Local recurrence after primary radiation of nasopharyngeal carcinoma (NPC) remains an important cause of morbidity and mortality. Salvage treatment using reirradiation or surgery has been shown to improve survival over nontreatment. Surgery is traditionally performed using an open approach. Advances in endoscopic approaches for resection of paranasal sinus tumors have been extended to NPC. This article reviews the treatment options, in particular the role of endoscopic nasopharyngectomy in the management of recurrent NPC. The endoscopic anatomy, surgical principles, and published results on endoscopic nasopharyngectomy are presented. Short-term outcomes for early-stage recurrences are promising but long-term follow-up is needed.
Epidemiology of nasopharyngeal carcinoma
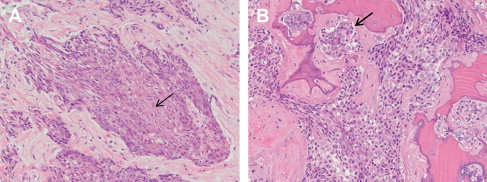
Nasopharyngeal carcinoma (NPC) is an epithelial malignancy that arises within the nasopharynx. It has a distinct racial and geographic distribution, with high prevalence in Southern China and Southeast Asia. The highest rates are registered among Cantonese in the Guangdong province of Southern China (of which Hong Kong is a part). The age-standardized incidence for Hong Kong males is 21.5 per 100,000 persons year. The male/female ratio is 2 to 3:1. NPC can be divided into keratinizing and nonkeratinizing, which is further subdivided into differentiated or undifferentiated ( Fig. 1 ). Most NPC in high-incidence areas is of the nonkeratinizing type and has an etiologic association with Epstein-Barr virus. Most of the literature deals with the nonkeratinizing type, and this type is implied when no distinction is made.
| EBM Question | Level of Evidence | Grade of Recommendation |
|---|---|---|
| What is role of endoscopic surgery for recurrent nasopharyngeal carcinoma? | 4 | C |
Treatment of primary nasopharyngeal carcinoma
NPC is highly radiosensitive and thus the primary treatment of NPC is radiation therapy. Early disease (stage I and II) NPC is treated with radiation alone whereas advanced disease (stage III and IV) is treated with concomitant chemoradiation. With advances in radiotherapy planning and delivery techniques such as intensity-modulated radiotherapy (IMRT) and the use of chemoradiation, a 5-year local control rate of 76% to 91% can be achieved. Nevertheless, local recurrence remains a common sign of treatment failure and a major cause of morbidity and mortality.
Treatment of primary nasopharyngeal carcinoma
NPC is highly radiosensitive and thus the primary treatment of NPC is radiation therapy. Early disease (stage I and II) NPC is treated with radiation alone whereas advanced disease (stage III and IV) is treated with concomitant chemoradiation. With advances in radiotherapy planning and delivery techniques such as intensity-modulated radiotherapy (IMRT) and the use of chemoradiation, a 5-year local control rate of 76% to 91% can be achieved. Nevertheless, local recurrence remains a common sign of treatment failure and a major cause of morbidity and mortality.
Investigations
The diagnosis of a recurrence is based on endoscopic or radiological detection of a suspicious mass in the nasopharynx followed by histologic confirmation. Detection of recurrence using traditional computed tomography (CT) or magnetic resonance imaging (MRI) can be challenging. Changes to nasopharyngeal tissue after radiotherapy such as edema, loss of tissue planes, fibrosis, and scarring can obscure the detection of tumor recurrence. Both CT and MRI scans have been reported to have a low sensitivity and moderate specificity in differentiating tumor recurrence from posttherapy changes. Positron emission tomography (PET) using fluorodeoxyglucose, apart from its use in the detection of distant metastases, has been shown to be more sensitive than both MRI and CT scan in detecting residual or recurrent tumor. In addition, combined PET/CT imaging can give accurate localization of focal uptake, allowing distinction of disease from normal physiology and better treatment planning.
Prognosis
Aggressive salvage treatment of local recurrence is warranted because patients can achieve reasonable long-term survival after salvage therapy. Patients who receive salvage treatment had a significantly better overall survival than those who did not receive salvage treatment.
This review examines the various treatment options available, in particular the role of endoscopic nasopharyngectomy in the salvage of locally recurrent NPC.
Management of recurrent nasopharyngeal carcinoma
Management of recurrent NPC remains challenging. Early detection of recurrent disease is essential for any form of salvage therapy to be successful. Current treatment options include reirradiation, chemotherapy, or surgery. The role of chemotherapy alone is primarily reserved for palliation in patients not suitable for radical radiation therapy or a nasopharyngectomy.
Radiotherapy for recurrent nasopharyngeal carcinoma
Reirradiation options include external beam radiotherapy (conventional two-dimensional radiotherapy, three-dimensional [3D] conformal radiotherapy, IMRT, and stereotactic radiotherapy) with or without brachytherapy. Reirradiation of local recurrences using traditional external beam irradiation can result in further 5-year survival rates of 8% to 36%. There is a significant correlation between the dose at reirradiation and the salvage rate; a higher local control rate is achieved with a dose of at least 60 Gy. As a result of a high cumulative radiation dose, late complications are frequent and have been reported in 26% to 57% of patients. Radiation-related complications included multiple cranial nerve palsies, temporal lobe necrosis, osteoradionecrosis, xerostomia, trismus, soft tissue fibrosis, hearing and visual impairment, endocrine dysfunction, and even carotid rupture. The treatment mortality ranged from 1.8% to 9.4% and was related mainly to neurologic damage. Newer treatment modalities such as the 3D conformational radiation, IMRT, and stereotactic irradiation aim to deliver more precise tumor coverage and spare critical nearby structures, thereby reducing the incidence of late complications.
Anatomy of the nasopharynx
It is essential to understand the complex anatomic relationships of the nasopharynx regardless of the surgical approach used. The nasopharynx is a narrow space located posterior to the nasal cavity and sits above the soft palate. It is bounded superiorly by the sphenoid sinus and upper clivus and posteriorly by the lower clivus and the first cervical vertebra. Anterolaterally, it is bounded by the medial pterygoid plate. Posterior to the medial pterygoid plate is the sinus of Morgagni. Internally the nasopharynx is covered by mucosal, and the pharyngobasilar fascia lies deep to it. The pharyngobasilar or pharyngeal fascia is a tough fascia that connects the superior constrictor muscle to the skull base. It originates from the pharyngeal tubercle of the occipital bone posteriorly and attaches to the posterior edge of the medial pterygoid plates anteriorly. The tensor veli palatini and the cartilaginous portion of the Eustachian tube pass through the sinus of Morgagni by traversing through the pharyngobasilar fascia. Posterior to the Eustachian tube along the lateral wall is the fossa of Rosenmuller, where NPC typically originates. When the tumor invades laterally through the sinus of Morgagni, it extends along the Eustachian tube and involves the parapharyngeal space and foramen ovale area. This situation results in a constellation of symptoms:
- •
Ipsilateral conductive hearing loss
- •
Ipsilateral akinesia of the soft palate
- •
Ipsilateral trigeminal (mandibular) neuralgia, also known as Trotter syndrome
The biggest risk in this surgery is the proximity of the parapharyngeal internal carotid artery (ICA) to the nasopharynx. Identification of key surgical landmarks and their relationship to the ICA minimizes the risk of injuring the carotid artery. Wen and colleagues presented a detailed endoscopic anatomy of the nasopharynx and highlighted several landmarks. They found that osseous landmarks, such as the medial pterygoid plate, foramen lacerum, and the isthmus of the Eustachian tube, along with the muscular landmarks (longus capitis), all lead to the ICA.
Preoperative evaluation of nasopharyngeal carcinoma
Patients are restaged using a combination of CT and MRI, each providing complementary information about bone erosion and soft tissue invasion ( Figs. 2 and 3 ). The limiting factor for surgery is tumor involvement of the ICA in its petrous or parapharyngeal segment. When tumor is in contact with the ICA, surgical options include dissection of tumor from the artery with preservation of the ICA or sacrifice of the ICA to obtain a clear resection margin. The ability of the patient to tolerate sacrifice of the ICA is assessed with a balloon occlusion test with neuromonitoring ( Fig. 4 ). If the patient tolerates temporary occlusion without a neurologic deficit or evidence of decreased cerebral perfusion, permanent occlusion can be performed with low risk of a delayed stroke. On the other hand, if the patient fails the balloon occlusion test, the goals of surgery need to be modified or alternative therapy should be considered.
Surgery for recurrent nasopharyngeal carcinoma
Surgery presents a reasonable choice when the recurrent tumor is resectable. It gives satisfactory local control with a 5-year survival rate between 30% and 52% and there is less morbidity than high-dose reirradiation.
Access to the nasopharynx has always been difficult and is traditionally achieved with an open approach. Depending on the extent and site of the recurrent NPC, various approaches have been developed to facilitate adequate surgical resection, including transpalatal, maxillary swing, transmandibular, facial translocation, and transinfratemporal fossa approaches. These approaches are complex and may result in considerable morbidity, including facial scarring, trismus, dental malocclusion, injury to cranial nerves (infraorbital nerve in the maxillary swing, lingual nerve in the mandibular swing, both in facial translocation, facial palsies with infratemporal fossa approaches), palatal defects, dysphagia, nasal regurgitation, osteonecrosis, osteomyelitis, and even rupture of the ICA.
In an attempt to reduce the morbidities associated with open surgical approaches, minimally invasive techniques have emerged. To and colleagues described a midfacial degloving transnasal approach, which avoided a facial incision. This approach was coupled with the use of stereotactic navigation for precise localization of the ICA. The investigators were able to achieve tumor clearance in 12 of 15 patients. The 3 remaining patients had their tumors stuck to the ICA. No follow-up data were available. In a follow-up publication, To and colleagues compared this technique with a conventional open transfacial approach. There appeared to be fewer mortalities and morbidities in the minimally invasive group. However, the staging of the recurrent tumor in each group of patients was not indicated, and no follow-up data were available.
Roh and Park described a transseptal approach similar to a conventional transseptal hypophysectomy to gain access to the nasopharynx. By inserting a bivalve speculum between the mucoperichondrial flaps, and with the aid of a microscope and CO 2 laser the investigators achieved complete resection of tumors in 3 patients with recurrent T1 NPC. There was no recurrence during a follow-up period of 12 to 28 months.
Endoscopes have revolutionized the approach to diseases involving the nasal cavity and the sinuses. The advantages include avoidance of a facial scar, less destruction of the surrounding tissues, and possibly better preservation of function. With increasing experience and expertise, the indications have also expanded rapidly from dealing with benign pathologies to sinonasal malignancies. Anterior skull base tumors such as olfactory neuroblastoma can now be safely resected with an endoscopic craniofacial resection, maintaining the same oncologic principles as in open surgery. Early results on endoscopic resection of sinonasal malignancies are promising. The limits of endoscopic surgical techniques are constantly evolving and now include diseases involving sites such as the infratemporal fossa and nasopharynx.
The endoscope is well suited for the nasopharynx. Improvement in the optics of the rod-lens endoscope, coupled with high-resolution cameras and monitors, have allowed excellent visualization of this area. Reliability of intraoperative navigational devices, the use of extended endonasal instruments, and better understanding of endoscopic anatomy of the nasopharynx have made endoscopic nasopharyngectomy safe and feasible.
Principles of endoscopic nasopharyngectomy
The surgical margin status is an important prognostic factor for both local control and overall survival for surgical salvage of recurrent NPC. The ability to achieve clearance is dictated by the recurrent T stage, involvement of vital anatomic structures, and the ability to obtain adequate surgical exposure. The widest possible exposure offers the best opportunity to achieve complete resection with negative margins. This oncologic principle is also applicable to endoscopic surgery. Greater exposure can be achieved by resecting the posterior half of the septum (vomer) and reduction of the inferior turbinates. This strategy allows the whole nasopharynx to be visualized. The need for further exposure depends on the site and extent of the tumor.
Castelnuovo and colleagues described a modulated approach to the nasopharynx. Depending on the tumor extent, these investigators classified nasopharyngeal tumor resections into 3 types. Type 1 resection was the most conservative. The incision began superiorly from the nasopharyngeal vault, down along the posterior border of the torus into the fossa of Rosenmuller, and horizontally across at the level of the atlas. The Eustachian tube was preserved. Posteriorly the resection extended deep to the periosteum of the skull base, and the ventral part of the clivus was drilled out. This resection was suitable for small tumors centrally located in the nasopharynx. Type 2 was for tumors involving the roof of the nasopharynx, and the exposure was extended superiorly into the sphenoid sinus. Bilateral sphenoidectomies and removal of the rostrum allowed access into the sphenoid sinuses. The floor of the sinus was entirely drilled to the coronal plane of the clivus. The rest of the resection was similar to type 1. Type 3 was the most extensive, and the resection includes the lateral nasopharyngeal wall up to the parapharyngeal space and the ipsilateral cartilaginous portion of the Eustachian tube. A complete ethmoidectomy and a modified medial maxillectomy followed by drilling of the medial pterygoid plate were performed. An angled probe was placed into the Eustachian tube, and the cartilaginous portion was then removed up to its bony junction. This is a critical landmark because the parapharyngeal ICA lies just posterior to the bony Eustachian tube landmark and hence is at risk if the resection is carried beyond this point.
All-Sheibani and colleagues also described a similar endonasal transpterygoid approach to the nasopharynx. An endoscopic medial maxillectomy supplemented by an endoscopic Denker approach allowed the removal of the posterior and lateral walls of the maxillary antrum. This procedure was followed by mobilization of the soft tissue contents of the pterygopalatine fossa laterally and removal of the pterygoid process and cartilaginous Eustachian tube. Again, this approach allowed control of the parapharyngeal and petrous segments of the ICA, thus allowing tumors in the fossa of Rosenmuller and infratemporal fossa to be safely resected.
If resection of the ICA is necessary to achieve a clear margin, this can be performed endoscopically if the artery is sacrificed preoperatively using endovascular techniques. Even so, this part of the operation may be facilitated by a combined open (infratemporal skull base) and endoscopic approach.
After a nasopharyngectomy, once the surgical margins are confirmed with frozen sections, consideration should be given to the reconstruction. The wound can be left to heal by secondary intention or alternatively it can be covered with either free mucosal or a pedicled turbinate graft. The latter allows for faster mucosalization. Coverage of heavily irradiated tissue with vascularized tissue speeds the healing process and decreases the risk of wound healing complications and postoperative headache. For large defects with an exposed ICA, a temporalis muscle transposition (combined approach) provides ample coverage.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


