Purpose
To evaluate the safety and effectiveness of the aspheric diffractive Tecnis multifocal ZM900 (TCMF) intraocular lens (IOL; Abbott Medical Optics, Inc, Santa Ana, California, USA).
Design
One-year, nonrandomized, multicenter, evaluator-masked, bilateral, parallel-group comparative clinical evaluation.
Methods
Subjects underwent bilateral implantation with the TCMF IOL or the CeeOn 911A monofocal (CEMN) IOL (Abbott Medical Optics, Inc) according to subject preference.
Results
One-year results were available for 244 eyes of 125 TCMF IOL subjects and for 245 eyes of 123 CEMN IOL subjects. Mean distance visual acuities (VAs) were statistically and clinically equivalent between the 2 groups. Mean binocular and monocular uncorrected and distance-corrected near VAs were significantly better for the TCMF IOL versus the CEMN IOL group ( P < .0001). A greater proportion of TCMF IOL versus CEMN IOL subjects achieved binocular combined VAs of 20/25 distance and 20/32 near (84.2% [96/114] vs 6.2% [7/113]; P < .0001). The TCMF IOL group had excellent depth of focus, maintaining a mean of 20/40 or better for far, intermediate, and near distances. Mean contrast sensitivity scores were lower for the TCMF IOL versus the CEMN IOL group, but the differences were not considered clinically significant. Halos and night glare were more common in the TCMF IOL versus the CEMN IOL groups. Both reading acuity (20/20 vs 20/47; P < .0007) and speed (148 vs 117 words/minute; P < .0001) were significantly better for the TCMF IOL versus the CEMN IOL group, as were the proportions of the TCMF IOL group versus the CEMN IOL group that achieved spectacle independence (84.8% vs 5.2%; P < .0001) and that functioned comfortably at near without glasses (96.4% vs 30.4%; P < .0001).
Conclusions
The TCMF IOL provided enhanced near VA, reading acuity per speed, depth of focus, and spectacle independence compared with the monofocal IOL.
Consistent advances in cataract surgical techniques and devices have raised patients’ postoperative expectations from good best-corrected distance visual acuity (BCDVA) to excellent uncorrected distance visual acuity (UCDVA). Having achieved this goal, cataract surgeons are now striving to improve patients’ postsurgical quality of life by providing good functional uncorrected postoperative visual acuity at both distance and near. The first step toward this goal was the development of the multifocal intraocular lens (IOL).
Multifocal IOLs use diffractive or refractive optics to produce 2 or more foci for far, near, and sometimes, intermediate vision. Clinical studies to date demonstrate that subjects successfully learn to attend to the in-focus image and disregard the out-of-focus image(s) produced by multifocal IOLs. In a review of multifocal IOL studies, it was concluded that multifocal IOLs improve near visual acuity without significant degradation of distance visual acuity as compared with monofocal IOLs.
Although multifocal IOLs are the only type of IOLs indicated to provide 2.6 to 3.0 diopters (D) of add in the spectacle plane (3.0 to 4.0 D of add in the IOL plane), the splitting of light to multiple foci and the simultaneous in- and out-of-focus images can cause some decrease in contrast sensitivity and may increase the likelihood of experiencing halos and glare compared with traditional monofocal IOLs. An aspheric IOL design improves contrast sensitivity by reducing or canceling the normal positive spherical aberration of the cornea. Improved quality of vision is seen with monofocal aspheric IOL designs. An aspheric multifocal IOL design may reduce the incidence and severity of halo and glare seen with multifocal IOLs. Multifocal IOLs are a success when these drawbacks are more than compensated for by the improvement in range of visual function. Thus, measures of patient satisfaction, although subjective, become very important in determining the effectiveness of a multifocal IOL.
A 2-phase, controlled clinical trial comparing the Tecnis Aspheric Multifocal (TCMF) IOL with the monofocal CeeOn 911A (CEMN) IOL (both from Abbott Medical Optics, Inc, Santa Ana, California, USA) was performed to assess the performance of the TCMF IOL. Results for the first cohort of subjects who completed the 1-year study evaluation are presented here, highlighting measures of visual acuity, quality of vision, and patient satisfaction.
Methods
The initial study phase was a nonrandomized, evaluator-masked, bilateral, comparative, 1-year assessment of the TCMF and the CEMN IOLs. Each patient provided written informed consent for the study before any study procedures were performed. Because not all cataract patients are appropriate candidates for multifocal IOLs, subjects were counseled as to the benefits and drawbacks of each lens and were allowed to choose which type of implant (multifocal or monofocal) they preferred.
Subjects enrolled in the study were at least 18 years of age and had visually significant cataracts in both eyes. Inclusion criteria included naturally dilated pupils of 4.0 mm or more in dim light and 1.0 D or less of corneal astigmatism. Subjects were excluded if they used systemic or ocular medications that may affect vision, had any systemic or ocular condition that would increase the operative risk or confound the outcome(s) of the study, or required an intraocular lens of less than 15.0 D or more than 26.0 D.
The TCMF IOL used in this study is a second-generation silicone multifocal IOL with a diffractive zone across the posterior surface of the 6.0-mm optic that provides a far and a near focal point that are 4.0 D apart. The lens has the same aspheric, modified prolate design on the anterior surface as the TCMF IOL. The CEMN IOL is a traditional, spherical, monofocal IOL of the same material, haptic, and edge design as the TCMF IOL.
The investigators used their standard small-incision phacoemulsification cataract extraction surgical techniques. Pre-existing keratometric astigmatism was managed by incision site placement only. No additional refractive procedures were allowed during the study period. All eyes were targeted for emmetropia.
Visual acuities were measured with 100% contrast Early Treatment Diabetic Retinopathy Study acuity charts. Distance visual acuities were tested at 4 m; near visual acuities were tested at a fixed distance of 33 cm as well as at each subject’s preferred distance (best distance). Binocular best-corrected distance defocus visual acuity was tested in −0.5-D increments from 0 to −5 D defocus using a 100% contrast Early Treatment Diabetic Retinopathy Study chart. Binocular best-corrected distance contrast sensitivities were evaluated with Functional Acuity Contrast Test sine wave grating charts with the self-illuminated and self-calibrated Optec 6500 Vision Tester (StereoOptical Co, Chicago, Illinois, USA) under photopic and mesopic conditions. Photopic testing was at 85 cd/m 2 , mesopic testing was at 3 cd/m 2 . All test results were adjusted mathematically for the test distances used, and logarithm of the minimal angle of resolution visual acuities were converted to Snellen equivalents for presentation. Binocular reading acuity and speed were assessed with MNREAD continuous-text acuity charts (Lighthouse Low Vision Products, Long Island City, New York, USA) with distance correction in place at the subject’s best distance. Contrast sensitivity, reading ability, and defocus testing were performed only at 4 to 6 months after surgery. Questionnaires assessing functional vision and patient satisfaction were administered over the phone by a trained individual who was masked as to the IOL implanted.
Comparisons between IOL groups for categorical data such as gender, race, preoperative acuity, and so forth were performed using the Fisher exact test. Comparisons between IOL groups for age were performed using 2-sample t -tests. For uncorrected near visual acuity (UCNVA), distance-corrected near visual acuity (DCNVA), reading acuity, reading speed, defocus, and optical visual symptoms, all results were compared between IOL groups using the Wilcoxon rank-sum test. For distance visual acuity data, a nonequivalence approach using 90% confidence intervals was used to determine if the mean for multifocal eyes was within 1 line of the mean for monofocal eyes. Unless otherwise indicated, 2-sided testing was performed with α set at 0.05.
Results
A total of 248 subjects were implanted across 13 sites in the United States between November 29, 2004, and December 21, 2005. The TCMF IOL was implanted in 244 eyes of 125 subjects; the CEMN IOL was implanted in 245 eyes of 123 subjects. One-year data as of February 27, 2007, were available from 94.4% (118/125) of TCMF IOL subjects and from 94.3% (116/123) of CEMN IOL subjects. Seven TCMF IOL subjects were not included in this analysis because of declining to participate further (n = 2), lens explantation (n = 1), death (n = 1), loss to follow-up (n = 1), and lack of 1 year bilateral data because of delayed implantation of the second eye (n = 2). Seven CEMN IOL subjects were not included because of declining to participate further (n = 3), death (n = 1), illness (n = 2), and loss to follow-up (n = 1).
Mean age was 66.4 ± 9.1 years for the TCMF IOL group and 68.7 ± 8.9 years for the CEMN IOL group. Although statistically significant ( P = .0458), the difference in mean age of 2.3 years was not clinically significant. Most of each group were white (TCMF, 100%; CEMN, 92.7%) and predominantly female (TCMF, 63.2%; CEMN, 65.9%). For most eyes, preoperative pupil size was at least 4 mm under photopic conditions and from 4 to 5 mm under mesopic conditions. All monocular results presented are for first eyes.
Additional surgical procedures or complications were rare for either lens group. There were 3 lens-related secondary surgical interventions in a single TCMF subject who underwent a pupilloplasty and bilateral lens explantation. In this subject, there was a misalignment of less than 0.5 mm between the IOL and the dilated pupil because of a slight difference in anatomic position. Pupilloplasty was undertaken in 1 eye in an effort to alleviate halos and glare, but ultimately both eyes underwent lens exchange for a monofocal IOL. Four lenses were exchanged in the TCMF IOL group: 3 because of errors in refractive power, and 1 because of implantation of an incorrect lens. There were no lens explantations or exchanges in the CEMN IOL group. Neodymium:yttrium–aluminum–garnet capsulotomy was performed on 12.8% (16/125) of TCMF IOL and 4.9% (6/123) of CEMN IOL first eyes ( P = .0425).
There were no significant differences in postoperative photopic or mesopic pupil size, spherical equivalent correction achieved, or absolute postoperative cylinder between the 2 groups. Mean postoperative spherical equivalents were within 0.25 D of plano (TCMF IOL, 0.02 ± 0.49 D; CEMN IOL, −0.17 ± 0.47 D). Mean deviation from the targeted refraction (emmetropia) was similar for the 2 groups (TCMF IOL, 0.08 ± 0.49; CEMN IOL, −0.02 ± 0.49; P = .12).
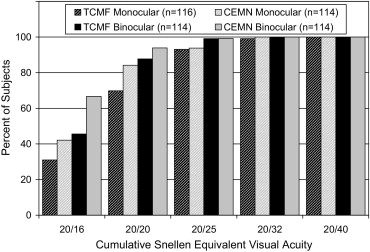
At 1 year, based on confidence interval analyses, the 2 groups were equivalent (defined as a difference of less than 1 Snellen line) for mean monocular (TCMF 6.53 ± 1.55 [20/28]; CEMN 7.21 ± 1.34 [20/24]) and binocular (TCMF IOL, 7.54 ± 0.94 [20/22]; CEMN IOL, 7.98 ± 1.06 [20/20]) UCDVA as well as monocular (TCMF IOL, 7.87 ± 0.90 [20/21]; CEMN IOL, 8.17 ± 0.88 [20/19]) and binocular (TCMF IOL, 8.35 ± 0.82 [20/18]; CEMN IOL, 8.68 ± 0.78 [20/17]) BCDVA. All subjects in both lens groups achieved a binocular UCDVA of 20/40 or better; however, more CEMN IOL subjects achieved binocular UCDVA of 20/20 or better (77.2%; 88/114) compared with TCMF IOL subjects (57.9% [66/114]; Figure 1 ). All subjects in both groups achieved monocular and binocular BCDVA of 20/40 or better; additionally, the same proportions of subjects in both lens groups achieved monocular and binocular BCDVA of 20/25. A slightly higher percentage of subjects achieved monocular and binocular BCDVA of 20/20 or better in the CEMN IOL group compared with the TCMF IOL group ( Figure 2 ).
Monocular and binocular UCNVA and DCNVA were tested at 33 cm, the theoretical best test distance for the TCMF IOL, and at the subject’s best near distance. In all comparisons, the mean score for the TCMF IOL group was significantly better ( P < .0001) than that of the CEMN IOL group by approximately 4 to 5 lines of near acuity ( Table 1 ).
| Near Visual Acuity | Photopic UCNVA | Photopic DCNVA | Mesopic DCNVA | |||
|---|---|---|---|---|---|---|
| TCMF | CEMN | TCMF | CEMN | TCMF | CEMN | |
| Monocular 33 cm | 11.9 ± 1.6 (20/32) | 7.7 ± 1.8 (20/84) | 12.5 ± 1.2 (20/28) | 7.6 ± 1.7 (20/87) | 10.1 ± 1.8 (20/50) | 5.9 ± 1.6 (20/130) |
| Monocular best distance | 12.3 ± 1.4 (20/29) | 8.2 ± 2.0 (20/76) | 12.8 ± 1.2 (20/26) | 8.0 ± 1.8 (20/80) | 10.5 ± 1.9 (20/45) | 6.2 ± 1.8 (20/120) |
| Binocular 33 cm | 13.0 ± 1.0 (20/25) | 9.0 ± 1.8 (20/63) | 13.2 ± 1.0 (20/24) | 8.6 ± 1.6 (20/70) | 11.1 ± 1.5 (20/39) | 6.8 ± 1.7 (20/104) |
| Binocular best distance | 13.1 ± 1.0 (20/24) | 9.5 ± 2.0 (20/57) | 13.4 ± 1.0 (20/23) | 8.9 ± 1.6 (20/64) | 11.3 ± 1.5 (20/37) | 7.1 ± 1.8 (20/99) |
The percentage of subjects achieving better binocular UCNVA and DCNVA scores at both 33 cm and at best distance was substantially greater in the TCMF IOL group compared with the CEMN IOL group ( Figure 3 ). With near add in place, there was no significant difference between the groups in mean best-corrected near acuity at best distance ( P = .1167).
The proportion of subjects achieving binocular combined visual acuities of 20/40 distance and 20/40 near (> 98% for TCMF IOL vs < 22% for CEMN IOL) or 20/25 distance and 20/32 near (> 84% for TCMF IOL vs < 7% for CEMN IOL) at 33 cm was significantly greater ( P < .0001) for the TCMF IOL group than the CEMN IOL group for both UCNVA and DCNVA ( Figure 4 ).
The depth-of-focus curves for the TCMF and CEMN IOL groups are shown in Figure 5 . Mean visual acuity for the TCMF IOL group remained at 20/40 or better for far, intermediate, and near distances, through −4 D of defocus. Mean visual acuity for the CEMN IOL group was similar to that of the TCMF IOL group through −1.5 D of defocus, then decreased steadily as defocus increased. Regardless of pupil size, mean visual acuity in the TCMF IOL group typically remained 20/40 or better through far, intermediate, and near distances ( Figure 6 ).
Mean contrast sensitivity scores were lower for the TCMF IOL group compared with the CEMN IOL group under all lighting conditions ( Figure 7 ). However, the mean difference between lens groups did not reach clinical significance (generally regarded as 0.30 log units) under any test condition.
With distance correction in place, the TCMF IOL group read text of a significantly smaller print size ( P < .0001) than the CEMN IOL group at best distance. The smallest print size read for the TCMF IOL group was equivalent to a Snellen score of 20/20, compared with 20/47 for the CEMN IOL group. Reading speed also was significantly better for the TCMF IOL group ( P = .0007), reading 148 words per minute at a smaller critical print size of Snellen 20/30 compared with 117 words per minute at Snellen 20/63 for the CEMN IOL group.
For each eye, subjects were asked by investigators if they were having any difficulties with their vision. At 1 year, night glare (15.5% [18/116]) and halos (22.4% [26/116]) were the most frequently reported symptoms for the TCMF IOL group (first eye). Most reports of night glare were moderate (10.3% [12/116]), and only 2.6% (3/116) were severe. Most halos were rated as mild (12.1% [14/116]), with 5.2% (6/116) reported as moderate and 5.2% (6/116) reported as severe. For CEMN IOL first eyes, the most reported optical or visual symptom at 1 year also was halos (8.6% [10/116]), with most reports being mild in severity. Night glare was reported by 4.3% (5/116) CEMN IOL subjects.
At 1 year, the great majority of subjects were satisfied with their lens choice: 94.6% (106/112) of TCMF IOL subjects and 89.6% (103/115) of CEMN IOL subjects reported they would elect the same IOL again. The most common reason for not electing the same IOL again was poor near vision, all from CEMN IOL subjects. The mean rating of vision without spectacles (on a scale of 1 to 10) was significantly better ( P < .0001) for the TCMF IOL group (8.9 ± 1.4) than the CEMN IOL group (7.9 ± 2.0).
Spectacle independence was significantly greater for the TCMF IOL compared with the CEMN IOL group (84.8% [95/112] vs 5.2% [6/115]; P < .0001; Table 2 ). Subjects also reported if they were able to function comfortably at near (TCMF, 96.4% [108/112]; CEMN, 30.4% [35/115]), intermediate (TCMF, 93.8% [105/112]; CEMN, 84.2% [96/115]), or far (TCMF, 96.4% [108/112]; CEMN, 98.3% [113/115]) distances without spectacles. A significantly greater proportion of the TCMF IOL group were able to function comfortably at near ( P < .001) and intermediate ( P = .0324) distances compared with the CEMN IOL group. There was no significant difference between the 2 groups in their ability to function comfortably at far distances ( P = .4417).



