We read with interest the article by Balachandran and associates in which they report spontaneous recovery of corneal transparency in 2 cases with nearly complete graft detachment after Descemet membrane endothelial keratoplasty. They suggest that “endothelial transfer, migration, regeneration, or a combination thereof from either the donor or the recipient may explain the visual recovery.” We report a case that supports their concept of endothelial migration.
A 45-year-old woman underwent uneventful Descemet stripping endothelial keratoplasty phacoemulsification and intraocular lens implantation for Fuchs endothelial dystrophy. The graft was 8.5 mm in diameter, prepared with manual dissection from an organ-cultured cornea (70-year-old donor; endothelial count, 2600 cells/mm 2 ). The graft was well centered, and postoperative best spectacle-corrected visual acuity (BSCVA) at 1 month was 6/12. Seven months after the procedure, an endothelial rejection episode developed with corneal thickening to 970 μm (host, 600 μm; donor, 370 μm). The rejection responded to intensive topical steroids with a reduction in corneal thickness to 900 μm (host, 610 μm; donor, 290 μm) and recovery of BSCVA to 6/9. Visual acuity was maintained until 20 months after surgery, when the cornea began to decompensate clinically with a reduction in BSCVA from 6/24 to 6/60 at 26 months as a result of corneal edema. An uneventful repeat Descemet stripping automated endothelial keratoplasty was performed. The original graft was peeled off the host cornea and was replaced with an 8.75-mm graft.
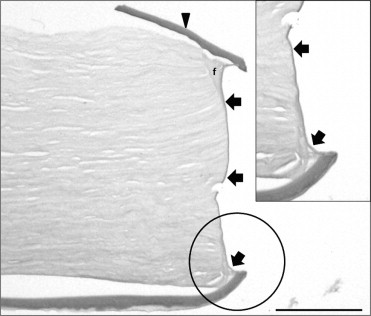
Histologic analysis of the donor lenticula ( Figure ) showed a fragment of Descemet membrane displaced to the anterior (stromal) margin of the graft button, where fibrous tissue joined it to stroma. Although the endothelium was grossly attenuated, a thin new basement membrane (descemetization) extended between the 2 parts of Descemet membrane along the stromal wound surface, indicating endothelial migration along this margin in response to surgery.