Evaluation of the Patient
When the first two editions of this book were written, considerable emphasis was placed on the physical aspects of orbital diagnosis. In particular, the overall appearance of the eye and ocular adnexa, careful palpation of the orbit, and precise exophthalmometry were believed to be important in the initial evaluation of the patient. These features, when combined with the analysis of subjective symptoms and other objective findings, enabled an educated guess of the position and size of an assumed orbital mass. This was the first step in an orderly progression leading to a logical decision about the surgical or nonsurgical management of the problem.
When the third edition was written, the discovery, refinement, and sophistication of radiographic imaging shifted orbital diagnosis toward the realm of technology and away from almost sole reliance on ophthalmologic assessment. The wizardry of imaging makes possible such a positive display of most tumors that even the patient can see the putative orbital mass. The latter has been a tremendous help in establishing an effective communication between the physician and patient, a contrast to former times when dialogue was so frequently based on assumption. Orbital imaging is now so refined that either computed tomography scan or magnetic resonance imaging is an absolute necessity in the patient’s workup. However, the clinician should not let these diagnostic tools replace or overshadow the importance of the patient’s anamnesis.
The Story
Allowing the patient to verbalize the reasons for seeking ocular consultation is the first priority. The ophthalmologist should set aside time to be an attentive and patient listener. Usually, the first sentence or initial paragraph of the anamnesis highlights the symptom or sign of disease most important to the patient. This chief complaint should definitely be kept in mind when all the preliminaries of diagnosis are completed and the physician is ready to propose treatment. Is the patient’s main concern a protrusion or displacement of the eye? If so, an “exploratory” orbitotomy, combined with incisional biopsy, may not meet the patient’s expectations of relief because the proptosis may still be noticeable postoperatively. Does the patient seek help principally because of loss of vision or diplopia? Here, the necessary surgical management of the orbital problem is likely to worsen the symptoms temporarily. The patient should be advised of these eventualities. Later, this sort of discussion may help maintain a smooth rapport with the patient if recovery is slow. Is the patient’s problem fundamentally aesthetic, such as marked edema or discoloration of the eyelids or a disturbing redness of the eye? Such features may forewarn a complex set of events requiring a treatment approach that meets the patient’s cosmetic expectations. Finally, the patient may frame the problem as one of pain or headache, as contrasted to the frequent expression of pressure. The latter is but a common manifestation of increased orbital bulk. Relief from pain and headache may require more than one mode of therapy and a greater commitment of time and expense on the part of the patient.
At some point in the evaluation, a discreet inquiry is made about any earlier event that might have a bearing on the current complaint. The patient is usually willing to talk about prior treatment but is often reticent about previous diagnoses. This may enhance the patient’s opinion of the objectivity of the physician’s forthcoming recommendations.
More direct questioning is reasonable if the current complaint is related to previous surgical procedures. Women should be asked about previous breast surgery, although the interval between the surgery and the current orbital disorder may seem too long to be relevant. The possibility of metastasis is always present in such situations. The
same possibility of metastatic disease also exists in elderly men who have undergone surgery of the prostate gland. In either sex, nasal surgery may presage an unsuspected mucocele or carcinoma that first becomes manifest by secondary invasion of the orbit. A prior thyroidectomy should alert the ophthalmologist either to possible orbital sequelae of Graves orbitopathy with asymmetric features or to occult thyroid carcinoma. Finally, previous biopsy findings from small lymph nodes or lumps might be compatible with orbital spread of lymphoma, neurofibroma, melanoma, squamous cell carcinoma, and adenocarcinoma of various origins. Considering the anatomic size of the orbital cavity, the variety of lesions and tumors that select this small space for a second residence is amazing.
same possibility of metastatic disease also exists in elderly men who have undergone surgery of the prostate gland. In either sex, nasal surgery may presage an unsuspected mucocele or carcinoma that first becomes manifest by secondary invasion of the orbit. A prior thyroidectomy should alert the ophthalmologist either to possible orbital sequelae of Graves orbitopathy with asymmetric features or to occult thyroid carcinoma. Finally, previous biopsy findings from small lymph nodes or lumps might be compatible with orbital spread of lymphoma, neurofibroma, melanoma, squamous cell carcinoma, and adenocarcinoma of various origins. Considering the anatomic size of the orbital cavity, the variety of lesions and tumors that select this small space for a second residence is amazing.
Sometimes, in adults, the story is told by a spouse or a close relative of the patient. Here, the descriptive events may reflect only the opinion of the observer and, therefore, lack the subjective input of the patient. Such patients are often less concerned about their orbital problem than the narrator is and may be less responsive to treatment options. If the outcome of treatment is unsatisfactory, these patients may avoid any responsibility for the event with the statement, “I only did what the doctor told me to do.” It may be prudent to defer orbitotomy for a while, unless absolutely necessary, in an adult patient who is mentally competent but does not take an active role in the discussion.
In children, of course, the parent or guardian develops the story. Parents tend to relate the orbital ailment to some previous trauma or minor respiratory illness and to understate the severity and progression of the symptoms. Even direct recall by older children and adolescents may be colored by what they have heard their parents say.
As the interview winds down, keep in mind the patient’s age and the pantheon of tumors for the patient’s age-group. These tumors are listed in Chapter 3.
Pressure, Headache, and Pain
These subjective manifestations of disease are difficult to assess, whatever their cause and wherever their anatomic location. Fortunately, in a very severe form, they are not a common accompaniment of orbital tumors. The pressure sensation and uncomfortable feeling described by some patients are probably caused by increasing orbital bulk secondary to slowly expanding tumors and cysts. A more severe form of pressure sensation is encountered in patients with progressive exophthalmos of Graves orbitopathy, in which edematous extraocular muscles and retrobulbar tissues shove the eye forward against the constraint of retracted eyelids and the tethering effect of the extraocular muscle. These patients usually say the affected eye “feels as though it will pop.” We have seen the most severe forms of this symptom in a few patients whose ocular apparatus ultimately decompensates after a long-standing end-stage bout with an inflammatory tumor. In such patients, the eye of the affected orbit is blind and phthisic, the fibrotic orbital contents are hard and stony, and the pressure sensation is unremitting.
Pain, rather than pressure, from an orbital disorder may also be severe. It tends to be more localized and more or less constant, may have a nocturnal phase, and is not easily alleviated by over-the-counter remedies. If the patient describes the pain as localized to the deep orbit, consider the likelihood of an orbital apex lesion, particularly if there is an associated ocular motility disturbance or dysesthesia in the distribution of the second division of the trigeminal nerve on the side of the affected orbit. Orbital angiitis, an invasive fungal infection, or thrombotic sequelae of an arteriovenous malformation deep in the orbit may mimic this type of pain. A sudden extravasation of blood into the cystic space of a lymphangioma in a child or hemorrhage from a varicocele also fits into this category of pain.
If the pain seems most severe in the nasal or inferior portion of the orbit, think of a possible carcinoma of the ethmoid or maxillary sinus. Numbness of the forehead may accompany infiltration of the supraorbital nerve by a squamous cell carcinoma of the adjacent forehead skin. If the pain is referred to the lateral orbit, be wary of a malignant neoplasm of the lacrimal gland, although such localized pain sometimes accompanies an acute inflammatory process of this structure.
Headache lies somewhere between pressure and pain in intensity, more bothersome than pressure but less severe than pain. It is not easily described by the patient (“the eye just hurts”), is poorly localized, variable in duration and frequency, and often soothed by over-the-counter analgesics. Headache may accompany inflammatory and vasculitic disorders of the orbit sometime during their course. Headache also is a nuisance in patients with orbitocranial meningioma and secondary orbital invasion by a malignant tumor of a paranasal sinus.
Another subjective manifestation that may be the compelling reason for the patient to seek early consultation is “head noise.” The patient is startled by the precipitous onset of noise, most commonly described as swishing or pulsating in type or as being synchronous with the heartbeat. Less frequently, the noise is buzzing, blowing, rushing, pumping, or throbbing in type. The noise may be constant, intermittent, or postural (i.e., when standing, sitting, or lying down). Often, the sound is lateralized to the ipsilateral ear.
This noise is a telltale symptom of vascular malformation in the orbit or the intracranial vault just posterior to the orbit. It tends to be more frequent and intense in traumatic arteriovenous fistulas than in the spontaneous type. Surprisingly, the noise may not be audible on auscultation, particularly in spontaneous arteriovenous fistulas. Patients with a dural arteriovenous shunt seldom note head noise, unless the shunt is large or bilateral in extent. A bruit is heard best by auscultation directly over the front of the eye of the affected orbit with the eyelid closed.
Chronology
The rate of progression and overall duration of the patient’s presentation are of equal importance in diagnosis. In general, the more rapid the progression, the shorter the interval since onset. The literature that addresses these features usually postulates that lesions with a long interval of presentation are benign, whereas orbital disorders of short duration are more likely to be malignant or inflammatory. This overlooks the fact that, among adults, some patients really do not know how long their disorder has been present. Here, prior photographs may be the only proof of an overlooked proptosis of many years’ duration. Such photographs, in some patients, have suggested a duration of 15 to 30 years; but, instead of being benign, such lesions on excision prove to be a malignant degeneration of a long-standing benign process (see Fig. 1.1). A sudden spurt in the amount of proptosis of an otherwise indolent course may also signify the onset of malignancy.
More acute presentations of short duration may also behave contrary to conventional dicta, particularly in children. The child with a bulging eye and red, edematous eyelids of orbital rhabdomyosarcoma of a few days’ duration may look strikingly similar to the child with an inflammatory tumor of similar duration. Both lesions can be equally alarming to the parent. The former lesion is malignant, whereas the latter is benign, although potentially aggressive. The inflammatory lesion is associated with pain, but the malignant lesion creates little, if any, discomfort (see Fig. 1.2). A tissue diagnosis should be obtained quickly in these situations and appropriate treatment started, rather than dithering over whether the lesion is benign or malignant on the basis of its dynamics.
In other cases, the presentation may not be acute, subacute, or chronic but instead may wax and wane—sometimes better, sometimes worse. In adults, this behavior suggests one of the inflammatory tumors. A tumor commonly associated with an episodic course in infants and children may also show episodic features, but the triggering mechanism is often an upper respiratory tract infection. The presentation of a mucocele of frontal or ethmoid sinus origin may also undergo transient changes induced by respiratory-like illness. Overall, the literature tends to overstate the importance of the duration of disease in orbital diagnosis.
 Figure 1.1 Malignant mixed tumor in a 49-year-old man whose prior photographs indicated a slowly progressive displacement of the left eye of 30 years’ duration. The slow progression suggested benignity, but the tumor proved to be a benign mixed tumor that had undergone malignant degeneration. The downward and inward displacement of the eye is usually the result of some lesion of the lacrimal gland fossa. |
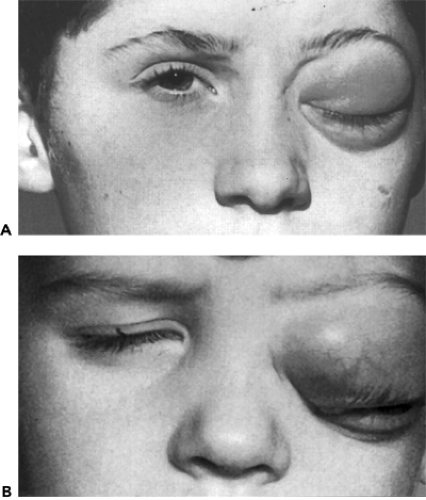 Figure 1.2 Two adolescent males of the same age decade with reddish discoloration, proptosis, and edema of one eyelid of several weeks’ duration. The presence of pain in one patient (A) (vasculitides, left upper eyelid) but the absence of pain in the other patient (B) (rhabdomyosarcoma, left lower eyelid) was a differential point in the presentation of these tumors. (See Color image.) |
Inspection of the Eye and Adnexa
When discussion with the patient is completed and a written summary recorded, an objective assessment of the orbital ailment is next in importance. Inspection of the eye and adnexal structures should include an assessment of the color and texture of the adnexal tissue and the surface of the eye, measurement of the degree of proptosis, a notation of any disparity in the anatomic relationship of the eye and covering eyelids, and palpation of the orbital rim and soft tissue components of the anterior orbit. These examinations, along with a subsequent analysis of ocular function and motility, were once avenues leading to an educated guess about the position and size of an orbital mass and the nature of the putative disorder. Now, principally because of orbital imaging techniques, determination of size, position, and configuration of a
tumor is no longer a guess; it is a reality. Therefore, the once-important alterations of the external eye and adnexa are now more documentary rather than diagnostic in the overall assessment plan.
tumor is no longer a guess; it is a reality. Therefore, the once-important alterations of the external eye and adnexa are now more documentary rather than diagnostic in the overall assessment plan.
Assessment of Proptosis
Exophthalmometry is essential in the initial evaluation of any orbital disorder, although proptosis (forward protrusion) may either not be present or is masked by a droopy or swollen eyelid. In addition, exophthalmometry is important to the patient’s record as a baseline for judging the patient’s course or response to therapy and is a universal standard of reference for any future correspondence pertaining to the orbital problem.
Some combination of proptosis and displacement of the eye was present in approximately 80% of the cases in a 50-year case series. Exophthalmometry was impractical in some cases because of the removal of the eye on the side of the affected orbit, an ulcerating carcinoma of the periorbital area, an orbital deformity secondary to surgery for recurrent sinus carcinoma, or an orbital deformity associated with fibrous dysplasia or massive neurofibromatosis. Enophthalmos, such as occurs with metastatic scirrhous carcinoma of the breast, is present in <1% of cases.
Initially, we used the Hertel exophthalmometer to measure the degree of proptosis. For the last 30 years or so, we have used the Krahn modification of the Hertel instrument. The normal values derived with the Krahn device range from 14 to 21 mm in adults. Any value <14 mm can usually be considered diagnostic of enophthalmos. Values >21 mm are encountered occasionally in individuals with a hereditary tendency for prominent eyes or a moderate degree of myopia. A difference of 2 mm or more in the position of one eye relative to the other is noteworthy. All measurements are subject to variables such as asymmetry of the patient’s face, shifting position of the exophthalmometer, or strabismus of one eye. The physician may use any exophthalmometer that is practical as long as the method of measurement and positioning of the physician in relation to the patient’s eyes are kept constant. In children, the use of an exophthalmometer may not be possible. In such cases, unilateral proptosis may be determined by looking downward over the brow and noting the relative position of the eyes (see Fig. 1.3).
 Figure 1.3 Unilateral proptosis in a 22-month-old girl as viewed from above the eyebrow. This is a practical method for the clinical assessment of proptosis in children. The subtle subcutaneous spread of orbital lymphangioma and neurofibromatosis into the tissues of the eyelid and eyebrow may be more clearly documented with a brow view than with a front face photograph. |
Displacement of the eye, a shift along a plane other than the normal visual axis, accompanies proptosis. Almost without exception, the direction of displacement is opposite the mass effect of an enlarging tumor. Orbital imaging has relegated assessment of displacement to a documentary rather than a diagnostic role.
There are, however, some infrequent exceptions to the tenet that protrusion of the eye is invariably associated with progression of an orbital tumor. Enophthalmos is one of these. Most often, enophthalmos is secondary to the tractive effect of an infiltrative, sclerosing, metastatic carcinoma of orbital soft tissue (see Fig. 1.4). Other tumors with a
similar effect are squamous cell carcinoma of adnexal origin and Wegener granulomatosis. Enophthalmos may also be secondary to fat atrophy associated with orbital varix or long-standing firm tumors such as cavernous hemangioma and neurofibroma. In these situations, the vertical width of the palpebral fissure may appear normal, but the upper eyelid sulcus is deep and sunken posteriorly.
similar effect are squamous cell carcinoma of adnexal origin and Wegener granulomatosis. Enophthalmos may also be secondary to fat atrophy associated with orbital varix or long-standing firm tumors such as cavernous hemangioma and neurofibroma. In these situations, the vertical width of the palpebral fissure may appear normal, but the upper eyelid sulcus is deep and sunken posteriorly.
 Figure 1.4 Metastatic adenocarcinoma in a 45-year-old woman with blepharoptosis, deepening of the upper lid sulcus, and enophthalmos (5 mm) of the right eye of 3 months’ duration. These were first manifestations of metastasis from carcinoma of the breast removed 4 years previously. |
 Figure 1.5 A 53-year-old woman with slowly progressive prominence of the left eye since birth had visual acuity of counting fingers, Krahn exophthalmometer readings of R 17 mm and L 20 mm, and high myopia of 20 diopters.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|