Squamous cell carcinoma of the oral cavity (SCCOC) and squamous cell carcinoma of the oropharynx (SCCOP) represent two distinct disease entities. SCCOC continues to be related to tobacco risk factors, and the current anatomic staging system provides useful prognostic value. Most patients with SCCOP in Western countries now have HPV-associated tumors, and tumor HPV status is considered the most important prognostic factor. Smoking status is emerging as an important prognostic factor for HPV-driven SCCOP, independent of tumor HPV status. Sentinel lymph node biopsy and FDG-PET/CT imaging are diagnostic staging tools useful in select patients with SCCOC and SCCOP.
| FNA | Fine needle aspiration biopsy |
| FDG-PET/CT | Fluorodeoxyglucose positron emission tomography/computed tomography |
| HPV | Human papillomavirus |
| SCCOC | Squamous cell carcinoma of oral cavity |
| SCCOP | Squamous cell carcinoma of oropharynx |
| SNB | Sentinel lymph node biopsy |
| TROG | Trans Tasman Radiation Oncology Group |
Key points
- •
Squamous cell carcinoma of the oral cavity (SCCOC) and squamous cell carcinoma of the oropharynx (SCCOP) represent two distinct disease entities.
- •
A clinical profile has emerged for the patient with an human papillomavirus (HPV)–associated SCCOP as typically a middle-aged, white male, without heavy tobacco history.
- •
The American Joint Committee on Cancer tumor, node, metastasis staging system has useful prognostic significance for SCCOC, but it does not include important prognostic histopathologic factors including tumor thickness, perineural invasion, lymphatic invasion, and extracapsular extension.
- •
Most patients with SCCOP in Western countries have HPV-associated tumors; tumor HPV status is one of the most important prognostic factors for these patients. Smoking status is emerging as an important prognostic factor for HPV-driven SCCOP, independent of tumor HPV status.
- •
For SCCOP, tumor HPV status and smoking status may have greater prognostic significance than traditional anatomic TNM staging; it is likely that future iterations of the AJCC TNM staging system will incorporate tumor HPV and/or p16 status, and perhaps smoking history.
- •
For patients with SCCOC with risk factors for occult lymph node metastases, the gold standard for treatment of the clinically node-negative neck remains an elective neck dissection. However, sentinel lymph node biopsy has been shown to be an effective clinical staging tool that may obviate an elective neck dissection in some patients.
- •
FDG-PET/CT imaging is useful in select patients with unknown primary squamous cell carcinoma of the head and neck (SCCHN), and in some patients with advanced SCCHN at high risk for distant metastases.
Introduction
As discussed elsewhere in this issue, it has become increasingly clear over the last several decades that squamous cell carcinoma (SCC) of the oral cavity (SCCOC) and SCC of the oropharynx (SCCOP) generally represent two different disease entities, with differing causes, prognosis, and response to treatment. The emergence and recognition of human papillomavirus (HPV) as the causative agent in most SCCOP over the last 2 decades necessitates separate discussion of SCCOC and SCCOP in terms of evaluation and staging. This article discusses evaluation and staging of these two distinct diseases, including a discussion of 2 novel diagnostic approaches: sentinel lymph node biopsy (SLNB) and fluorodeoxyglucose (FDG) positron emission tomography (PET)/computed tomography (CT) imaging.
Introduction
As discussed elsewhere in this issue, it has become increasingly clear over the last several decades that squamous cell carcinoma (SCC) of the oral cavity (SCCOC) and SCC of the oropharynx (SCCOP) generally represent two different disease entities, with differing causes, prognosis, and response to treatment. The emergence and recognition of human papillomavirus (HPV) as the causative agent in most SCCOP over the last 2 decades necessitates separate discussion of SCCOC and SCCOP in terms of evaluation and staging. This article discusses evaluation and staging of these two distinct diseases, including a discussion of 2 novel diagnostic approaches: sentinel lymph node biopsy (SLNB) and fluorodeoxyglucose (FDG) positron emission tomography (PET)/computed tomography (CT) imaging.
Diagnosis and evaluation of SCCOC
SCCOC generally presents with a painful oral lesion, although other presenting symptoms include a painful or bleeding ulcer, loose teeth or ill-fitting dentures, trismus (caused by pterygoid involvement), hypoesthesia (caused by perineural involvement), or otalgia (referred pain from the ninth and 10th cranial nerves). Evaluation of SCCOC should include a thorough history and physical examination, dental evaluation, and cross-sectional imaging (CT or magnetic resonance imaging [MRI]). Tissue biopsy, which can generally be performed with local anesthesia in the clinic, is essential to both confirm the suspected diagnosis and to provide prognostic information such as tumor thickness and perineural invasion, which further direct diagnostic evaluation and treatment. A good history should take into account the traditional risk factors for SCCOC (including tobacco, alcohol, and betel nut or pan chewing), family history, and a thorough dental history including a history of caries, extractions, and dentures. Multiple independent studies suggest that HPV does not often play a role in the pathogenesis of SCCOC, with an incidence of high-risk HPV type 16 identified in less than 3% of cases.
A chest radiograph should routinely be performed to assess for distant metastases or second primary malignancies. CT scan is the typical cross-sectional imaging modality used for SCCOC, because it allows the best assessment of extent of both soft tissue and bony involvement. MRI may be used in conjunction or in place of CT, and can be beneficial in cases in which there is suspected perineural invasion along the inferior alveolar or greater palatine nerves, in cases in which dental amalgams result in CT artifact, and in cases in which better delineation of potential base of tongue invasion is desired. Ultrasound with fine-needle aspiration (FNA) biopsy can be used to evaluate lymph nodes that are equivocal on cross-sectional imaging. The role of FDG-PET/CT in the initial evaluation and staging of SCCOC and SCCOP is discussed later.
Diagnosis and evaluation of SCCOP
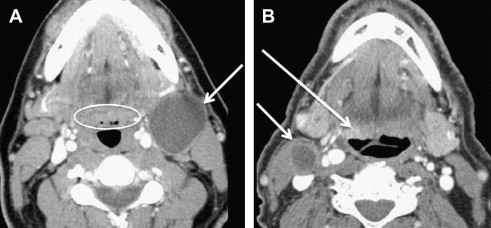
Considerations in the diagnosis and evaluation of SCCOP have changed over the last decade because of the emergence of HPV, which now may account for greater than 80% of SCCOP in Western countries. A clinical profile has emerged for the patient with an HPV-associated SCCOP as typically a middle-aged, white male, without a heavy tobacco history. Patients with HPV-associated SCCOP often present with a painless neck mass that is often cystic on cross-sectional imaging and can be easily confused and misdiagnosed as a second branchial cleft cyst ( Fig. 1 ). Often these patients are otherwise asymptomatic, with a small or occult tonsil or base of tongue painless tumor. Therefore, a middle-aged or elderly person who presents with a cystic neck mass in levels 2 or 3 of the neck should be considered an SCCOP until proved otherwise. Initial diagnostic evaluation of a middle-aged or elderly person with a cystic neck mass should include a thorough head and neck examination, focusing on the lymphoepithelial tissue of the tonsils and base of tongue; cross-sectional imaging; and FNA of the neck mass, with or without ultrasound guidance. If the all of these studies are negative for evidence of SCCOP, FNA biopsy may be repeated, or the patient may be taken to the operating room for an examination under anesthesia with panendoscopy and tonsillectomy. If an examination under anesthesia and frozen section analysis fail to reveal an SCCOP, an excisional biopsy of the neck mass may be performed. However, frozen section should be performed, and the surgeon should be prepared to complete the neck dissection if frozen section analysis of the neck mass confirms SCC.
Patients with SCCOP, or SCC found in a neck lymph node without obvious primary site of disease, should have the FNA or open biopsy specimen evaluated for HPV. In many academic centers, HPV testing is performed by a combination of p16 protein immunohistochemistry (highly sensitive, but not highly specific for HPV) and HPV DNA detection by in situ hybridization (highly specific, but not highly sensitive for HPV). Polymerase chain reaction (PCR)–based amplification can be substituted for in situ hybridization as a method of HPV detection. In some cases, if there is strong and uniform p16 protein immunohistochemistry, the known presence of an oropharyngeal tumor, and typical HPV histomorphology, HPV confirmatory DNA detection with in situ hybridization or PCR-based amplification can be omitted. Cytopathologic specimens from FNA in patients with a potential SCCOP should ideally be handled by a histopathology laboratory familiar with HPV testing techniques, because HPV testing often cannot be retrospectively performed from FNA smears.
Prognostic staging for SCCOC
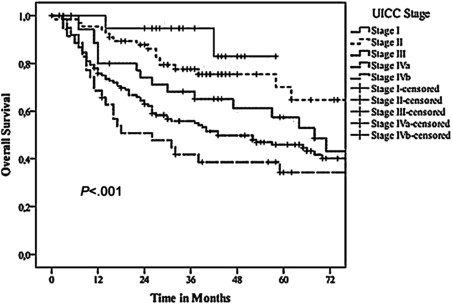
The American Joint Committee on Cancer (AJCC) tumor, node, metastasis (TNM) staging system is a universally accepted, anatomically based clinical staging system for SCCOC ( Table 1 summarizes the most recent seventh edition guidelines published in 2010). Kreppel and colleagues recently evaluated the sixth edition AJCC guidelines published in 2003, confirming that the T stage, N stage, and overall stage groupings remain good predictors of overall survival in patients with SCCOC ( Fig. 2 ). Although the AJCC TNM staging system contains useful prognostic information for SCCOC, it does not include histopathologic features such as tumor thickness, perineural invasion, lymphatic invasion, and extracapsular extension, all of which have been shown to have prognostic significance and influence treatment outcomes for SCCOC.
| Tumor (T) Stage SCCOC | Tumor (T) Stage SCCOP |
|---|---|
| T1: ≤2 cm | T1: ≤2 cm |
| T2: 2–4 cm | T2: 2–4 cm |
| T3: >4 cm | T3: >4 cm, or extension to lingual surface epiglottis |
| T4a: invades maxilla, mandible, extrinsic tongue muscles, maxillary sinus, or skin | T4a: invades larynx, extrinsic tongue muscles, medial pterygoid, hard palate, or mandible |
| T4b: invades masticator space, pterygoid plates, skull base; or encases carotid artery | T4b: invades lateral pterygoid muscle, pterygoid plates, lateral nasopharynx, skull base, or encases carotid artery |
| Lymph Node (N) Stage SCCOC and SCCOP |
|---|
| N0: no regional lymph node metastasis N1: metastasis in a single ipsilateral lymph node, ≤3 cm in greatest dimension N2a: metastasis in single ipsilateral lymph node, >3 cm but ≤6 cm in greatest dimension N2b: metastases in multiple ipsilateral lymph nodes, none >6 cm in greatest dimension N2c: metastases in bilateral or contralateral lymph nodes, none >6 cm in greatest dimension N3: metastasis in a lymph node >6 cm in greatest dimension |
| Overall Stage SCCOC and SCCOP | |||
|---|---|---|---|
| Stage | T | N | M |
| 0 | Tis | N0 | M0 |
| I | T1 | N0 | M0 |
| II | T2 | N0 | M0 |
| III | T3 | N0 | M0 |
| T1 | N1 | M0 | |
| T2 | N1 | M0 | |
| T3 | N1 | M0 | |
| IVA | T4a | N0-N2 | M0 |
| T1-T3 | N2 | M0 | |
| IVB | T4b | Any N | M0 |
| Any T | N3 | M0 | |
| IVC | Any T | Any N | M1 |
Tumor thickness has long been shown to be a strong predictor for occult cervical lymph node involvement for SCCOC, and a recent meta-analysis by Huang and colleagues supported an optimal tumor thickness cutoff point of 4 mm (negative predictive value of 96%) for determining the need for elective treatment of the neck. This 4-mm cutoff value has also previously been suggested by multiple single-institution studies. Perineural invasion has been shown to be a significant independent predictor of local recurrence and overall survival, irrespective of tumor margin status. Studies have also shown perineural invasion to be a significant prognostic indicator of regional metastases. Lymphatic invasion is another poor prognostic marker for SCCOC, conferring a 5 times greater increased risk of recurrence within 3 years in a multivariate analysis by Fan and colleagues. In addition, extracapsular lymph node disease extension has long been shown to be a poor prognostic feature for patients with all head and neck cancers, with an approximately 50% reduction in survival.
Prognostic staging for SCCOP
TNM Staging
The most recent AJCC staging guidelines for SCCOP remain almost identical to those for SCCOC (see Table 1 ). Although there is subtle difference in characterization of advanced primary tumors (T3 and T4) related to invasion of adjacent structures, the early primary tumor (T1 and T2), regional lymph nodes (N), distant metastasis (M), and anatomic stage/prognostic groups for these two distinct diseases are the same. As discussed earlier, the staging system for SCCOC has been validated in the recent literature. In contrast, recent literature has brought into question the staging system for SCCOP, which is still based on experience with SCCOP related to traditional tobacco and alcohol risk factors, and does not account for the improved outcomes of patients with HPV-positive tumors.
HPV Status
Greater than 80% of patients with SCCOP in Western countries may now have HPV-associated tumors. A profile for these patients has become evident over the last decade, with HPV-associated SCCOP tumors often occurring in middle-aged white men with little or no tobacco history. With the increasing incidence of HPV-associated SCCOP over the last several decades, there has been a concomitant trend in these patients presenting with a more advanced stage of disease according to the AJCC staging guidelines, particularly because patients with HPV-associated SCCOP usually present with small primary tumors and are more likely to have multiple early lymph node metastases.
In the Trans Tasman Radiation Oncology Group (TROG) study of 185 patients with SCCOP, patients with p16-positive SCCOP:
- •
Had smaller primary tumors (T1-2 15% for p16 negative vs T1-2 37% for p16 positive; P = .001)
- •
Were more likely to have multiple or large metastatic lymph nodes (N2-3 65% for p16 negative vs N2-3 86% for p16 positive; P = .001)
Additional prospective clinical trials of carcinomas of various head and neck sites by the Eastern Cooperative Oncology Group and the Danish Head and Neck Cancer Group have also shown that patients with HPV-positive or p16-positive carcinoma have more advanced nodal disease at presentation. Notwithstanding that patients with HPV-associated tumors often present with more advanced nodal disease, patients with HPV-associated tumors also have consistently shown improved response to treatment and prognosis compared with patients with HPV-negative tumors.
Smoking Status
In addition to HPV status, smoking status has emerged as a potentially important independent prognostic factor for patients with SCCOP. Smoking status has been shown to be a cofactor in the development of HPV-negative, but not HPV-positive, SCCOP. Many patients with HPV-associated tumors have no tobacco exposure, or significantly less tobacco exposure, than patients with other mucosal upper aerodigestive tract SCCs. However, approximately 50% of patients with HPV-positive tumors may have some smoking history. Several studies have indicated that tobacco exposure is associated with lower survival in patients with HPV-associated SCCOP. Whether this occurs because of a different intrinsic tumor biology of HPV-positive tumors in smokers or is more related to the response of these tumors to therapy remains unanswered.
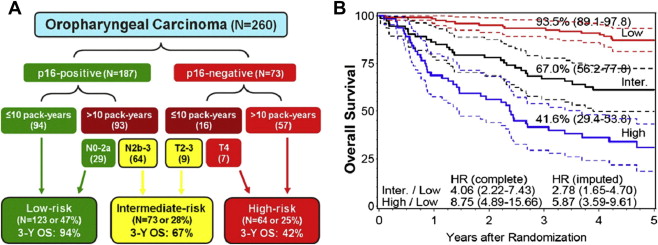
A recent study of patients with SCCOP treated in the RTOG 0129 trial (a randomized trial comparing accelerated-fractionation radiotherapy with standard-fractionation radiotherapy, each combined with cisplatin therapy, in patients with squamous cell carcinoma of the head and neck) specifically evaluated the interaction between tumor HPV status and patient smoking status, finding tumor HPV status and tobacco smoking (≤10 or >10 pack-years) to be the two strongest independent determinants of overall and progression-free survival in patients with SCCOP. Furthermore, patients were stratified into low-risk, intermediate-risk, and high-risk overall survival cohorts primarily based on these two independent risk factors, with 3-year overall survivals of 94%, 67%, and 42% for the low-risk, intermediate-risk, and high-risk groups, respectively ( Fig. 3 ). Nonsmokers with HPV-positive tumors were included in the low risk group, whereas smokers with HPV-negative tumors were included in the high-risk group. The intermediate group included smokers with HPV-positive tumors and higher nodal stage, as well as nonsmokers with HPV-negative tumors and lower tumor (T) stage. Therefore, although tumor HPV status and patient smoking status were the strongest prognostic factors in this risk stratification, traditional TNM anatomic staging factors helped define patients in the intermediate risk cohort.