Purpose
To evaluate the therapeutic efficacy of topical interleukin-1 receptor antagonist (IL-1Ra) in the treatment of dry eye disease.
Design
Laboratory investigation.
Methods
Dry eye disease was induced in C57BL/6 female mice through exposure to a desiccating environment within a controlled environment chamber. Topical formulations containing 5% IL-1Ra, 1% methylprednisolone, 0.05% cyclosporin A, and a vehicle control containing carboxymethylcellulose sodium were applied after the induction of dry eye. Corneal fluorescein staining was performed by a masked observer in the different treatment groups. Immunohistochemical studies were undertaken to enumerate corneal CD11b+ cells, as well as to evaluate corneal lymphangiogenesis. Real-time polymerase reaction was used to quantify the expression of interleukin-1β in the cornea.
Results
A significant decrease in corneal fluorescein staining was observed after topical treatment with 5% IL-1Ra ( P < .01), 1% methylprednisolone ( P < .01), and 0.05% cyclosporin A ( P < .03). Additionally, a significant decrease in the numbers of central corneal CD11b+ cells ( P < .05), corneal lymphatic growth ( P < .05), and corneal interleukin-1β expression ( P < .003), compared with vehicle treated, were demonstrated only after treatment with 5% IL-1Ra and 1% methylprednisolone, and were absent after cyclosporin A treatment.
Conclusions
Topical treatment with IL-1Ra is effective in ameliorating the clinical signs of the dry eye disease, as well as in reducing underlying inflammation. These effects are comparable with those resulting from treatment with topical methylprednisolone. Topical IL-1Ra may hold promise as a novel therapeutic strategy in the treatment of dry eye.
Dry eye disease (DED) is an extremely common ocular disorder, and large epidemiologic studies, using a variety of definitions, have estimated its prevalence at approximately 10% to 20% of the adult population. DED is defined as a multifactorial condition of the tears and ocular surface, characterized by symptoms of discomfort, visual disturbance, and tear film instability, with potential damage to the ocular surface. Moreover, it is accompanied by increased osmolarity of the tear film and inflammation of the ocular surface. DED can affect visual function, and thus common tasks of daily living such as reading, speed, and driving are affected adversely by this condition.
Inflammation has been recognized as an important component of DED, and anti-inflammatory therapies have therefore proven useful in decreasing ocular surface inflammation, stimulating tear production, and improving the overall signs and symptoms of dry eye. Moreover, consistent with the concept that inflammation is a key feature in the pathophysiology of DED is the finding that the clinical signs and symptoms of dry eye improve with methylprednisolone and cyclosporin (CsA). Unfortunately the long-term use of topical corticosteroids is limited by potential sight-threatening side effects, such as glaucoma, cataract, and infection. Furthermore, CsA, the only drug approved by the Food and Drug Administration in the United States for treatment of DED, is associated in some patients with a burning and stinging sensation and requires several months to produce a clinical therapeutic effect.
Interleukin-1 receptor antagonist (IL-1Ra) is an endogenous IL-1 receptor antagonist, which is produced primarily by activated monocytes and tissue macrophages, and inhibits the activities of the proinflammatory forms of IL-1 (IL-1α and IL-1β) by competitively binding to the IL-1 receptor-I. IL-1Ra is typically upregulated in inflammatory conditions, such as in rheumatoid arthritis, to down-modulate the inflammatory functions of the IL-1 receptor-I ligation by the agonistic ligands, IL-1α and IL-1β. Although the binding affinity of natural IL-1Ra to its receptor is similar to that of IL-1α and IL-1β, higher concentrations of IL-1Ra relative to agonistic IL-1 ligands have been shown to be required to inhibit completely the cellular effects of IL-1. This is probably because only 5% receptor availability for IL-1 can initiate inflammatory responses, and thus virtually all cellular IL-1 receptor-I receptors must be blocked for sufficient suppression of the IL-1 system. Normal tear fluid has been found to contain high concentrations of IL-1Ra in concentrations 25 000 and 40 000 times greater than both proinflammatory forms of IL-1, and it is thought that concentration of IL-1Ra in the tear fluid may therefore be a natural homeostatic mechanism for regulation of IL-1–mediated functions on the ocular surface.
Given the critical role of inflammation in the pathogenesis of DED, we examined the therapeutic efficacy of topical IL-1Ra in DED using a validated murine model of dry eye. Our data show a significant amelioration of clinical signs of DED in IL-1Ra–treated mice. In addition, we investigated the effect of topical IL-1Ra in modulating infiltration of inflammatory cells, expression of inflammatory cytokine, and lymphangiogenesis in dry eye cornea—mechanisms that are of pathophysiologic relevance in DED induction and progression —and demonstrate significant suppression of DED-associated inflammation with topical use of IL-1Ra.
Methods
Animals
Eight- to 10-week-old female C57BL/6 mice (Charles River Laboratory, Wilmington, Massachusetts, USA) were used in this study.
Induction of Dry Eye
Dry eye was induced in the mice by placing them in a controlled environment chamber (CEC), which allows continuous regulation of relative humidity below 30%, a constant temperature of 21 to 23 C and airflow of 15 L/minute, 24 hours per day. To achieve maximum ocular surface dryness, the conditions in CEC were supplemented with topical application of 1% atropine sulfate (Falcon Pharma, Fort Worth, Texas, USA) twice daily for the first 48 hours. Additionally, the mice also received on their dorsal surface subcutaneous injections 0.1 mL (5 mg/mL) of scopolamine hydrobromide (Sigma-Aldrich, St. Louis, Missouri, USA) to exacerbate dry eye 3 times daily (9 am, 1 pm, and 5 pm) for the entire duration of the experiment.
Topical Formulations and Treatment Regimen
The formulations tested included 5% IL-1Ra, 1% methylprednisolone, 0.05% CsA (Restasis; Allergan, Irvine, California, USA). The topical IL-1Ra and methylprednisolone were formulated aseptically from the commercially available anakinra (Kineret; Biovitrum, Stockholm, Sweden) and methylprednisolone sodium succinate, respectively, and transferred into a sterile, light-protected dropper container. Anakinra (50 mg/mL) was diluted in carboxymethylcellulose sodium (Refresh Liquigel; Allergan) and methylprednisolone (10 mg/mL) was diluted in nonpreserved sterile normal saline solution. Forty-eight hours after the induction of dry eye, the mice in the CEC were divided randomly into 5 different groups (n = 8 to 10 in each group): (1) an untreated group, (2) a group receiving topical vehicle control (carboxymethylcellulose sodium), (3) a group receiving 5% IL-1Ra, (4) a group receiving 0.05% CsA, and (5) a group receiving 1% methylprednisolone. Three microliters of the eye drop were applied topically to both eyes of unanesthetized mice 3 times daily from 48 hours to day 9 (total, 21 doses). The untreated group received no eye drops. Ocular signs of dry eye were evaluated using fluorescein staining at day 2, day 6, and day 9. Mice then were sacrificed on day 10 for cellular and molecular studies.
Corneal Fluorescein Staining
Fluorescein staining of the corneal epithelium was used as a diagnostic tool to study the effect of desiccating stress on the ocular surface of the mice. Corneal fluorescein staining was performed at baseline (day 0, before placing the mice in the CEC), day 2 (before instillation of topical therapy), day 6, and finally at day 9. Using a micropipette, 0.7 μL 2.5% fluorescein (Sigma-Aldrich) was applied to the eye into the inferior conjunctival sac (n = 8 eyes per group,) as previously described. After 3 minutes, punctate staining on the corneal surface was evaluated in a masked fashion using a slit-lamp biomicroscope under cobalt blue light. The National Eye Institute grading system was used to assess the corneal surface staining.
RNA Isolation and Molecular Analysis Using Real-Time Polymerase Chain Reaction
Total RNA was isolated from the cornea tissues using the RNeasy Microkit (catalog no. 74004; Qiagen, Valencia, California). Two corneas per group were isolated, pooled together, and stored at −80 C in Trizol (catalog no. 15596026; Invitrogen, Carlsbad, California) until future use. The first strand of complementary DNA was synthesized with random hexamers using SuperScript III Reverse Trancriptase (catalog no. 18080; Invitrogen) according to the manufacturer’s recommendations and using 500 ng total RNA. Real-time polymerase chain reaction analysis was performed using FAM-MGB dye-labeled predesigned primers (Applied Biosystem, Foster City, California, USA) for glyceraldehyde 3-phosphate dehydrogenase (assay ID.Mm99999915_g1) and IL-1β (assay ID.Mm00434228_m1). In each well, 2.5 μL complementary DNA was loaded, and assays were performed in duplicates. A nontemplate control was included in all the experiments to evaluate DNA contamination of the reagent used. The glyceraldehyde 3-phosphate dehydrogenase gene was used as the endogenous reference for each reaction. The results were normalized by the cycle threshold (CT) of glyceraldehyde 3-phosphate dehydrogenase, and the relative mRNA level in the untreated group was used as the normalized control for the other groups.
Immunohistochemical Staining
The following primary antibodies were used for immunohistochemical staining: rat antimouse CD11b-FITC for monocytes/macrophages (1:100; BD Pharmingen, San Diego, California), goat antimouse CD31 FITC as panendothelial marker (1:100; Santa Cruz Biotechnology, Santa Cruz, California), and purified rabbit antimouse LYVE-1 as lymphatic endothelial marker (1:400; Abcam, Cambridge, Massachusetts, USA). Respective isotypes were used as negative controls. The secondary antibody used was Rhodamine conjugated goat antirabbit (1:100; BD Pharmingen). For whole mount immunofluorescence corneal staining, freshly excised corneas were washed in phosphate-buffered saline and acetone fixed for 15 minutes and then stained with CD11b or double-stained with CD31 and LYVE-1 as described previously. To analyze infiltration of CD11b + cells, corneas from 3 mice from each group were taken and cells were counted in 6 areas in the periphery (0.5 μm area from the limbus) and the center (central 2 μm area) of the cornea in a masked fashion, using a confocal microscope (Leica TCS 4D; Lasertechnik, Heidelberg, Germany) at ×40 magnification. The mean number of cells was obtained by averaging the total number of cells in all the areas studied, and the result was expressed as the number of positive cells per square millimeter.
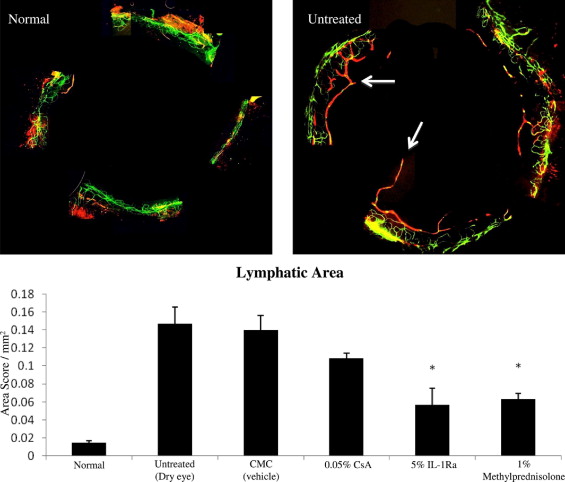
Quantification of Corneal Lymphangiogenesis
The lymphatics were analyzed by an automated image analysis program using Matlab (The Mathworks Inc, Natick, Massachusetts, USA). Lymphatics were isolated from 12 digitized immunofluorescent micrographs with this program and subsequently analyzed the lymphatic area (LA). LA represents the total surface area of the lymphatic vessels when projected into the plane of the image.
Statistical Analysis
A 2-tailed Student t test was performed, and P values of less than .05 were deemed statistically significant. Results are presented as the mean ± standard error of the mean of at least 3 experiments.
Results
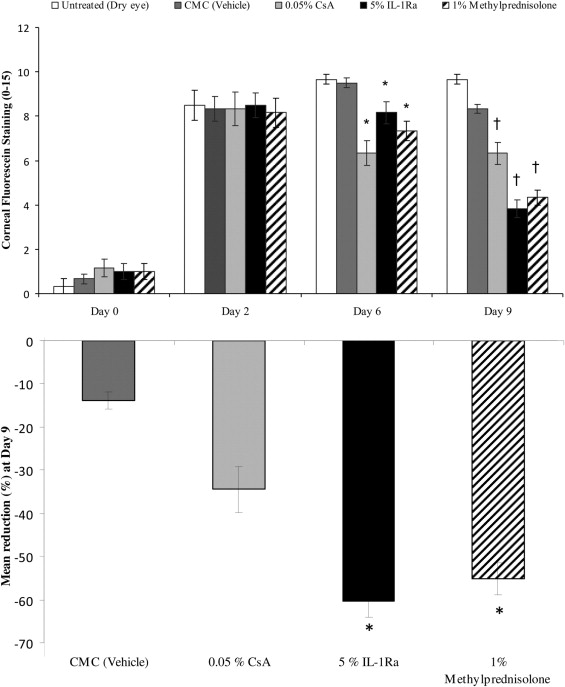
Amelioration of Clinical Signs of Dry Eye
The clinical signs of dry eye were measured by corneal fluorescein staining using the National Eye Institute grading scheme. On day 0, mice were placed in the CEC, and after 48 hours, all mice showed an increase in corneal staining corresponding to dry eye induction ( Figure 1 , Top). Topical treatment with the 5% IL-1Ra, 1% methylprednisolone, 0.05% CsA, and the vehicle control (carboxymethylcellulose sodium) were started on day 2, and corneal fluorescein staining scores were measured at days 6 and 9. Treatment with topical 5% IL-1Ra, 1% methylprednisolone, and 0.05% CsA led to a significant decrease in corneal fluorescein staining compared with the untreated and vehicle group at day 6 ( P < .01) and day 9 ( P < .003; Figure 1 , Top). Moreover, 5% IL-1Ra and 1% methylprednisolone showed a statistically significantly greater reduction in the CFS score compared with 0.05% CsA at day 9 (55% and 60% vs 34%, respectively; P < .01; Figure 1 , Bottom).
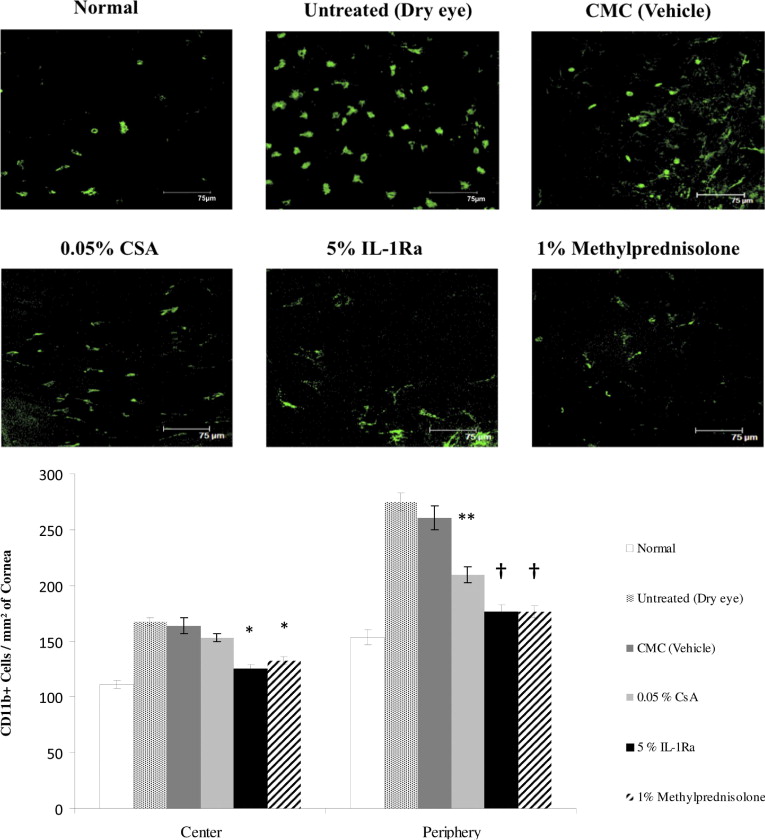
Reduction of CD11B + Cells Infiltration in Dry Eye Cornea
The normal cornea has a resident population of bone marrow-derived immature CD11b + antigen-presenting cells (APC), and the induction of dry eye is associated with a significant increase in the number of corneal CD11b + cells. Using confocal microscopy of corneal whole mounts, we investigated CD11b + cells infiltrating the cornea of different regimen-treated groups ( Figure 2 , Top). A significant decrease was seen in the number of CD11b + cells, both in the periphery and the center, of dry eye corneas that were treated with 5% IL-1Ra (176.2 ± 6.5 and 125.0 ± 3.4) and 1% methylprednisolone (176.1 ± 5.4 and 132.1 ± 3.5) compared with vehicle-treated dry eye corneas (260.7 ± 11.0 and 164 ± 7.1; Figure 2 , Bottom). However, the 0.05% CsA-treated group showed only a significant decrease in the number of CD11b + cells in the peripheral corneas compared with vehicle-treated corneas (209.5 ± 6.8 vs 260.7 ± 11.0; P = .004; Figure 2 , Bottom). No difference in the CD11b + cell numbers was observed between untreated and vehicle-treated dry eye corneas.
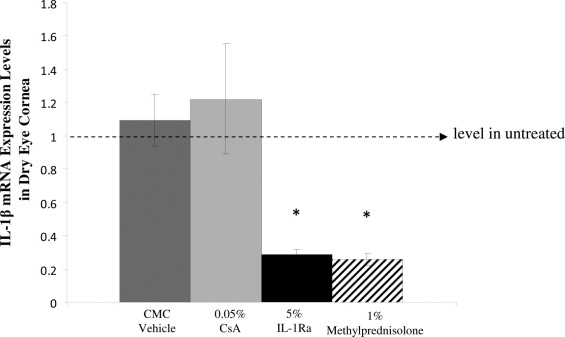
Reduction in the Expression of Interleukin-1β in Dry Eye Cornea
DED is accompanied by an increase in the proinflammatory forms of IL-1. Therefore, to determine the relative efficacy of the different treatment regimens on the gene expression of IL-1β, real-time polymerase chain reaction analysis was performed to quantify the transcript expression of IL-1β in the cornea of different groups (n = 4 to 6 per group). Analysis of relative expression of IL-1β among different groups showed that treatment with 5% IL-Ra and 1% methylprednisolone decreased significantly the levels of IL-1β in the cornea compared with groups treated with CsA ( P = .02) and vehicle control ( P = .003; Figure 3 ) .
Inhibition of Lymphatics Ingrowth in Dry Eye Cornea
The normal human cornea is avascular and alymphatic, thus suppressing both the afferent (lymphatic) and efferent (vascular) arms of the immune cycle. The lymphatic system plays an essential role in generating immune-inflammatory responses by directing the antigen-bearing immunocytes (e.g., dendritic cells) from the periphery to the draining lymph nodes, where the T cells are primed and expanded. Our data on corneal lymphatic ingrowth showed a significant increase in the LA in the dry eye corneas compared with normal corneas (0.14 ± 0.018 vs 0.01 ± 0.002, respectively; P = .02; Figure 4 , Top). A significant decrease in the LA was observed only in groups treated with 5% IL-1Ra (0.05 ± 0.001) and 1% methylprednisolone (0.06 ± 0.006) compared with the vehicle-treated group (0.14 ± 0.01; P < .04; Figure 4 , Bottom).