Purpose
To determine the ability of anterior segment optical coherence tomography (OCT) to detect intraocular lens (IOL) tilt evaluation in relation to the limbus.
Design
Observational case series.
Methods
The IOL position of 123 eyes of 92 patients was examined with anterior segment OCT (Carl Zeiss Meditec, Dublin, California, USA). All eyes underwent uneventful phacoemulsification with the IOL in the bag. Images were obtained in 4 axes (180 to 0 degrees, 225 to 45 degrees, 315 to 135 degrees, and 270 to 90 degrees). Using MatLab software version 7.1 (Mathworks), the OCT images were analyzed. The distance between the iris margin and the anterior surface of IOL, the slope ratio between IOL and limbus, and the angle (θ; position of IOL with reference to the limbus) were determined and were correlated with the astigmatism and vision.
Results
The mean slope of the limbus and the IOL in all axes was 0.003 ± 0.09 and −0.002 ± 0.12, respectively. The average slope ratio was 1.1 ± 1 (range, −2.09 to 3.82) and the angle (θ) was 1.52 ± 0.9 degrees (range, 0.04 to 3.6 degrees). The mean ocular residual astigmatism was 0.2379 ± 0.469 diopters. There was no significant correlation of ocular residual astigmatism with slope ratio ( r = −0.171; P = .060) and slope angle ( r = −0.132; P = .147). There was significant correlation of ocular residual astigmatism with total astigmatism (r=0.602, p=0.000). The mean distances between the iris margin and the anterior surface of IOL at the pupillary plane were 0.80 ± 0.6 mm and 0.83 ± 0.57 mm, respectively.
Conclusions
The normal in-the-bag IOL maintains an angle with reference to the limbus and a slope ratio without causing a significant tilt. Anterior segment OCT can be used as an alternative in IOL tilt evaluation by the analysis of its position in relation to the limbus.
The accurate position of an intraocular lens (IOL) in the capsular bag is vital in preventing postoperative tilt and astigmatism. IOL tilt is one of the components of malposition that can lead to astigmatism, change in optical higher-order aberrations, and loss of best-corrected visual acuity. Ultrasound biomicroscopy, Scheimpflug images, Purkinje reflections, photographic documentation, anterior segment analysis system are the methods used for evaluation of IOL position. Although anterior segment optical coherence tomography (OCT) has been used to image the IOL position, there are no reports of postoperative IOL tilt estimation with OCT in a large population. This study used anterior segment OCT to evaluate the position of IOLs implanted within the capsular bag after uneventful phacoemulsification and correlated the results with visual acuity and refractive outcomes.
Methods
The study included 123 eyes of 92 patients who underwent uneventful phacoemulsification with the IOL in the capsular bag. The inclusion criterion was receipt of an in-the-bag fixated IOL after uneventful phacoemulsification, and the exclusion criterion was complicated cataract surgery with posterior capsular rent or after neodymium:yttrium–aluminum–garnet capsulotomy. Patients were taken randomly (every fifth patient from the postoperative clinic 6 months after surgery), and thereby selection bias was decreased.
The IOL types were as follows: the single-piece, foldable hydrophilic acrylic IOL (6-mm optic, 12.5-mm overall length; Appasamy Associates, Chennai, India), single-piece foldable acrylic IOL (6-mm optic, 10.7-mm overall length, Akreos; Bausch & Lomb, Rochester, New York, USA), and a single-piece, nonfoldable polymethyl methacrylate (PMMA) IOL (6.5-mm optic, 13-mm overall length; Appasamy Associates). The pupils were dilated with 0.5% tropicamide and images were obtained in mesopic illumination. The headrest and chin rest of the OCT were adjusted to guarantee a perpendicular position of the patient’s head for each examination. Cross-sectional imaging of the IOL was carried out with the Visante anterior segment OCT (Carl Zeiss Meditec, Dublin, California, USA). The anterior segment single-scan mode was used. Images were obtained in 4 axes, namely 180 to 0 degrees, 225 to 45 degrees, 315 to 135 degrees, and 270 to 90 degrees. The optics of the IOL were imaged with reference to the position of iris, limbus, and capsule.
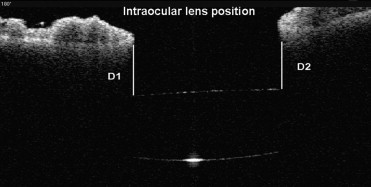
The images then were analyzed with the caliper tools in the software of the anterior segment OCT for iris vault (distance in millimeters between the iris margin and the anterior surface of the IOL at the pupillary plane [D1, D2]; Figure 1 ). Using MatLab software version 7.1 (Mathworks, Natick, Massachusetts, USA), anterior segment single scan images were analyzed. A straight line (L) passing through the limbus on either side of the image was marked as the reference line. A second line (1) passing through the horizontal axis of the IOL ( Figure 2 ) was marked. The horizontal axis of the IOL was determined by the following method. The image from OCT was converted to binary for subsequent extraction of edge coordinates. The selected points on the anterior and posterior arc edges of IOL were obtained. The mathematical representation to fit the anterior and posterior arc of IOL was derived from the equation of the circles passing through the given points ( Figure 2 ). The intersection points of the 2 circles were joined to form the horizontal axis of the IOL. This was executed in all the 4 quadrants (180 to 0 degrees, 225 to 45 degrees, 315 to 135 degrees, and 270 to 90 degrees) in all the eyes. The slopes were calculated for both the straight lines (L,1).
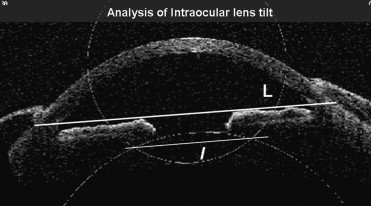
When the reference line along the limbus and the IOL optic were parallel, the optic was not considered to be tilted. The angle (θ) in degrees between the 2 lines (L and 1) was determined. The slope ratio was calculated by dividing the slope of IOL by the slope of the limbus. Corneal topography was examined with Orbscan (Bausch & Lomb). All patients underwent refraction and retinoscopy. The best spectacle-corrected visual acuity was determined with Snellen distant vision acuity charts. Ocular residual astigmatism (ORA) using the method of Alpins and Goggin was determined, and graphical correlation was performed.
Statistical Analysis
Data was entered in a Microsoft Excel worksheet (Microsoft Corp, Redmond, Washington, USA) and was analyzed using SPSS software version 16.1 (SPSS, Inc, Chicago, Illinois, USA). Differences were considered statistically significant at P < .05. Bonferroni correction was conducted to minimize the errors in multiple comparison tests.
Results
One hundred twenty-three eyes of 92 patients were evaluated in the study. The mean time between the date of surgery and the date of OCT imaging was 6 ± 1.2 months. The calculated mean slope in all axes of limbus (L) and the IOL (1) as seen with the OCT was 0.003 ± 0.09 and −0.002 ± 0.12 ( Figure 3 ). Of the 4 axes, the 180- to 0-degree axis showed the IOL contour completely in all 123 eyes ( Figure 4 ). The average values of all parameters are given in Table 1 . The mean slope ratio was 1.1 ± 1 (range, −2.09 to 3.82). The mean distance D1 was 0.80 ± 0.6 mm and the mean distance D2 was 0.83 ± 0.57 mm. There was no significant correlation between slope ratio and D1 ( r = 0.109; P = .123) or D2 ( r = 0.081; P = .371; Figure 5 ). The mean slope angle (θ) between the limbus and the IOL was 1.52 ± 0.9 degrees (range, 0.04 to 3.6 degrees).
| Mean ± SD (n = 123) | |
|---|---|
| Slope of IOL | –0.002 ± 0.12 |
| Slope of limbus | 0.003 ± 0.09 |
| Slope ratio | 1.1 ± 1.0 |
| Angle (θ) with reference to the limbus (in degrees) | 1.52 ± 0.9 |
| Iris vault D1 (mm) | 0.80 ± 0.6 |
| Iris vault D2 (mm) | 0.83 ± 0.57 |
The mean postoperative sphere and total astigmatism (total manifest cylinder in the corneal plane) was 0.21 ± 1.2 diopters (D) and 0.88 ± 1.2 D, respectively. The corneal astigmatism resulting from corneal topography was 0.64 ± 0.86 D. There was no significant correlation between the total astigmatism and the slope ratio ( r = −0.027; P = .766) or the angle (θ; r = −0.057; P = .530). The mean ORA was 0.2379 ± 0.469 D. There was no significant correlation (Pearson correlation coefficient) of ORA ( Figure 6 ) with slope ratio ( r = −0.171; P = .060) and slope angle ( r = −0.132; P = .147). However, there was a significant correlation of ORA with total astigmatism ( Figure 7 ; r = 0.602; P = .000) than with corneal astigmatism ( r = 0.447; P = .00), as seen by the higher r value. There was no significant correlation between ORA and postoperative best-corrected visual acuity ( r = −0.039; P = .669).
There were 3 groups of IOLs, namely, a single-piece acrylic IOL (Appasamy Associates), a single-piece foldable acrylic IOL (Akreos; Bausch & Lomb), and a single-piece PMMA IOL (Appasamy Associates). Bonferroni correction was conducted to minimize the errors in multiple comparison tests. There was no significant difference among the IOL groups with respect to the slope ratio ( P = .431, Kruskal-Wallis test), postoperative vision ( P = .935), and angle (θ; P = .333).
In dividing the 123 eyes based on postoperative vision, 3 groups, namely, best spectacle-corrected visual acuity 20/20 or better, 20/30, and 20/40 or worse ( Table 2 ) were identified. Bonferroni correction was conducted to minimize the errors in multiple comparison tests. There was no significant difference between the 3 groups in ORA ( P = .073, Kruskal-Wallis test). There was a significant difference between the 3 groups with respect to D1 ( P = .033, Kruskal-Wallis test) and D2 ( P = .000). Eyes with 20/20 or better best spectacle-corrected visual acuity had tendency to show higher mean D1 and D2 ( Table 2 ). However, there was no significant difference between the 3 groups with respect to slope of limbus ( P = .114) or slope of IOL ( P = .098). There were 61 eyes with unilateral and 31 eyes with bilateral pseudophakia. There was no significant difference (Mann –Whitney U test) noted between unilateral and bilateral eyes in total astigmatism ( P = .658), ocular residual astigmatism ( P = .837), slope ratio ( P = .636), and angle (θ; P = .524). Posterior capsular opacity was seen in 15 of 123 eyes and was higher in the PMMA group. Pigment dispersion on the IOL was seen in 1 eye. Prominent IOL reflection was seen in the eyes with thick posterior capsular opacification or multiple pigment dispersion on the optic.



