cause postoperative endophthalmitis (see
Fig. 11.1). Additionally, the study determined that there was no apparent benefit from the use of intravenous antibiotics (cephalosporins and aminoglycosides).
1 The systemic antibiotics chosen in the EVS were the best available at the time; however, several studies following the completion of the EVS revealed that systemically administered cephalosporins and aminoglycosides do not readily achieve therapeutic intraocular concentrations in the vitreous cavity.
2,3Unfortunately, even within the confines of a well-conceived and well thought-out multicenter, prospective clinical trial like the EVS, a number of pertinent issues remain unresolved or were not fully addressed in the original study. These include the choice of the intravitreal antibiotics (ceftazidime was not employed, and today it has virtually replaced intravitreal amikacin), the management of types of endophthalmitis not specifically studied in the EVS (filtering bleb-associated, posttraumatic, indolent, postintravitreal injection and fungal endophthalmitis), the role of intravitreal corticosteroids, and inpatient versus outpatient management of infection.
Additionally, since the completion of the EVS, new antibiotics such as the fourth-generation fluoroquinolones have been developed, and these agents will most likely play a key role in the treatment of proven infection or in the prophylaxis against infection in the near future (as described in the following text).
The Endophthalmitis Vitrectomy Study
In the late 1980s, the EVS group set out to determine the role of vitrectomy versus vitreous tap in the treatment of postoperative endophthalmitis, and to address the role of intravenous antibiotics versus no intravenous antibiotics in treating endophthalmitis. Vitrectomy was introduced in the 1970s and many surgeons began to employ it in conjunction with intravitreal antibiotics for treating endophthalmitis. There were several theoretical advantages to vitrectomy including the removal of the infecting organisms and
their toxins, better distribution of antibiotics, clearing of tractional membranes that could lead to retinal detachment, clearing of opacities in the vitreous, and providing a good volume of vitreous material for microbiologic culture. Before the EVS, small human studies were inconclusive regarding the benefits of vitrectomy and in previous studies it appeared that only the most advanced cases of endophthalmitis underwent vitrectomy. Therefore, visual outcomes were poor and it was uncertain if vitrectomy would yield superior outcomes in eyes with better presenting vision. In the late 1980s, the role of vitrectomy in the management of endophthalmitis remained quite controversial. During this time, the role and benefit of systemic intravenous antibiotics in the management of endophthalmitis was also uncertain. It was the “standard of care,” yet it was questioned whether the theoretical benefit outweighed the systemic side effects of antibiotics used at the time. Additional factors included an analysis of the costs of the antibiotics and hospitalization for administration of these drugs. These unresolved issues served as the impetus for the largest prospective study on endophthalmitis management to date.
4Clinical centers in 25 US cities enrolled 420 patients over a 3 1/2-year time frame. Entry criteria were stringent and were limited to patients who had a clinical diagnosis of endophthalmitis within 6 weeks of cataract extraction or secondary intraocular lens (IOL) placement and had a vision worse than 20/50 but at least light perception. Additionally, patients were required to have a hypopyon and clouding of the anterior chamber or vitreous media sufficient to obscure clear visualization of second-order retinal arterioles. Patients who did not have a cornea and anterior chamber clear enough to visualize at least a portion of their iris were excluded. Furthermore, the cornea needed to be clear enough to allow the possibility of pars plana vitrectomy.
4All eyes in the EVS underwent immediate cultures of the anterior chamber and vitreous. Intravitreal amikacin and vancomycin were administered, as were subconjunctival vancomycin and ceftazidime. Topical vancomycin,
amikacin, and cycloplegics were administered in all patients as well.
1Patients were randomized to the following groups: (a) Three-port pars plana vitrectomy with intravenous antibiotics (ceftazidime and amikacin); (b) three-port pars plana vitrectomy without intravenous antibiotics; (c) vitreous tap with intravenous antibiotics; and (d) vitreous tap without intravenous antibiotics.
1 The vitreous tap could be performed with or without a cutting type instrument, with a tap defined as removal of <0.3 ml of vitreous fluid.
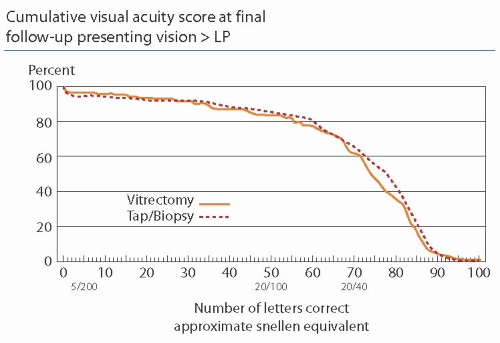
The EVS found no difference in outcomes between immediate three-port pars plana vitrectomy and vitreous tap/biopsy for patients with hand motion or better vision (
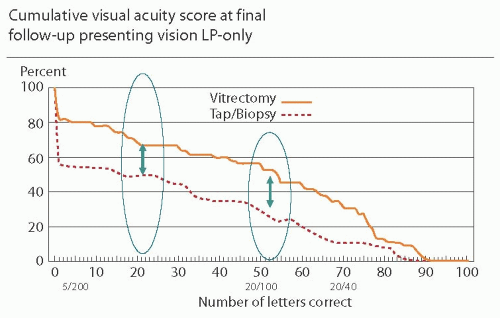
Fig. 11.2). In a subgroup analysis it was noted that in patients with a visual acuity of only light perception, improved visual results occurred in the immediate three-port pars plana vitrectomy group as compared to the vitreous tap/biopsy group. These patients were three times more likely to achieve >20/40 vision (33% vs. 11%), two times more likely to achieve >20/100 vision (56% vs. 30%), and less likely to incur a vision <5/200 (20% vs. 47%) (
Fig. 11.3). No difference in final visual acuity or media clarity was noted, whether or not systemic antibiotics were employed.
1Confirmed bacterial growth isolates were more likely to be positive in the vitreous compared to aqueous specimens.
Figure 11.1 demonstrates that 94.2% of confirmed growth isolates were gram-positive organisms (the vast majority due to one organism alone
Staphylococcus epidermidis—70%). Gram-negative
organisms only comprised 5.9% of confirmed growth isolates. At the time of the EVS, all gram-positive organisms were sensitive to vancomycin. However, 2 of the 19 gram-negative organisms were resistant to both amikacin and ceftazidime.
5,6,7,8An analysis was performed to determine the causes of <20/40 vision after endophthalmitis. The following etiologies were found: pigmentary degeneration of the macula (18%), macular edema (17%), unclear etiology (14%), and miscellaneous causes (10%). Epiretinal membranes, presumed optic nerve damage, corneal opacity, phthisis, posterior capsular opacity, retinal detachment, macular ischemia, and vitreous opacities each accounted for <10% of causes for <20/40 vision after endophthalmitis.
1A subset analysis of patients with diabetes included in the EVS resulted in two interesting findings. First, diabetes was associated with a higher yield of
S. epidermidis. Second, only 39% of patients with diabetes had a final visual outcome of >20/40 as compared to 55% of patients without diabetes. As a group, patients with diabetes fared worse and attained a less desirable visual outcome as compared to patients without diabetes.
1Retinal detachment occurred with an overall incidence of 8.3%. There was a minimal difference in the rates between the three-port vitrectomy group (7%) and the vitreous tap/biopsy group (9%). Retinal detachment repair was attempted in 66% of patients. The likelihood of obtaining a final visual outcome of >20/40 was 55% without a retinal detachment as compared with only 26% of patients who had a retinal detachment.
1The EVS answered some of the most controversial issues surrounding the management of endophthalmitis at the time. It was a well-designed study that utilized antibiotics that were the best available in the late 1980s. Additionally, the EVS taught us valuable information regarding the spectrum of causative organisms in postoperative endophthalmitis. The EVS clearly was a landmark study that provided ophthalmologists with evidence-based outcomes for managing postoperative endophthalmitis.
European Society of Cataract and Refractive Surgeons (ESCRS) Study of Prophylaxis of Postoperative Endophthalmitis after Cataract Surgery
In March of 2008, the European Registry of Quality Outcomes for Cataract and Refractive Surgery (EUREQUO) commenced. The ESCRS became the lead partner with 11 national societies as associated partners. The aims of this monumental effort were to improve treatment and standards of care for cataract and refractive surgery and to develop evidence-based guidelines for cataract and refractive surgery across Europe. The database contained data on 820,000 cataract surgeries roughly 3 years after commencing the project. Analysis included many variables spanning from outpatient versus inpatient surgery to type of IOLs chosen to same-day bilateral surgery. Of interest to this review is the European data regarding use of antibiotics in the setting of cataract surgery.
9The ESCRS multicenter study of the prophylaxis of endophthalmitis after cataract surgery study began in September 2003 and was terminated early in January 2006. The study included 24 ophthalmology centers in Austria, Belgium, Germany, Italy, Poland, Portugal, Spain, Turkey, and the United Kingdom. This randomized, placebo-controlled, multinational clinical study sought to evaluate prospectively the prophylactic effect of intracameral cefuroxime injection and/or perioperative levofloxacin eyedrops on the incidence of endophthalmitis after phacoemulsification cataract surgery.
10,11By the end of 2005, complete follow-up records had been received for 13,698 study patients. Such a clear beneficial effect from the use of intracameral cefuroxime had been observed that it was agreed it would be unethical to continue the study and to wait for the completion of all follow-up procedures before reporting this important result. If total reported cases of endophthalmitis are considered, the incidence rate observed in those treatment groups not receiving cefuroxime prophylaxis (23 cases in 6,862 patients) was almost five times as high as that in the groups
receiving this treatment (5 cases in 6,836 patients). If only cases proved to be due to infection are considered, the rate was more than 5 times as high in the treatment groups not receiving cefuroxime. Although the use of perioperative levofloxacin eyedrops as prophylaxis was also associated with a reduction in the observed incidence rate of postoperative endophthalmitis, this effect was smaller and was not statistically significant. The study group strongly recommended that intracameral cefuroxime administered at the time of surgery significantly reduced the risk for developing endophthalmitis after cataract surgery.
10By the time of the 2007 report, the study had recruited 16,603 patients. The study was based on a 2 × 2 factorial design, with intracameral cefuroxime and topical perioperative levofloxacin factors resulting in four treatment groups. The comparison of case and noncase data was performed using multivariable logistic regression analyses. Odds ratios (ORs) associated with treatment effects and other risk factors were estimated.
11Twenty-nine patients presented with endophthalmitis, of whom 20 were classified as having proven infective endophthalmitis. The absence of an intracameral cefuroxime prophylactic regimen at 1 mg in 0.1 ml normal saline was associated with a 4.92-fold increase (95% confidence interval [CI], 1.87-12.9) in the risk for total postoperative endophthalmitis. In addition, the use of clear corneal incisions (CCIs) compared to scleral tunnels was associated with a 5.88-fold increase (95% CI, 1.34-25.9) in risk and the use of silicone IOL optic material compared to acrylic with a 3.13-fold increase (95% CI, 1.47-6.67). The presence of surgical complications increased the risk for total endophthalmitis 4.95-fold (95% CI, 1.68-14.6), and more experienced surgeons were more likely to be associated with endophthalmitis cases. When considering only proven infective endophthalmitis cases, the absence of cefuroxime and the use of silicone IOL optic material were significantly associated with an increased risk, and there was evidence that men were more predisposed to infection (OR 2.70; 95% CI, 1.07-6.8)
11 (
Tables 11.1 and
11.2).
Since the release of this data, numerous controversies have been discussed including the risks of administering an incorrect concentration of antibiotic into the eye. The procedure for mixing appropriate dose and volume of cefuroxime can be complex, and incorrect dosing is possible. Errors are rare, but if the incorrect cefuroxime dose is administered, it may have serious consequences for the eye. Furthermore, it was found that the use of topical antibiotics did not seem to offer a prophylactic benefit. Topical agents were not administered postoperatively until the day after surgery, and levofloxacin, a third-generation fluoroquinolone, was employed in this study. Discussions have taken place as to whether or not a fourth-generation fluoroquinolone topical agent could have been more beneficial. Additionally, one should consider if installation of topical antibiotics on the day of surgery, rather than the day after, could have shown a prophylactic effect.
Lastly, generalizability of this data has been discussed. Rates of endophthalmitis, as well as causative organisms, vary throughout the world. Therefore, concern exists as to whether or not the ESCRS data is relevant to parts of the world where baseline rates of endophthalmitis are lower or higher.
Regardless, the ESCRS Study was the largest study of an antibiotic in medical history. The results were impressive and recommendations strong. However, as with any good clinical trial, controversies exist. These mainly revolve around antibiotics chosen, timing of dosing, and applicability of trial data to non-European parts of the world. Currently, approximately one-third to one-half of cataract surgeons around the world employs cefuroxime prophylaxis in cataract surgery.