Management of malignant neoplasms of the sinonasal tract and skull base is hampered by the relative low incidence and pathologic diversity of patient presentations. Many studies have reported successful outcomes in the endoscopic management of malignancy since 1996, and these are summarized in this article. Nonsurgical adjuvant therapies are important for locoregional control because surgery occurs in a restricted anatomic space with close margins to critical structures, and distant disease is an ongoing concern in these disorders. There remains a need for collaborative consistent multicenter reporting, and international registries have been established to assist in such efforts.
Many of the surgical techniques described endoscopically within the skull base can be applied to malignant sinonasal disease. However, it is the oncological principles of such treatment that must be adhered to when undertaking endoscopic tumor surgery. A focus should be maintained on a surgical philosophy that is driven by the disorder and its staging rather than the available surgical expertise and equipment. The endoscopic tumor surgeon should be equally comfortable in managing the patient by an open craniofacial as well as an endoscopic approach.
| EBM Question | Level of Evidence | Grade of Recommendation |
|---|---|---|
| Are oncological outcomes the same with EES compared to open craniofacial surgery? | 4 | C |
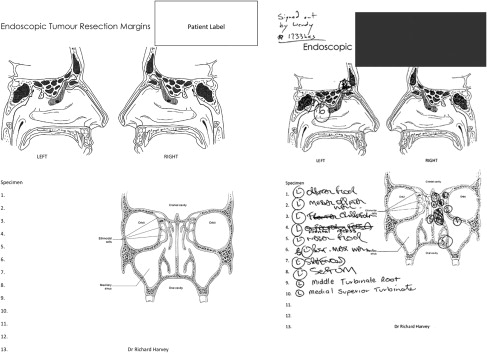
There are 3 foundations for successful endoscopic surgery. First, the resection should be defined with frozen section control of surgical margins. Few endoscopic tumor removals are en bloc and thus margin control is essential. Surgical mapping of such margins are advised ( Fig. 1 ). This mapping also aids postoperative adjuvant therapy planning. The access required should be predetermined by the tumor and preoperative imaging ( Table 1 ). There should be minimal attempts to be conservative at the expense of gaining adequate access for tumor removal. Functional cavity techniques are a secondary concern. In addition, there should be no hesitancy in removing macroscopically involved tissue, such as dura, periorbital, and other important structures. Although the biology of some tumors may afford an approach of gross removal from dura, carotid, and orbital structures with successful adjuvant therapy, this is not standard care and has yet to be proved as effective therapy for malignancy. This shortcoming should not prevent the surgeon from removing obviously involved anatomic barriers at the time surgery ( Fig. 2 ). Much of this is related to surgeon skill and expertise. It differs greatly from managing benign conditions, such as inverted papilloma, in which preserving anatomic barriers to spread is paramount.
| Tasks | CT | Standard MR | Study Planes | Additional MR Sequences |
|---|---|---|---|---|
| To distinguish tumor from retained mucus | Adequate, but less sensitive than MR (3-mm slice thickness better than 1 mm) | TSE T2-weighted sequences are indicated (slice thickness 3 mm) | Axial and coronal planes | FLAIR sequence to differentiate CSF from the cystic/fluid content of tumors or mucoceles |
| To assess periorbita invasion | Bone erosion precisely shown by CT. The periorbita is not usually distinguished from tumor signal (slice thickness 1–2 mm) | SE T1-weighted and TSE T2-weighted sequences are indicated. Periorbita can be more easily separated from tumor signal (slice thickness not >3 mm) | Axial and coronal planes | STIR (orbital fat signal suppressed) may be used to increase detection of orbital fat tissue |
| To assess dura mater invasion | Although skull base erosion is precisely shown by CT, only large dura breakage is detected. Contrast enhancement is required (slice thickness 1–2 mm) | TSE T2-weighted and postcontrast SE T1-weighted sequences are indicated (slice thickness not >3 mm) | Axial, coronal, and sagittal planes | — |
| To assess perineural spread | Limited to indirect signs (fat effacement or enlargement of foramina, muscular atrophy) | Direct demonstration of the abnormal nerve by enhanced fat-saturated SE T1-weighted sequences (slice thickness not >3 mm) | Axial and coronal planes | GE sequences with submillimetric isotropic slices (FIESTA; VIBE) to image the intraforaminal segment of cranial nerves |
| To assess relationships of tumor with cisternal cranial nerve segments | Not indicated | TSE T2-weighted sequence (slice thickness <3 mm) | Axial, coronal, and sagittal planes | MR cisternography with submillimetric isotropic slices (3DFT-CISS; DRIVE) |
| To analyze the intracranial/upper neck internal carotid artery course | CT angiography (requires contrast agent injection, high spatial resolution acquisition). MIP reconstructions | — | Axial, coronal, and sagittal planes | MR angiography (requires contrast agent injection). MIP reconstructions |
Proponents of the traditional craniofacial approach (tCFR) argue that an en bloc resection possible with the tCFR is impossible with endoscopic approaches that, at best, are “piecemeal resection” of the tumor. Proponents of the endoscopic approach are of the opinion that, in resecting tumors involving the anterior skull base an en bloc resection is rarely possible whatever approach is used. Optimum endoscopic visualization enables a wide-field, three-dimensional resection close to an en bloc resection in most cases and a better term is tumor disassembly. Proponents of both approaches agree that the resection is intended to achieve negative margins. An endoscopic approach offers several other advantages. The operation time is shorter, and is associated with less morbidity and shorter hospital stay. Patients do not experience the serious complications that can be associated with the approach in tCFR, nor are they likely to be subject to the reduction in quality of life. Nicolai and colleagues reported a complication rate of 6% following endoscopic resection of malignant tumor compared with 16% after craniofacial resection (CFR). The most common complication after endoscopic approach was cerebrospinal fluid (CSF) leak, followed by mucocele formation. Life-threatening complications, such as intracranial bleeding and infection, are a risk regardless of the approach.
The diversity of the malignant disorders seen in the skull base makes reporting of large homogenous cohorts of patient outcomes scarce. The sinonasal tract and skull base is a region with the greatest histologic diversity in the body, and this is reflected in the extensive disorder classification list compiled by the World Health Organization (WHO) ( Box 1 ).
Nasal cavity and paranasal sinuses
- 1.
Malignant epithelial tumors
- 2.
Neuroendocrine tumors
- 3.
Soft tissue tumors
- 4.
Borderline and low malignant potential tumors of soft tissue
- 5.
Malignant tumors of bone and cartilage
- 6.
Hematolymphoid tumors
- 7.
Neuroectodermal tumors
- 8.
Germ cell tumors
- 9.
Secondary tumors
Incidence and epidemiology
Malignant Tumors
Sinonasal neoplasms are uncommon neoplasms that account only for 1% of all malignancies, 3% of all upper respiratory tract malignancies, and only 3% to 5% of all head and neck malignancies. Annual incidence is 0.5 to 1 new cases per 100,000 inhabitants in Italy, whereas high rates for sinonasal malignancies (SNM) were found in Asian and African populations, the highest age-adjusted rates, between 2.5 and 2.6 per 100,000 per annum, occurring in Japanese men. Sinonasal malignancies are more common in men. The male/female ratio is reported to be between 1.2 and 2.7/1. In the maxillary sinus, the male/female ratio is 2:1, and in the ethmoid sinus the male/female ratio is 1.4:1. Overall, 75% of all malignant tumors occur in persons older than 50 years.
The most common sinonasal malignancies are the primary epithelial tumors, followed by the nonepithelial malignant tumors. In the group of epithelial SNMs, the squamous cell carcinoma (SCC) dominated, and, in the nonepithelial SNMs, the most common group was malignant lymphoma. The prevalence of the different malignant tumors in the literature is extremely variable. The incidence of epithelial SNMs ranges between 52.9% and 91%. In a series of 115 patients, Svane-Knudsen reported that 64% had well-differentiated SCCs, adenocarcinomas, and adenoid cystic carcinomas. Non-Hodgkin lymphomas and undifferentiated carcinomas represented 9% and 2.6%, respectively. In a German series of 216 cases, Zbaren and colleagues found 56% to be epidermoid carcinomas and 14% to be adenocarcinomas. Similarly, in 60 Japanese patients, Haraguchi and colleagues found a predominance of well-differentiated SCCs (25%) followed by melanomas and NHL (23%) and a small number of undifferentiated carcinomas (5%). However, in areas where there is a high incidence of sinonasal neoplasms, the histopathologic spectrum is different from the spectrum in low-risk areas. Undifferentiated carcinomas in Chinese high-risk areas (eg, Hong Kong) constitute more than 80% of all sinonasal malignancies. Incidence, site, and histologic type can vary in different geographic areas, which may be because of occupational, social, and genetic factors. For all nose and sinus tumors, the nose is the primary site in 25% and the sinuses 75%, and of all sinus neoplasms, 60% to 80% originate from maxillary sinus. However, it is not easy to determine the exact site of origin with large tumors. As a result, the tumor distributions in the literature are variable.
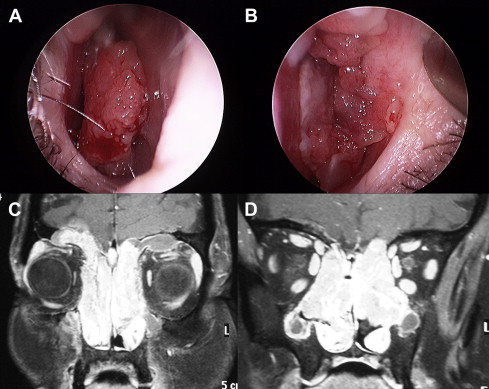
SCC is the most common tumor of the sinonasal malignancies ( Fig. 3 ). Approximately 60% to 73% of SCCs originate in the maxillary sinus, 20% to 30% in the nasal cavity, 10% to 15% in the ethmoid sinus, and 1% in the sphenoid and frontal sinuses. Among the carcinomas of the nose and paranasal sinuses, sinonasal gland carcinomas represent the second most frequent type of malignant epithelial tumor, and the paranasal sinuses are the most common site of minor salivary gland involvement. Adenoid cystic carcinoma (ACC) accounts for less than 1% of all head and neck malignancies and 10% of all salivary gland neoplasms. Lupinetti and colleagues reported that most patients were white (72.4%), nonsmokers (48.4), and nondrinkers (74.4%) in their ACC series. Sinonasal ACC accounts for 10% to 25% of all head and neck ACC. The maxillary sinus (47%) and the nasal cavity (30%) were the most common primary tumor sites. ACC has a propensity for perineural spread and bony invasion, which can lead to significant skull base involvement and intracranial extension.
Adenocarcinoma is the third most common mucosal epithelial malignancy found in this area ( Fig. 4 ), after SCC and ACC, and represents approximately 8% to 15% of all sinonasal cancers. The incidence is less than 1 case per 100,000 inhabitants per year, occurring predominately among men with a mean age of presentation of 60 to 65 years. However, in the northern part of Spain, the incidence is 0.19 cases/100,000 inhabitants per year. The median age of onset lies between 50 and 60 years and even earlier in wood dust–related tumors. Men develop adenocarcinoma 4 times more frequently than women, implying an occupational hazard. It is located most frequently (85%) in the ethmoid sinus and the upper part of the nasal cavity. One study using endoscopic endonasal surgery showed that woodworkers’ adenocarcinomas constantly originated in the olfactory cleft, appearing as polyplike neoplasms with well-defined boundaries. They occasionally arise in other sites of the nasal cavity (maxillary sinus in 10%) and these cases are usually not related to wood dust exposure.
Sinonasal mucoepidermoid carcinoma accounts for 0.6% of all salivary tumors and 4.8% of all mucoepidermoid carcinomas. The most common site is maxillary sinus, followed by nasal cavity, nasopharynx, and ethmoid sinuses in order of decreasing frequency.
Associated Risk Factors
Wood dust exposure
The association between wood dust exposure and adenocarcinoma of the sinuses is also well established. It is estimated that woodworkers have a 500 times increased risk compared with the male population and up to 900 times compared with the population in general. It has been shown that the true risk factor is the exposure to wood dust particles, and not the possible exposure to chemical products used in the industry, such as polish, varnish, or protectors. Hardwood types, such as ebony, oak, and beech, confer the highest risk of developing sinonasal adenocarcinomas, increased further by inhalation of formaldehyde or substances normally used in this type of industry. The strong relation of adenocarcinoma to exposure to wood dust makes it a disease almost exclusive to carpenters and furniture makers. Therefore, in many countries (eg, Australia, Germany, the United Kingdom, Belgium, France), it is considered an industrial disease. The furniture makers who are likely to be exposed to the fine wood dusts of threshold greater than 5 mg/m 3 /d are at greater risk. Many findings indicate a dose-response relationship, with a higher incidence of tumors occurring among workers exposed for longer periods of time. Recent studies have shown that even short periods of exposure (<5 years) can lead to an increased risk of carcinoma. In general, the normally long latency period is estimated at 40 years, although it can range between 20 and 70 years. Despite this clear cause, it is still unknown by what molecular mechanism sinonasal adenocarcinomas develop. Because wood dust does not have mutagenic properties, it is hypothesized that prolonged exposure to, and irritation by, wood dust particles stimulate cellular turnover by inflammatory pathways.
Smoking
Smoking is associated with an increased risk of nasal cancer, especially SCC of the maxillary sinus. However, some reports did not find any increased risk for sinonasal tract malignancies associated with tobacco and alcohol. Further research is needed to determine whether smoking is a significant causal factor in sinonasal carcinoma.
Chemical exposure
Thorium dioxide, when used as an imaging agent, may cause antral squamous and mucoepidermoid carcinomas. Although no other definitive risk factors for mucoepidermoid carcinoma have been identified, minor trauma and chronic irritation have been implicated in the cause of sinonasal tract cancers in general. Relative risk rates for sinonasal epithelial malignancies have been determined for several chemical agents (chromates, nickel compounds, isopropylic alcohol, and mustard gas) and for several occupations (ie, nuclear refinery work, leather work in boot and shoe manufacturing, chrome pigment work, metalwork, textile work, construction work, baking, flour milling, and farming) even in the apparent absence of causal agents. Increased risks to different industries were reported as: the metal industry, relative risk ranging from 3.1 to 5.9; the textile industry, ranging from 2.9 to 17.0; the mining and construction industry, ranging from 2.3 to 5.3; and the agricultural industry, ranging from 1.9 to 3.3. Among women, exposure to textile dust was associated with an increased risk of SCC and adenocarcinoma. For SCC, the risk increased with the duration and the level of exposure. The risks associated with the different types of textile fibers (cotton, wool, and synthetic fibers) were similar and the results did not incriminate a particular type of textile. An association between SCC and nickel exposure has been shown by Pedersen and colleagues who reported that workers at a nickel refinery in Norway developed SCC at 250 times the expected rate, with a latent period varying from 18 to 36 years.
Human papillomavirus infection
The current evidence linking human papillomavirus (HPV) to at least a proportion of benign sinonasal papillomas is convincing. Based on the analysis of more than 1000 such lesions, Syrjaenen reported that HPV-6 and HPV-11 is present in one-third (33.3%) of inverted papillomas and this detection rate is higher than most other reported extragenital papillomas, except those of the larynx and bronchus. Tang and colleagues detected human papilloma virus in up to 86% of inverted papilloma cases. The 2005 International Agency for Research on Cancer evaluation on the carcinogenicity of HPV in humans concluded that there is sufficient evidence for the carcinogenicity of HPV in the oral cavity and oropharynx, limited evidence in the larynx, and inadequate evidence in sinonasal cavities. However, some previous reports have suggested a possible implication of HPV in the development of several carcinomas of the sinonasal region. In 1993, Kashima and colleagues found that 4% of SCC were HPV positive. Alos and colleagues detected HPV DNA in tumor tissue of 20% of patients with sinonasal SCC. The tumors affected predominantly men, by a ratio of approximately 3:1; no significant differences in sex and age were found between HPV-positive and HPV-negative groups. There were no significant differences in tumor stage at presentation. Despite the similar clinical characteristics and staging at presentation, patients with HPV-positive tumors had a significantly better prognosis than those with HPV-negative neoplasms ( Fig. 5 ). Syrjaenen showed that 21.7% of sinonasal carcinomas analyzed were positive for HPV. Low-risk HPV types 6 and 11 are usually confined to benign lesions, whereas the reverse is true for the oncogenic HPV types 16 and 18, and the presence of squamocolumnar junctions and squamous cell metaplasia in the sinonasal system. The discrepancies reported by several studies might result, in part, from technical reasons, but it is also possible that sinonasal lesions have a heterogeneous cause (HPV related and nonrelated) and/or that some novel (as yet unidentified) HPV types exist in these lesions, which are detected by some studies but not by others.
Rare Tumors
Primary sinonasal tract mucosal malignant melanomas are rare, accounting for between 0.3% and 2% of all malignant melanomas and about 4% of head and neck melanomas. The head and neck represents the most common site of mucosal malignant melanoma with a suggested incidence of about 0.018/10 5 to 0.051/10 5 per year. Sinonasal tract mucosal malignant melanomas represent up to 4% of all sinonasal tract neoplasms. In the National Cancer Database report by the American College of Surgeons Commission on Cancer and the American Cancer Society of more than 84,000 melanomas seen from 1985 to 1994, only 1.3% were melanomas that arose from mucosal surfaces, of which 55% were of the head and neck. Sinonasal tract mucosal malignant melanomas were found to be equally common in men and women. A higher proportion of melanoma was identified in black patients (10.4%). In general, the mean age for sinonasal tract mucosal malignant melanomas (64.3 years) is later than for cutaneous malignant melanomas. Sinonasal tract mucosal malignant melanoma is a more lethal disease in patients older than 60 years, a finding similar to cutaneous melanoma. Tumors originating in the sinuses are less common than those arising in the nasal cavity, but sinus tumors may grow asymptomatically until late in the disease course. One-third of patients had neck metastases, which often preceded distant metastasis, and distant metastasis was always rapidly fatal.
The incidence of olfactory neuroblastoma was 0.4 cases/million inhabitants per year but is difficult to establish, and the tumor is not as rare as is commonly reported and probably represents more than 5% of all nasal malignant tumors. Olfactory neuroblastoma occurs in a wide age range (3–90 years), with a bimodal peak in the second and sixth decades of life. Occasional cases have also been reported in children younger than 10 years. Olfactory neuroblastoma affects male and female patients with similar frequency and can be found in all age groups. No known causal factor exists for this tumor, although diethylnitrosamine injections can induce tumors in hamsters at the site of the olfactory epithelium. No hereditary patterns have been described for this neoplasm, and there is no apparent racial predilection.
Extrapulmonary neuroendocrine carcinomas (SNEC) only account for 4% of all SNECs, and few cases of SNECs of head and neck have been reported. Less than 250 cases of head and neck SNEC have been published, including 48 cases of SNEC in the nasal and paranasal cavities. Most patients with SNEC of the head and neck are male. Although there seems to be an association with cigarette smoking, the association is not as strong as that with pulmonary SNEC. Although the neoplasm has been described at any age between 16 and 77 years, the prevalent distribution is in the fifth and sixth decades. No particular risk factors for this tumor have been identified.
Although tumors of this type occur in a variety of organs and sites, small cell undifferentiated carcinoma (ScCC) of the sinonasal tract is a rare malignancy, with the reported series all having fewer than 10 patients. In the MD Anderson series of neuroendocrine tumors, there were only 7 cases of small cell carcinoma. The paucity of well-documented cases precludes generalization about the clinical features. Within this limitation, the mean age at presentation is approximately 50 years (range 26–77 years), and there is no sex predilection. Anatomic sites include the nasal cavity, ethmoid sinuses, and maxillary sinus.
Sinonasal undifferentiated carcinoma (SNUC) is also a rare tumor, with fewer than 100 reported cases in the world literature. There is a male predominance (2–3:1). The age range is broad, usually ranging from the third to ninth decades; the median age at presentation is in the sixth decade. There are no known causal agents. SNUCs are typically negative for Epstein-Barr virus (EBV). Some cases have been reported to develop following radiation therapy for nasopharyngeal carcinoma.
The annual incidence of the Ewing’s Sarcoma Family of Tumors (ESFT) in the United States is 2.1 cases per million children, and they account for approximately 2% of all cancers in children and young adults. ESFT is more common in male than in female patients and has a greater incidence in white and Hispanic children than in black or Asian children. ESFT is not believed to be inherited and is not associated with any cancer syndromes. In 95% of cases, at (11;22)(q24;q12) translocation is detected. Sinonasal tract involvement is rare, with about 50 cases reported in the English literature. Most of them were observed in the maxillary sinus, whereas fewer than 10 cases each involved the ethmoid and nasal fossa (also known as PNET-primitive neuroectodermal tumor).
Hemangiopericytomas are unusual vascular tumors that account for only 1% of all vascular neoplasms and for 3% to 5% of sarcomas. They rarely occur in the paranasal sinuses and nasal cavity. The rate of head and neck involvement ranges between 15% and 25%, with sinonasal tract localization present in 5% of patients. Ethmoid, nasal cavity, and sphenoid sinus are the preferential sites of origin. Although the tumor affects all ages, it occurs most commonly in adults in the sixth and seventh decades of life. No gender predominance is reported. Trauma, steroid therapy, and altered hormone secretions are proposed as predisposing factors.
Sarcomas of the head and neck are rare tumors, accounting for 4% to 10% of all sarcomas and fewer than 1% of all malignancies of the head and neck region. Sarcomas of the sinonasal tract comprise about 15% of sinonasal tumors. Oral and maxillofacial sarcomas present at any age from 5 months to 77 years (mean 42 years) and there is a male/female ratio of 3:1 with predilection for the mandible. The mean age and male/female ratio in Africa is lower than in Western series.
Osteosarcoma is a rare bone tumor that occurs primarily in long bones. Overall incidence is 1:100,000 inhabitants per year. Between 6% and 13% of cases occur in the head and neck region. Osteosarcoma had peak prevalence in the third decade, with equal gender distribution. Occurrence in the pediatric age is rare. In the maxillofacial region, it tends to occur a decade later than in long bones. Osteosarcoma accounts for 0.5% to 1% of all sinonasal tract tumors. In children with osteosarcoma, about 3% carry a germ line mutation in p53, with most of these having a family history suggesting Li-Fraumeni syndrome. The incidence of osteosarcoma has been increasing by about 1.4% per year for the past 25 years. The cause of osteosarcoma remains unknown. Bone abnormalities and diseases such as Paget disease of bone, fibrous dysplasia, myositis ossificans, other hereditary disorders like retinoblastoma, Li-Fraumeni syndrome, and previous chemotherapy and irradiation for other malignancies have been suggested as specific risk factors.
Rhabdomyosarcoma is the most frequent soft tissue sarcoma in the pediatric age group, accounting for up to 75% of all child sarcomas and 6% of all pediatric cancers. The embryonal subtype is the most common. Mesenchymal rhabdomyosarcoma is rare. The head and neck region is the most commonly involved site (37%). Occurrence of head and neck rhabdomyosarcoma in adults is rare. Only 10% of all soft tissue tumors and 1% of all neoplasms in the sinonasal tract are rhabdomyosarcomas. Sinonasal tract localization is present in about 8% of all adult-age rhabdomyosarcomas.
Chondrosarcoma make up only 10% to 20% of malignant primary bone tumors, with 5% to 10% located in the head and neck. Maxillary sinus is the most frequently involved site. In the skull base, chondrosarcomas typically occur at the petroclival synchondrosis. The lesion is commonly diagnosed in the sixth decade. The pediatric population is rarely affected. There is no gender predominance. However, in some reports it is more frequently seen in men. The cause of chondrosarcoma remains unknown. Meanwhile, associated conditions include multiple hereditary exostosis, Ollier disease, Maffucci syndrome, previous intravenous thorium dioxide contrast use, Paget disease of bone, chondromyxoid fibroma, and previous irradiation.
Leiomyosarcoma is unusual in the orofacial region and accounts for approximately 7% of all soft tissue sarcomas. It is the fourth most common sarcoma, mainly in the maxilla, and with a 5:1 male/female ratio. Sinonasal tract localization is rare, with about 40 cases reported in the literature.
Fibrosarcoma with mandibular predominance and equal sex distribution was the fifth most common sarcoma. Liposarcoma, fibromyxosarcoma, neurofibrosarcoma, ameloblastic sarcoma, and synovial sarcoma are rare.
Sinonasal lymphomas, either primary or secondary, are mostly non-Hodgkin lymphomas (NHLs) and are the second most common malignant tumors following carcinomas occurring in the sinonasal tract. NHLs are classified into B and T-NK subtypes according to lymphocytic phenotype. There is a difference in incidence, epidemiology, and cell type between Western and Asian countries. In Western countries, lymphomas are infrequent and sinonasal tract involvement varies between 0.2% and 2% of all NHLs. They constitute 5.8% to 8% of the extranodal lymphomas arising in the head and neck area. B-cell lymphomas are predominant and tend to affect paranasal sinuses in the elderly. In Asian and South American countries, the incidence of NHLs of the nasal region is higher than in the United States, they account for 2.6% to 6.7% of all lymphomas, and are the second most frequent group of extranodal lymphomas after gastrointestinal lymphomas. T or NK cell lymphomas are predominant and the nasal cavity is mainly involved in younger people.
EBV is considered important in the etiopathogenesis of lymphomas, especially for specific lymphomas such as Burkitt lymphoma and nasal NK-T lymphoma. In Asian countries, the prevalence of EBV-positive T-cell lymphomas is similar to the prevalence of EBV virus infection and differs from the findings of the more common EBV-negative B-cell nasal lymphomas in the United States. These findings suggest that EBV plays a role in the development of nasal T-cell lymphomas and that the incidence of EBV infection may explain the reported East-West difference in the incidence of nasal T-cell lymphomas.
Most of the malignant tumors of the sinonasal regions are primary in origin. Metastasis of malignant tumors to the sinonasal area occurs infrequently and usually presents at the late stage of primary disease. More than 50% of sinonasal metastases originate from a renal carcinoma. Other most common primary sources, in decreasing order after the kidney, are lung (12%), urogenital ridge (12%), breast (9%), and gastrointestinal tract (GI) tract (6%). The most common metastatic sites are the maxillary sinus (50%), followed by the ethmoid sinus (18%) and nasal cavity (15%). However, some reports from east Asia are different from European and North American reports. Different incidences of malignant neoplasms in the primary site may explain the different incidences of sinonasal metastatic tumor. Although the mean age of patients with sinonasal metastases varies in different primary origins, the highest incidence is in the sixth decade in men and the seventh decade in women.
SCC
Results following endoscopic resection of sinonasal SCC
Although large series of SCC of the maxillary sinus were found in the literature review, obtaining accurate survival figures was not straightforward. Comparison across studies was often confounded by heterogeneous patient cohorts and treatment modality. Most cases received radiotherapy combined with some form of maxillectomy with or without orbital clearance. In addition, most tumors were T3 or T4 at presentation and had frequently extended posteriorly into the pterygoid region, which significantly reduces long-term survival. The overall 5-year survival of maxillary SCC was reported at 25%, although patients with T1 tumors at presentation were higher at 55%.
Few studies reported oncological outcomes of SCC exclusively following endoscopic excision. Some studies reported on endoscopy-assisted surgery combined with conventional open approaches, whereas others compared outcomes between surgery and radiotherapy. Most published data are derived from a heterogeneous patient cohort of varied histologic type, in which the main objective was to compare outcomes between endoscopic and CFR. In studies that did reported outcomes following endoscopic resection of malignant tumors, there were frequently insufficient SCC cases for exclusive analysis.
One published study was identified from the literature review to have reported outcomes for endoscopic resection of sinonasal SCC. This was a small cohort study of 11 patients with a mean age of 62.5 years. Radiation or chemotherapy was used in 8 patients. Seven patients underwent surgery using a strictly endoscopic approach, whereas 4 required combined endoscopic and neurosurgical resection. Local recurrence and distant metastatic rates were 20% and 0%, respectively. Overall survival and disease-free survival were both calculated at 91%, with mean follow-up of 31.5 (range 6–88) months.
Eighteen studies were identified to be potentially relevant and had evaluated oncological results following endoscopic resection, performed as the sole procedure or in combination with CFR. Data related to SCC were scarce. Twelve articles included some reports on SCC ( Table 2 ).
| First Author, Year | Total Number of Malignant Sinonasal Tumors | Total Number of SCC in the Series | |
|---|---|---|---|
| 1 | Eviatar et al, 2004 | 6 | 1 |
| 2 | Castelnuovo et al, 2006 | 13 | 3 |
| 3 | Poetker et al, 2005 | 16 | 5 |
| 4 | Shipchandler et al, 2005 | 11 | 11 |
| 5 | Buchmann et al, 2006 | 78 | 33 |
| 6 | McKay et al, 2007 | 73 | 30 |
| 7 | Kim et al, 2008 | 40 | 7 |
| 8 | Chen, 2006 | 7 | 1 |
| 9 | Lund et al, 2007 | 49 | 3 |
| 10 | Podboj and Smid, 2007 | 16 | 6 |
| 11 | Nicolai et al, 2008 | 184 | 25 |
| 12 | Eloy et al, 2009 | 66 | 25 |
| Total | 559 | 150 |
A total of 150 patients with SCC were pooled from the data available (see Table 2 ). If a single center had generated more than 1 case series, from overlapping periods, data from the most recent series were used. Sixty-four patients underwent the traditional CFR (tCFR), 40 patients underwent endoscopy-assisted surgery with an appropriate open approach, and 39 were managed purely with endoscopic surgery ( Table 3 ). Seven patients were deemed unresectable or declined surgery and were treated with radiotherapy and chemotherapy. Only 1 study reported exclusively on endoscopic surgery for SCC.
| First Author, Year | SCC | tCFR | Combined | Endoscopic | Remarks |
|---|---|---|---|---|---|
| Eviatar et al, 2004 | 1 | — | — | 1 | — |
| Castelnuovo et al, 2006 | 3 | — | 3 | — | Endoscopic nasal and anterior craniotomy |
| Poetker et al, 2005 | 5 | — | — | 5 | — |
| Shipchandler et al, 2005 | 11 | — | 4 | 7 | — |
| Buchmann et al, 2006 | 33 | — | 33 | — | Open approaches complemented with endoscopic |
| McKay et al, 2007 | 30 | 23 | — | — | 7 underwent radiotherapy with chemotherapy |
| Kim et al, 2008 | 7 | 7 | — | — | — |
| Chen, 2006 | 1 | — | — | 1 | — |
| Lund et al, 2007 | 3 | — | — | 3 | — |
| Podboj and Smid, 2007 | 6 | — | — | 6 | — |
| Nicolai et al, 2008 | 25 | 9 | — | 16 | — |
| Eloy et al, 2009 | 25 | 25 | — | — | — |
| Total | 150 | 64 | 40 | 39 | 7 treated with radiotherapy/chemotherapy |
Of the 39 patients who underwent purely endoscopic surgery, data were available only for 23 patients. Individual data were collated from 5 studies, and are summarized in Table 4 . Patient demographics, tumor staging, site of origin, extent of tumor invasion, recurrence, and site of distant metastasis were not consistently reported in all of the 5 studies. Twenty-three patients, with a mean age of 59.8 (range 25–85) years, were analyzed. The male/female ratio was 2:1 (12 male, 6 female, 5 unreported). Contrary to previous studies that reported a preponderance of advanced disease, 65.2% of patients had either T1 or T2 tumors at presentation. This finding may represent selection bias of the investigators to offer endoscopic resection of the tumor. Six patients (26.8%) had local recurrence of SCC, which was higher than the 12% reported by Nicolai and colleagues. One of the 6 patients who had local recurrence also had distant metastasis (patient #5; see Table 4 ). Another patient (patient #16; see Table 4 ), who did not have local recurrence, was found to have distant metastasis to the brain. At latest follow-up, 19 patients (82.6%) were alive with no evidence of disease. Three patients (2 T1 and 1 T2) died of their disease, including the patient who had distant metastasis to the brain. One patient died of other causes.
| Patient No. | Gender | Age | Extent | Staging | Recurrence | Metastasis | Follow-Up (Mo) | Status |
|---|---|---|---|---|---|---|---|---|
| 1 | M | 63 | E | T1 | N | N | 25 | DFS |
| 2 | F | 68 | E, CP, LNW, orbital wall | T3 | N | N | 54 | DFS |
| 3 | F | 66 | Septum, M, nasal cavity | T2 | N | N | 31 | DFS |
| 4 | M | 66 | E, M, Mt | T3 | N | N | 30 | DFS |
| 5 | M | 54 | Septum, LNW | T2 | Y | N | 15 | DFS |
| 6 | M | 85 | E, M, S, CP, PMF, LNW | T4a | Y | N | 6 | DFS |
| 7 | M | 54 | Ant and LNW | T1 | N | N | 9 | DFS |
| 8 | Unknown | 70 | M, E | T1N0 | N | N | 89 | DFS |
| 9 | Unknown | 40 | St | T1N2b | Y | Y | 10 | DOD |
| 10 | Unknown | 61 | Mt | T1N0 | N | N | 21 | DFS |
| 11 | Unknown | 63 | E, M | T2N0 | Y | N | 92 | DFS |
| 12 | Unknown | 65 | Septum | T2N0 | Y | Y | 7 | DOD |
| 13 | M | 49 | Not stated | Stage IVB | Y | N | 57 | DFS |
| 14 | M | 69 | E, NF | T2 | N | N | 63 | DFS |
| 15 | F | 47 | NF | T1 | N | N | 62 | DFS |
| 16 | F | 80 | NF | T1 | N | Y | 28 | DOD |
| 17 | M | 50 | E | T3 | N | N | 34 | DFS |
| 18 | M | 35 | E | T2 | N | N | 89 | DFS |
| 19 | M | 40 | E | T4 | N | N | 78 | DFS |
| 20 | F | 71 | IT, NF, septum, and torus | T4b | N | N | 77 | DFS |
| 21 | M | 25 | E, PE, St, Mt, ant wall SS | T4 | N | N | 58 | DFS |
| 22 | F | 77 | E and MT | T2 | N | N | 19 | DOC |
| 23 | M | 77 | NC | T1 | N | N | 3 | DFS |
| Summary | 12 men 6 women 5 unknown | 59.78 (mean) 25–85 (range) | — | T1 = 8 T2 = 7 T3 = 3 T4 = 4 | Yes = 6 No = 17 | Yes = 3 No = 20 | 41.6 (mean) 3–92 (range) | DFS = 21 DOD = 3 DOC = 1 AWD = 1 |
Other reports of patients who were treated endoscopically lacked data documentation. These include 3 patients with SCC in a cohort of 49 patients reported by Lund and colleagues. One of these patients died at 40-months follow-up, 1 was alive with disease, and the third was disease free. The follow-up of this cohort ranged from 6 to 126 months (mean 36 months). They report overall survival of 88% at 5 years for the entire cohort. There were insufficient data to calculate survival outcome for the patients with SCC. Eviatar and colleagues report 1 case of a 76-year-old patient treated with endoscopic approach in a cohort of 6 patients with malignant sinonasal tumors that were treated in a 7-year period. This patient remains disease free 4 years after the surgery. More recently, Nicolai and colleagues reported their experience of 134 patients with malignant sinonasal tumors managed exclusively with endoscopic approach. This group included 16 patients with SCC. They report a 5-year disease-specific survival of 91.4% (standard deviation [SD] 3.9%) for the entire cohort of 134 patients treated with the endoscopic approach.
Two studies compared endoscopic outcomes with a tCFR cohort, whereas another 2 compared endoscopic and combined approaches. All studies were retrospective reviews of outcomes, with study cohorts ranging from 2 to 133 patients. When the studies were assessed against the Oxford Center for Evidence-Based Medicine Levels of Evidence criteria, all studies were judged to have level 4 evidence.
Conclusion
- •
Data on endoscopic surgery for sinonasal SCC are limited, although the accrued data from the pooled patients seems promising. Comparison between the pooled data and previously published outcomes is compounded by the heterogeneous patient population and small cohort of each tumor stage. Nonetheless, the overall disease-free survival rate seems to be comparable with conventional approaches. However, the mean follow-up period is limited to less than 4 years. The overall survival following CFR of sinonasal SCC was 67% at 3 years and decreased to 64% at 5 years’ follow-up.
- •
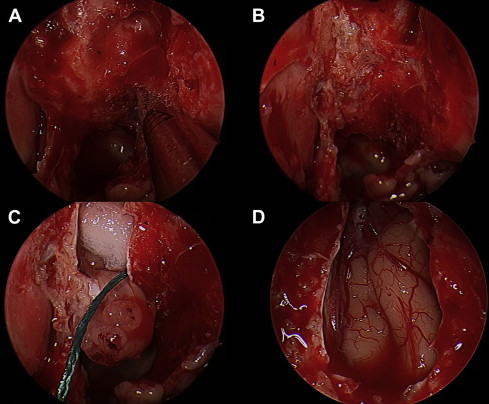
Whichever surgical technique is used, there is good evidence that the outcome is related to how thoroughly the tumor has been removed. A wide-field three-dimensional resection undertaken with optimum endoscopic visualization, achieving negative margins, offers resection of the tumor that is close to an en bloc resection, which is rarely possible in practice ( Fig. 6 ). The overall morbidity and mortality associated with endoscopic resection of sinonasal SCC seems to be less than with traditional approaches.

Fig. 6
( A ) SCC extended to nasal dorsum (CT) and requires resection to clear the margins ( B ) the remaining part was performed endoscopically. Local glabella flap was used for reconstruction ( C ). The goal of surgery is near-field 3 dimensional resection controlled by histological assessment – not an open or endoscopic debate.
Adenocarcinoma
Adenocarcinoma is a glandular malignancy of the sinonasal tract. It is divided into 2 main groups: (1) intestinal-type adenocarcinoma (ITAC), and (2) nonintestinal-type adenocarcinoma. Nonintestinal-type adenocarcinoma is further divided into low-grade and high-grade subtypes.
ITAC
This carcinoma resembles adenocarcinoma of the intestinal tract.
Epidemiology and causes
This tumor has a male predominance, probably caused by occupational exposure, and usually presents in the fifth and sixth decades (mean age at presentation 58 years). Wood dust and leather dust have been shown to be associated with the development of this tumor in several different countries, with a considerable delay between exposure and presentation (up to 40 years). It is believed that the larger dust particles may be involved because they are preferentially accumulated in the nose. The carcinogens involved are still unknown but may include alkaloids, saponins, stilbenes, aldehydes, quinones, flavonoids, terpenes, fungal proteins, and tannins.
Histology
There are 2 published classifications of these tumors, those of Barnes and Kleinsasser and Schroeder. The Barnes classification is preferred because it is simpler, and is the classification presented in Table 5 . The Kleinsasser and Shroeder classification divides the mucinous type of tumor into alveolar and signet ring tumors. Franchi and colleagues showed that such a division had no prognostic significance.
| Types | Approximate Prevalence Varies from Author to Author (%) | Differentiation | 3-y Cumulative Survival (%) a |
|---|---|---|---|
| Papillary | 18 | Well differentiated | 82 |
| Colonic | 40 | Moderately differentiated | 54 |
| Solid | 20 | Poorly differentiated | 36 |
| Mucinous | 14 | Mucinous | 48 |
| Mixed | 8 | Mixed differentiation | 71 |
ITAC are generally locally aggressive with a local recurrence rate of around 50%, local lymph node spread of about 10%, and distant metastasis rate of 20%. The cumulative, disease-specific, 5-year survival rate is between 40% and 60%, with most deaths occurring in the first 3 years. Because the average presentation of these tumors is generally late, with most being T3 and T4 tumors, staging tumors according to the tumor-node-metastasis (TNM) staging system has little prognostic significance.
Sinonasal nonintestinal-type adenocarcinomas
The tumors are divided into low-grade and high-grade subtypes, with low-grade presenting mostly in the ethmoid cells and the high-grade in the maxillary sinus. These tumors may present in the nasal cavity or in any combination of the locations discussed earlier. Low-grade tumors have a more indolent course, presenting with unilateral nasal obstruction and epistaxis, whereas high-grade tumors may present with additional symptoms associated with extension of the tumor into the orbit (double vision, proptosis), infratemporal fossa (infraorbital nerve sensory changes), or intracranial cavity (frontal lobe symptoms and headache).
Low-grade tumors have an excellent prognosis, with 5-year survival of up to 85%, whereas high-grade tumors have a poor prognosis, with 3-year survival of around 20%.
Salivary Gland–type Carcinomas
Salivary gland–type adenocarcinomas are uncommon, occurring in 5% to 10% of sinonasal adenocarcinomas. They are believed to originate from the seromucinous glands of the nasal and sinus epithelium. Table 6 lists the types and occurrence of all sinonasal salivary tumors (both malignant and benign).
| Tumor Type | Percentage Occurrence |
|---|---|
| High-grade adenocarcinoma not otherwise specified | 30 |
| ACC | 17 |
| Mucoepidermoid carcinoma | 5 |
| Low-grade salivary-type adenocarcinoma (various types including mucoepidermoid and acinic cell carcinoma | 21 |
| Pleomorphic adenoma a | 23 |
Adenocarcinoma not otherwise specified may be considered a diagnostic entity on its own and is often poorly differentiated with a poor prognosis, in keeping with other poorly differentiated adenocarcinomas. ACC is the most common salivary gland malignant tumor, originating most commonly in the maxillary sinus (60%) and nasal cavity (25%). The extent of tumor spread is often underestimated by radiology as perineural spread, which is common in this tumor and often remains undetected, and the long-term survival is poor with 7% 10-year survival with most patients dying of local recurrence rather than distant metastasis. Long-term follow-up is thus mandatory to detect late recurrences. The other salivary gland malignancies are all very rare and not individually presented.
Treatment
Most studies on the treatment of sinonasal malignancies do not separate the histologic types of tumors and present series in which the treatment of these tumors are grouped together ( Table 7 ). There are only a few published studies in which the adenocarcinomas have been separately reported. A great deal of the evidence for the treatment of nonepidermoid malignancies comes from separating these tumors from other tumors in the published studies.
| First Author, Year | Total Number of Malignant Sinonasal Tumors | Total Number of Adenocarcinomas |
|---|---|---|
| Lund et al, 1998 | 167 | 42 |
| Stammberger et al, 1999 | 43 | 7 |
| Thaler et al, 1999 | 4 | 1 |
| Goffart et al, 2000 | 78 | 40 |
| Roh et al, 2004 | 47 | 2 |
| Poetker et al, 2005 | 16 | 2 |
| Ganly et al, 2005 | 334 | 107 |
| Batra et al, 2005 | 25 | 3 |
| Buchmann et al, 2006 | 78 | 2 |
| Castelnuovo et al, 2006 | 18 | 10 |
| Chen, 2006 | 7 | 4 |
| Howard et al, 2006 | 259 | 62 |
| Lund et al, 2007 | 49 | 15 |
| Podboj and Smid, 2007 | 16 | 5 |
| Total | 1141 | 302 |
The central issue in the treatment of adenocarcinomas is to prevent locoregional recurrence, because most patients die as consequence of a local recurrence rather than as a result of either local or systemic metastasis. Treatment is focused on removing the tumor, where possible with a clear margin, and this depends on the site of the tumor. Pedunculated or isolated tumors attaching to turbinates or the septum can be easily removed with a good margin of normal tissue either by endoscopic or open approach. The treatment controversy is around tumors that abut or transgress the skull base or orbit. The current gold standard for the treatment of these tumors remains a CFR (tCFR), which involves a craniotomy to expose the anterior skull base from above and, traditionally, an open approach to the nasal and sinus cavity allowing resection of the cribiform plate, ethmoids, fovea ethmodalis, anterior face of sphenoid, and septum. Orbital involvement is determined by whether or not the orbital periostium is breached. If not breached, this structure is preserved. Postoperative irradiation is advocated by most investigators, although the evidence for its usefulness is lacking. Adjuvant chemotherapy is rarely given. The 3-year disease-specific survival rate is around 72%, and the 5-year survival rate for this procedure is around 60%. However, it is well recognized that CFR resection is not a benign procedure and has a significant morbidity, with 33% of patients suffering complications, and a mortality of 4.5%. With the increased usage of the endoscope in the 1990s, the nasal component of the CFR was more commonly performed endoscopically and this procedure was termed a combined endoscopic CFR (CECFR). In 2008, Nicolai and colleagues compared their results for CECFR with wholly endoscopic resection and found that, for adenocarcinoma, the 5-year disease-free survival was 60% compared with 80% for the wholly endoscopic approach. However, the indication for performing a combined approach was in patients who had more extensive tumor, usually with dura and brain invasion, so it is not possible to compare these outcomes.
In the 1990s, reports began to detail wholly endoscopic resection of adenocarcinomas of the sinonasal cavity. Again, most of these publications combined adenocarcinoma with other histologic groups, making true outcome assessment of this new technique difficult ( Table 8 ).
| First Author, Year | Total Cases (n) | Adenocarcinoma (n) | DXT (n) | Recurrence Rate for Entirely Endoscopic Resection (Follow-up is Mean Time for All Patients) |
|---|---|---|---|---|
| Stammberger et al, 1999 | 36 | 7 | — | 5 clear of disease at 30 mo |
| Shah et al, 1999 | 1 | 1 | — | 1 clear of disease at 12 mo |
| Goffart et al, 2000 | 66 | 40 a | 87.9% | 5-y disease-specific survival 57.6% |
| Roh et al, 2004 | 19 | 2 | 78.9% | 1 recurrence at 40 mo |
| Poetker et al, 2005 | 16 | 2 | 0% | No recurrences at 19 mo |
| Batra et al, 2005 | 9 | 2 | 78% | 1 recurrence at 24 mo |
| Lund et al, 2007 | 47 | 14 | 76% | 1 recurrence at 36 mo |
| Podboj and Smid, 2007 | 16 | 5 | 60% | No recurrence at 84 mo |
| Nicolai et al, 2008 | 134 | 44 | 35% | 5-y disease-specific survival 94.4% |
| Bogaerts et al, 2008 | 44 | 44 | 100% | 5-y disease-specific survival 83% |
| Jardeleza et al, 2009 | 12 | 12 | 75% | 91.6% disease-specific survival at 30 mo |
a Some of these patients may have had an additional craniotomy as part of the procedure.
The initial limitations of the wholly endoscopic approach were the ability of the surgeon to access extension of the tumor onto and through the dura and into brain. The stated principles of a wholly endoscopic resection remain the same as those for CFR in that the aim is to achieve a complete local resection to prevent local recurrence. The wholly endoscopic approach is different from the standard CFR approach in that the tumor in the nose is debulked until the tumor attachment is clearly identified. Once this is clear, the surgical approach to resect the entire tumor, including a margin of normal tissue, is planned. New endoscopic techniques for accessing previously difficult regions such as the frontal sinus, areas of the maxillary sinus, and infratemporal fossa are now available. Techniques such as frontal drillout or Draf III procedure allow full access to tumor extension into the frontal sinus or onto the posterior wall of the frontal sinus. Endoscopic medial maxillectomy gives access to the entire maxillary sinus and the infratemporal fossa. The current major controversy is whether the wholly endoscopic resection compromises the outcome by the resection being performed in most instances in a piecemeal fashion. The other area of debate is whether it is necessary to achieve clear margins and whether it is worthwhile documenting such margins during both the endoscopic and CFR approaches. The margins of an anterior skull base resection (either including or excluding the lamina papyracea) are usually bony or cartilaginous and this can make it difficult for the surgeon to obtain a representative sample to send for frozen section. In addition, it has been found that the incidence of recurrence after surgery in patients with positive and negative margins is similar. Because most patients receive postoperative radiotherapy, the positive margins (and normal resection margins) are all included in the postoperative treatment fields. Additional advantages of an endoscopic resection are the improved visualization of the tumor borders provided by the magnification achieved with the use of endoscopes, lack of skin incisions, and lack of resection of normal tissue (maxilla, nasal bones, sinuses) to be able to visualize the extent of the tumor. However, it is well recognized that wholly endoscopic resection of tumors abutting or breaching the normal confines of the sinonasal cavity is technically demanding, that the learning curve for such techniques is significant and takes considerable time to achieve, and that these procedures should not be adopted until such a level of expertise has been developed within the skull base team (see Fig. 2 ).
Conclusion
- •
Endoscopic resection is possible for many tumors
- •
Adjuvant radiotherapy is used for all but very small tumors
- •
Stripping of the tumor from involved structures is not considered standard of care, and involved structures such as the dura should be resected as they would be in tCFR.
Malignant neuroectodermal tumors
Olfactory Neuroblastoma/Esthesioneuroblastoma
Incidence and cause
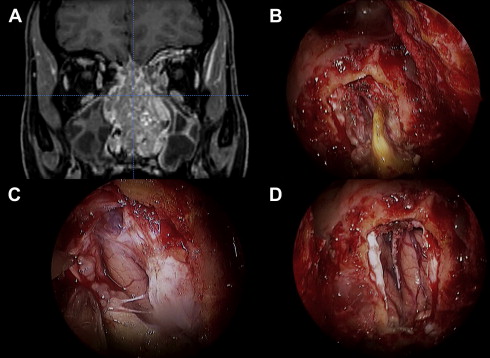
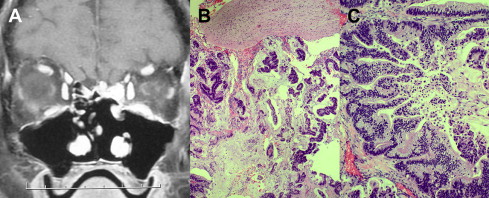
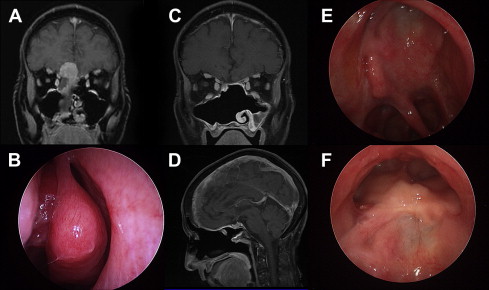
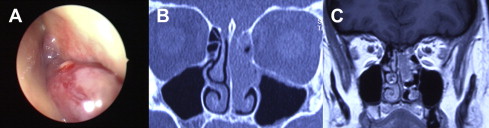
The incidence of olfactory neuroblastoma is difficult to establish, but the tumor is not as rare as is commonly reported, and probably represents more than 5% of all nasal malignant tumors. Olfactory neuroblastoma occurs in a wide age range (3–90 years) with a bimodal peak in the second and sixth decades of life ( Fig. 7 ). Sporadic cases have also been reported in children less than 10 years of age.
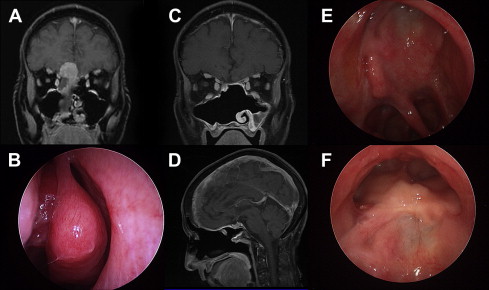
The exact cell of origin of olfactory neuroblastoma is believed to be the basal reserve cell, the olfactory stem cell that gives rise to both the neuronal and the epithelial sustentacular cells. Proposed sources have included Jacobson vomeronasal organ, the sphenopalatine ganglion, the ectodermal olfactory placode, Loci ganglion, autonomic ganglia in the nasal mucosa, and the olfactory epithelium. Although a neuronal or neural crest origin is supported by the presence of neurofilaments in olfactory neuroblastoma, until recently little evidence has linked olfactory neuroblastoma directly to the olfactory epithelium despite the clinical association ( Fig. 8 ).
No known causal factor exists for this tumor, although diethylnitrosamine injections can induce tumors in hamsters at the site of the olfactory epithelium. No hereditary patterns have been described for this neoplasm and there is no apparent racial predilection.
Staging
Kadish and colleagues were the first to propose a staging classification, using 3 categories, group A, B, and C ( Table 9 ). A further system was proposed with the advent of advances in imaging, based on the TNM system ( Table 10 ). Although a system of classification has been proposed, various attempts have been made to modify the Kadish system. Other investigators suggest that, by using the Kadish staging system and the Hyams grading system independently, they can predict patients’ outcome with more accuracy. The Hyams grading system is based on histology and is referred to later.
| Type | Extension |
|---|---|
| A | Tumor limited to the nasal cavity |
| B | Tumor involving the nasal and paranasal sinuses |
| C | Tumor extending beyond the nasal and paranasal sinuses, including involvement of the cribriform plate, base of the skull, orbit cavity, or intracranial cavity |
| D | Tumor with metastasis to cervical nodes or distant sites |
| Stage | Characteristics |
|---|---|
| T1 | Tumor involving the nasal cavity and/or paranasal sinuses (excluding the sphenoid sinus), sparing the most superior ethmoidal cells |
| T2 | Tumor involving the nasal cavity and/or paranasal sinuses (including the sphenoid sinus) with extension to, or erosion of, the cribriform plate |
| T3 | Tumor extending into the orbit or protruding into the anterior cranial fossa, without dural invasion |
| T4 | Tumor involving the brain |
| N0 | No cervical lymph node metastases |
| N1 | Any form of cervical lymph node metastases |
| M0 | No metastases |
| M1 | Any distant metastases |
Treatment and Results
The primary site
A combination of surgery and radiotherapy is the most frequently used approach, and the one that achieved the highest cure rates. Despite the lack of support for single-modality treatment regimes, a substantial number of patients are treated by surgery or radiotherapy alone. The difference in survival between the combined treatments and radiotherapy alone is significant ( Table 11 ). The 5-year disease-specific survival in the literature is between 52% and 90%. Surgery alone was associated with lower survival combined with a combination of radiotherapy and chemotherapy, or triple modality treatment (surgery, radiotherapy, and chemotherapy). Although the results were 15% to 20% better, the differences from the best combination were not statistically significant, probably because of the limited number of patients. These results were complied from the MEDLINE database from the period 1990 to 2000, without language tags. There were 26 treatment studies that formed the basis for the tabulations described earlier, and data extracted from these studies comprised the total number of patients, the staging system used, the patients’ distributions by stage and the histologic grade, and the treatment used. Outcome data consisted of recurrence-free survival at 3 and 5 years; overall survival at 5 and 10 years; and the results by stage, grade, and treatment modality.
| Modality | No. of Patients | Frequency (%) | Survival (%) | Odds Ratio | Confidence Interval |
|---|---|---|---|---|---|
| Surgery alone | 87 | 20 ± 22 | 48 ± 40 | 1.9 | 0.7–4.9 |
| Surgery plus radiotherapy | 169 | 44 ± 20 | 65 ± 25 | 1 | — |
| Radiation alone | 49 | 13 ± 19 | 37 ± 33 | 2.5 | 1.02–6.0 |
| Surgery plus radiotherapy plus chemotherapy | 48 | 7 ± 16 | 47 ± 37 | 2.1 | 0.68–16.5 |
| Radiation plus chemotherapy | 26 | 0 ± 1 | 0 | — | — |
| Chemotherapy | 6 | 2 ± 4 | 40 ± 55 | — | — |
In 5 studies, olfactory neuroblastoma were histopathologically graded and, according to Hyams and colleagues, the mean 5-year survival was 56% (SD 20) in patients with grade I or II tumors and 25% (95% confidence interval [CI] SD 20) in those with grade III or IV tumors. This difference was significant (odds ratio 6.18; 1.30–29.3). In 25 studies that used the Kadish classification, the mean 5-year survival for group A was 72% (SD 41), group B 59% (SD 44), and group C 47% (SD 16). On average, 5% (SD 7) of patients presented with cervical lymph node metastases. In the studies of survival data according to N stage, only 29% of N+ patients were treated successfully, compared with 64% of N0, a significant difference (odds ratio 5.1; 95% CI 1.6–17.0).
Surgery
Most institutions favor surgery as the first treatment modality, followed by radiotherapy.
Endocranial extension and a close relation to the ethmoid roof and cribriform plate have conventionally led to a combined transfacial and neurosurgical approach. CFR allows for an en bloc resection of the tumor with better assessment of any intracranial extension and protection of the brain and optic nerve. The resection should include the entire cribriform plate and crista galli. It is said that the olfactory bulb and overlying dura should be removed with the specimen, although there is no clear evidence to support the assertion that the whole of the bulb should be removed. Open surgery has long been regarded as the gold standard, with results available for decades. A craniotomy is probably not justified for T1 tumors if there is clear radiological evidence of a normal cribriform plate and no involvement of the upper ethmoidal cells, although this clinical picture is seldom seen. The evolution of surgical techniques has created another surgical option in the form of endonasal endoscopic surgery. The use of endoscopic surgery for olfactory neuroblastoma followed by the use of the stereotactic radiosurgical γ knife therapy has recently been used. One report of 10 cases with a mean follow-up of 38 months used endoscopic resection alone without any recurrence, although only 2 had Kadish stage C. In the last decade, numerous articles with small numbers have been published on the endoscopic resection of olfactory neuroblastoma. Devaiah and Andreoli reviewed the literature with a meta-analysis and showed that an endoscopic approach gave a better survival rate. The aim of this study was to compare results of open, endoscopic, endoscopy-assisted, and nonsurgical treatments since the first publication in the literature that mentioned an endoscopic removal. This analysis extracted sufficient data in 361 subjects and the statistically significant results for the full cohort are summarized in Table 12 .
| Treatment A | Number | Treatment B | Number | P |
|---|---|---|---|---|
| Surgery | 279 | No surgery | 52 | <.001 |
| Open surgery | 214 | Endoscopic surgery | 40 | .0019 (endoscopic better) |
| Open surgery | 214 | Endoscopy assisted | 57 | .0123 (endoscopic better) |
Endoscopic surgery produced overall better survival rates than open surgery, with no significant difference between follow-up times in the endoscopic and open surgery groups. Because the gold standard open procedure considerably predated endoscopic treatment, they also grouped the data according to the publication year. The endoscopic surgery group maintained better survival rates ( Table 13 ). These data show evidence for the efficacy of endoscopic surgery in olfactory neuroblastoma. There are more cases of long-term follow-up in the open surgery group than the endoscopic treatment group and most of the open surgery tumors belonged to the Kadish C and D stages, whereas the endoscopic techniques were used more commonly for Kadish A and B tumors. This finding reflects how endoscopic surgery has mainly been used for less extensive lesions, which might not only be a reflection of the size of the tumor but their symptoms, because more extensive lesions might be expected to be more invasive and less differentiated, although this cannot be ascertained from the data available. The most recent publication on endoscopic endonasal resection for all Kadish groups has recently been published by Folbe and colleagues This is a retrospective, multicenter study with 23 patients operated endoscopically, with postoperative radiotherapy in 16 patients. The mean follow-up was 45.2 months with 1 recurrence. The investigators conclude that endoscopic surgery is replacing CFR and that oncological control is not sacrificed when good endoscopic resection techniques are used.
| Treatment A | Number | Treatment B | Number | P |
|---|---|---|---|---|
| Open surgery | 145 | Endoscopic surgery | 40 | .0018 (endoscopic better) |
| Open surgery | 145 | Endoscopy assisted | 57 | .0133 (endoscopic better) |
Radiotherapy
Standard radiotherapy techniques include external megavoltage beam and a 3-field technique; an anterior port is later combined with wedge fields to provide a homogeneous dose distribution. The doses range from 55 Gy to 65 Gy, with most receiving more than 60 Gy. Currently, it is considered that radiotherapy should play a role in the management of olfactory neuroblastoma, particularly in patients who have had incomplete surgical resection or who present with residual disease. In a small retrospective series, a comparison was made between conventional radiotherapy and stereotactically guided conformal radiotherapy (SCRT). It was concluded that SCRT improved target coverage and sparing of organs at risk.
Chemotherapy
Olfactory neuroblastoma is regarded as a chemosensitive tumor based on multiple reported responses to treatment. Neoadjuvant therapy is seldom curative on its own and it may be of no benefit in some patients. Individuals who respond to preoperative chemotherapy have a greater chance of long-term disease-free survival. It has been proposed that Hyams’ grading is an important predictor of response to chemotherapy, and it has been suggested that cisplatin-based chemotherapy is helpful in advanced, high-grade olfactory neuroblastoma and should be considered the treatment of choice in the systemic treatment of these patients.
Neoadjuvant chemotherapy has been advocated for patients with advanced disease at the University of Virginia in a 20-year period. In 34 consecutive patients, two-thirds showed a significant reduction of tumor burden with adjuvant therapy and patients who showed a response to neoadjuvant therapy showed a significantly greater disease-free mortality. Preoperative chemotherapy consisted of cyclophosphamide (650 mg/m 2 ) and vincristine (1.5 mg/m 2 ; maximal dose, 2 mg), administered every 3 weeks for 6 cycles. Adriamycin was used in combination with cyclosphosphamide in 2 patients. Most patients also received a total dose of 50 Gy of preoperative fractionated radiation therapy.
CNS Metastases
CNS metastases (as opposed to direct intracranial extension) can occur in olfactory neuroblastoma. These lesions are believed to arise when tumor cells violate the ependymal epithelium of the ventricles to gain free access to the ventricular fluid. Tumor cells then disseminate through the CSF pathways to distant sites. More than 17 patients identified from the literature had CNS metastases from olfactory neuroblastoma. The trends were found in these patients (1) most patients in whom CNS metastases developed had Kadish stage C disease at diagnosis; (2) there was a highly variable time to onset of CNS metastases, ranging from 1 to 228 months after initial diagnosis of olfactory neuroblastoma; (3) survival after CNS metastases was generally less than 2 years; and (4) the treatment regimen that appeared to result in the longest survival after CNS metastases included surgical resection of the metastatic lesion followed by radiation and/or chemotherapy.
Neck Metastases
Neck metastases are found at presentation in 5% of patients. Such patients should be treated by neck dissection or radiotherapy. It has been estimated from a review of the literature that up to 23.4% may develop cervical lymph node metastases. Thus, treatment of the clinically negative neck may be warranted. In general, an elective neck dissection is not considered because these cervical nodes metastases may not develop for 2 years or more. It is pragmatic to treat them when they are clinically apparent. However, nodal metastases are associated with the development of distant metastases; hence, should these patients undergo an elective neck dissection in advance of the development of metastatic neck disease? The high frequency of occurrence of lymph node metastases is sufficient to refute the claim that olfactory neuroblastoma is a low-grade malignant tumor. Distant metastases synchronous at presentation have been reported in 6.6% (3/45).
Primary Tumor Recurrence
The assessment of recurrent olfactory neuroblastoma at the primary site is usually undertaken with magnetic resonance imaging (MRI). The appearance of the recurrent tumor does not differ from that imaged at initial presentation. Enhanced computed tomography (CT) and MRI images in the coronal plane are helpful in identifying small recurrences and/or intracranial extensions. The meta-analysis by Dulguerov and colleagues found that the 5-year survival of 45% was associated with recurrent disease. Local recurrence in olfactory neuroblastoma occurs in approximately 30%. CFR followed by radiotherapy is associated with fewer recurrences (around 10%). Salvage after local recurrence is possible in 33% to 50% of cases.
Regional and Distant Recurrence
Regional recurrence in the cervical lymph nodes, where the primary site is disease free, occurs in 15% to 20% of cases and is salvageable by treating these in one-third.
Distant metastases with locoregional control are common (8%) and carry a poor prognosis. The time to metastases in varies from 1 to 20 months. Sites involved include the lung, liver, eye, parotid, CNS, bone, vertebrae, and epidural space.
Assessment of Recurrence and Further Treatment
Median survival after recurrence is 12 months, so it is imperative to deal with the primary site initially to minimize the risk of metastatic disease.
There is a delayed neck metastatic rate of 16%, and some consider that this is an indication for elective neck dissection in all cases of olfactory neuroblastoma. Patients with advanced local disease should undergo radiological examination of the neck and may be candidates for regional treatment that may include either treating the neck with radiotherapy or performing an elective neck dissection followed by radiotherapy.
The principle site for distant metastases in one series was bone, with vertebrae being the most common location (86%). Asymptomatic bone metastases were found in 3 patients at presentation coincidentally with a bone scan that was performed after bone marrow biopsies showed aplasia. Hence, a bone scan and bone marrow biopsy should be considered if the likelihood of distant metastases is raised. The significant risk factor for developing distant metastases is the presence of cervical metastases at initial presentation.
There is a single case report of a woman with an olfactory neuroblastoma with epithelial and endocrine differentiation that transformed into a mature ganglioneuroma after chemoradiotherapy.
Recommended Follow-up
Olfactory neuroblastoma is a neoplastic disease with a long natural history characterized by frequent local and regional recurrences after conventional treatment, and so extended follow-up of patients is warranted. The mean time for recurrence is 5 years for evaluating most other cancers of the head and neck, but this is not valid for olfactory neuroblastoma; there the survival data at 10, 15, and even 20 years is important in evaluating the result of treatment.
Girod and colleagues have suggested that MRI with gadolinium should be done 2 to 4 months after completion of all therapy, and should be repeated 4 to 6 monthly for 5 years and then annually for the patient’s lifetime. Continued clinical follow-up is indicated annually thereafter and any symptoms should be investigated. An annual chest radiograph should be performed to exclude the presence of metastases.
Conclusion
- •
The current recommended treatment strategy is:
- ○
Kadish A: –surgery, in selected cases combined with radiotherapy.
- ○
Kadish B: radiotherapy before or after surgery, to the primary tumor site and subclinical lymph nodes. Adjunctive chemotherapy may be added to this treatment depending on the degree of differentiation of the tumor.
- ○
Kadish C/D: preoperative chemotherapy and/or radiotherapy followed by surgery. The use of adjuvant chemotherapy has yet to be further elucidated, as well as the timing of the surgery and the radiotherapy. Surgery may be followed by chemoradiotherapy at centers with extensive skull base experience.
- ○
Malignant neuroectodermal tumors
Olfactory Neuroblastoma/Esthesioneuroblastoma
Incidence and cause
The incidence of olfactory neuroblastoma is difficult to establish, but the tumor is not as rare as is commonly reported, and probably represents more than 5% of all nasal malignant tumors. Olfactory neuroblastoma occurs in a wide age range (3–90 years) with a bimodal peak in the second and sixth decades of life ( Fig. 7 ). Sporadic cases have also been reported in children less than 10 years of age.
The exact cell of origin of olfactory neuroblastoma is believed to be the basal reserve cell, the olfactory stem cell that gives rise to both the neuronal and the epithelial sustentacular cells. Proposed sources have included Jacobson vomeronasal organ, the sphenopalatine ganglion, the ectodermal olfactory placode, Loci ganglion, autonomic ganglia in the nasal mucosa, and the olfactory epithelium. Although a neuronal or neural crest origin is supported by the presence of neurofilaments in olfactory neuroblastoma, until recently little evidence has linked olfactory neuroblastoma directly to the olfactory epithelium despite the clinical association ( Fig. 8 ).
No known causal factor exists for this tumor, although diethylnitrosamine injections can induce tumors in hamsters at the site of the olfactory epithelium. No hereditary patterns have been described for this neoplasm and there is no apparent racial predilection.
Staging
Kadish and colleagues were the first to propose a staging classification, using 3 categories, group A, B, and C ( Table 9 ). A further system was proposed with the advent of advances in imaging, based on the TNM system ( Table 10 ). Although a system of classification has been proposed, various attempts have been made to modify the Kadish system. Other investigators suggest that, by using the Kadish staging system and the Hyams grading system independently, they can predict patients’ outcome with more accuracy. The Hyams grading system is based on histology and is referred to later.



