Purpose
To develop a novel method of posterior fixation suture augmented by the application of Marlex mesh and to evaluate the surgical results in a rabbit model.
Design
Animal study.
Methods
setting: Prospective, masked-observer, controlled experimental study. study population: Sixty superior rectus muscles of 30 rabbits. intervention: Each superior rectus muscle was randomly subjected to posterior fixation suture at a distance of 6 mm from the muscle insertion. The rabbits were divided into 3 groups: conventional posterior fixation suture (Conventional group), and modified posterior fixation suture using a silicone sponge (Silicone group) or using Marlex mesh (Marlex group). Nonabsorbable sutures were used for muscle-sclera (Conventional group) or muscle-implant fixation (Silicone and Marlex group) and absorbable sutures were used for implant-sclera fixation (Silicone and Marlex group). main outcome measures: The efficacy of posterior fixation suture was determined by forced duction testing toward the operated-on muscle immediately after the operation and at 8 weeks postoperatively. Eyes were enucleated at 8 weeks after surgery to measure the stability of the bond using a push pull gauge, and finally the histologic findings were evaluated.
Results
Immediately after posterior fixation suture and at 8 weeks postoperatively, the restrictive motion during duction toward the operated-on muscle was greater in the Marlex group compared to the other groups ( P < .001). The resistance to separation of the myoscleral union was greatest in the Marlex group ( P < .001).
Conclusions
Posterior fixation suture can be effectively reinforced and stabilized using Marlex mesh.
Posterior fixation of the extraocular muscle, also known as the faden operation, is designed to weaken the muscle only in its field of action without affecting the ocular alignment of the primary gaze. Magnetic resonance imaging (MRI) has revealed the major role of pulleys in the mechanical behavior of the extraocular muscles, and the effect of posterior fixation suture can be better explained by the passive elastic force and mechanical restriction caused by the pulley sleeves during duction toward the operated-on muscle.
In this study, we designed a novel method of posterior fixation suture reinforced with surgical mesh in a rabbit model to enhance the one-way weakening effect of posterior fixation suture by increasing the restrictive motion of pulleys in the field of action, and to improve its long-term effect by stabilizing the suture. Marlex mesh (C. R. Bard, Covington, Georgia, USA) is a nonabsorbable polypropylene mesh widely used in hernia repair. Monofilament polypropylene is the most commonly used material for surgical meshes, because of its inert and nonantigenic characteristics, inherent strength, and low infection rate owing to its hydrophobic surface. A previous study demonstrated that it was an ideal implant for repairing early blow-out fracture with minimal resultant complications. Therefore, Marlex mesh was chosen for its high mechanical stability and low risk of infection. As for the controls, a Conventional group of posterior fixation suture was set to compare the efficacy of the new procedure. The introduction of an external implant would be expected to cause more inflammation or foreign body reaction than a simple fixation suture. To determine the safety of Marlex mesh in ocular tissues, we set another control group using a safe surgical implant widely used in ocular tissues. Silicone sponge was selected as it has long been used in scleral buckling surgery, with tolerable complications and minimal host reaction.
The efficacy of the modified method was measured by the mechanical restriction toward the field of action based on the pulley theory, and stability was estimated by the resistance of the myoscleral union to separation. Histologic findings were evaluated for fibrosis, inflammation, and foreign body reactions in all 3 groups and their results were compared.
Materials and Methods
Thirty healthy New Zealand white rabbits (1.5-2.0 kg) underwent faden operation 6 mm posterior to the insertion of both superior rectus muscles with the use of nonabsorbable 5-0 polyester sutures (5-0 Ethibond; Ethicon, Somerville, New Jersey, USA) and absorbable 6-0 polyglactin sutures (6-0 Vicryl; Ethicon). Sixty superior rectus muscles were divided among 3 experimental groups: conventional posterior fixation (Conventional group), modified posterior fixation using a silicone sponge (Silicone group), or modified posterior fixation suture using Marlex mesh (Marlex group). In the Silicone group and the Marlex group, posterior fixation suture was accomplished in an indirect fashion, as the muscle was sutured to the implant, and then the implant was fixed to the sclera. Each superior rectus muscle underwent 1 of the 3 different procedures, and the 2 eyes of each rabbit were randomly assigned to minimize inter-rabbit variation.
Procedures
General anesthesia was induced by administering 30 to 45 mg/kg ketamine hydrochloride (Ketalar; Yuhan Co, Seoul, Korea) and 5 to 10 mg/kg xylazine hydrochloride (Rompun; Bayer Korea, Seoul, Korea) intramuscularly, and topical anesthesia was achieved using proparacaine hydrochloride. Polyvinylpyrrolidone-iodine was applied to the eyelids for preoperative surgical antisepsis. A limbal peritomy was created from 10 o’clock to 2 o’clock. The superior rectus muscle was isolated on a Jameson hook, and the intermuscular connections were dissected. The superior oblique tendon was disinserted and allowed to retract from the surgical field.
In the Conventional group, 2 points were marked on the sclera and superior rectus muscle, 6 mm from the insertion point, and 2 nonabsorbable 5-0 polyester sutures were placed for posterior fixation suture. Each suture incorporated one third of the muscle belly at its lateral borders and was sutured to the sclera via a 2-mm-length tract. These points were located near the equator of the globe, sufficiently posterior to reproduce the usual complications of posterior fixation sutures. The retroequatorial region was avoided because the retractor bulbi muscle insertion point is nearby.
In the Silicone group, an oblong silicone sponge (DORC International BV, Zuidland, The Netherlands) (3.5 mm × 7.5 mm) was cut into 10-mm-length fragments. Each piece was horizontally sliced in half, leaving a hinge at 1 end, and the superior rectus muscle was enclosed between its upper and lower body. The center of the sponge was placed 6 mm posterior to the muscle insertion. To secure the implant with the muscle, the upper and lower bodies of the silicone sponge were sutured together, incorporating the muscle belly at its center using nonabsorbable 5-0 polyester sutures. Finally, 2 posterior fixation sutures were placed incorporating the lateral borders of the upper and lower body of the sponge, and were sutured to the sclera via a 2-mm-length tract using absorbable 6-0 polyglactin sutures ( Figure 1 , Top left and Bottom left).
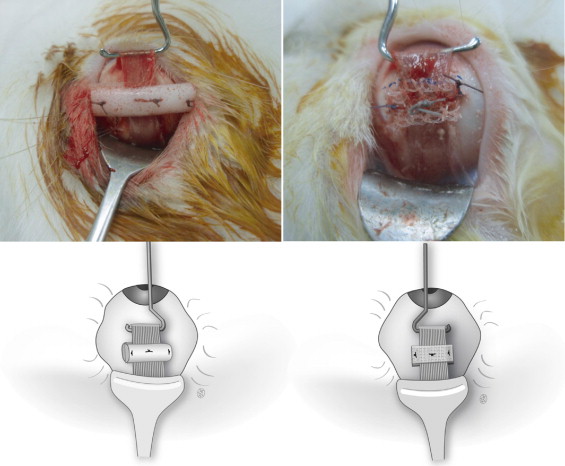
In the Marlex group, posterior fixation was reinforced using Marlex mesh. First, the Marlex mesh was cut into 7.5 × 10-mm pieces. Two pieces were used as a pair to envelop the superior rectus muscle. The center of the meshes were placed 6 mm posterior to the muscle insertion point. To secure the implant with the muscle, the upper and lower pieces of the Marlex mesh were sutured together, incorporating the muscle belly at its center, using nonabsorbable 5-0 polyester sutures. Finally, 2 posterior fixation sutures were placed incorporating the lateral borders of the upper and lower meshes, and were sutured to the sclera via a 2-mm-length tract using absorbable 6-0 polyglactin sutures ( Figure 1 , Top right and Bottom right).
The conjunctiva was closed using 8-0 polyglactin sutures and ofloxacin ointment was applied. Forced duction testing was performed to check for the restriction of duction toward the operated-on muscle under general anesthesia immediately after the operation and at 8 weeks postoperatively. The distance between the myopexy and the anatomic insertion point was measured. The strength of the fixation suture was evaluated using a push pull gauge at the myoscleral union to assess the stability of the bond; finally, the histologic findings were evaluated.
Efficacy of Posterior Fixation Suture: Restricted Duction Toward the Operated-on Muscle
Forced duction testing was performed on the operated-on muscles immediately after posterior fixation suture and at 8 weeks postoperatively by an independent observer other than the surgeon, who was completely masked to the posterior fixation suture protocol. Forced duction testing was graded as follows: score 0, no restriction of duction toward the field of action; score 1, mild restriction; score 2, moderate restriction; and score 3, severe restriction.
Stability of Posterior Fixation Suture: Distance and Resistance to Separation
The distance between the myopexy and the anatomic insertion point was measured. To assess the stability of the bond, we measured the maximal tensile strength required to separate the posterior fixation suture using a push pull gauge. After enucleation, the cut ends of the superior rectus muscles were tightly sutured with 4-0 black silk and then connected to a push pull tension gauge (Teclock, Okaya, Japan). The traction was slowly increased in the perpendicular direction until the myoscleral union was broken, and the maximum tension was recorded.
Postmortem Histologic Examinations
Tissues in each of the 3 groups were examined macroscopically and microscopically using hematoxylin-eosin staining and Masson trichrome staining by a pathologist completely masked to the posterior fixation suture protocol. The degree of fibrosis, acute and chronic inflammation between the sclera and superior rectus muscles, and foreign body reactions around the implants were investigated. Severity scales were scored from 0 to 4, modified from the criteria that were previously described. Fibrosis was graded as follows: grade 0, absent; grade 1, focal loose; grade 2, diffuse loose; grade 3, focal dense; and grade 4, diffuse dense. Acute inflammation was graded as follows: grade 0, absent; grade 1, 1 focus of at least 5 polymorphonuclear leukocytes (PMNs); grade 2, more than 1 focus of grade 1 or at least 1 focus of 5 to 20 PMNs; grade 3, multiple and/or confluent foci of grade 2; and grade 4, diffuse and dense PMN infiltration with microabscess formation. Chronic inflammation was graded as follows: grade 0, absent; grade 1, 1 focus of at least 5 mononuclear inflammatory cells (lymphocytes and plasma cells); grade 2, more than 1 focus of grade 1, at least 1 focus of 5 to 20 mononuclear inflammatory cells; grade 3, multiple and/or confluent foci of grade 2; and grade 4, diffuse and dense lymphoplasmacytic infiltration with lymphoid follicle formation. Foreign body reactions were graded as follows: grade 0, absent; grade 1, focal and few multinucleated giant cells; grade 2, focal and frequent multinucleated giant cells; grade 3, diffuse and frequent multinucleated giant cells; and grade 4, diffuse and frequent multinucleated giant cells with necrosis.
Statistical Analysis
Statistical analyses were performed using Fisher’s exact test or linear-by-linear association to identify the differences among the 3 groups with respect to the forced duction testing and the histologic findings. The distance and tensile forces of the posterior fixation sutures were analyzed using one-way analysis of variance (ANOVA). For statistical analysis, forced duction testing grades were divided into low (score 0, 1) or high (score 2, 3) grades. Histologic parameters were also divided into low (grade 0, 1, and 2) or high (grade 3 and 4) grades and were compared using Fisher’s exact test. Statistical significance was accepted for P values < .05. When statistical significance was identified among the 3 groups, post hoc pairwise comparisons were carried out.
Results
Efficacy of Posterior Fixation Suture: Restricted Duction Toward the Operated-on Muscle
The results from the forced testing of the duction toward the operated-on muscles immediately and 8 weeks after the operation are shown in Figure 2 . Immediately after the operation, the grade of restricted duction was low in all of the eyes in the Conventional group and in most of the eyes in the Silicone and Marlex groups. However, the Marlex group had significantly more eyes with a high-grade restriction toward the operated-on muscles than the Conventional group ( P = .023 by Fisher’s exact test). Eight weeks after surgery, there was no significant change compared to the immediate postoperative period in all groups ( P > .999, Conventional; P = .384, Silicone; and P = .260, Marlex). Between groups, the Marlex group had significantly more eyes with high-grade restriction toward the operated-on muscles than the Conventional group ( P < .010). There was no significant difference between the Silicone group and the Conventional group immediately after the operation and at 8 weeks postoperatively ( P = .500, and P = .244, respectively). There was minimal or no restriction to the opposite side of duction in all groups at all periods examined.
Stability of Posterior Fixation Suture: Distance and Resistance to Separation
The distance of the posterior fixation was observed at the expected distance of 6 mm at both sides of the muscle in all groups without significant deviation. However, partial extrusion of the silicone sponge was found in 1 eye. Concerning the resistance to separation of the myoscleral union, most of the operated-on muscles were sufficiently adhered to the sclera. The maximum tensile strength to break the myoscleral union was 234 ± 39.5 (range, 210-340) gram force in the Conventional group, 256 ± 74.5 (range, 170-480) gram force in the Silicone group, and 321 ± 41.7 (range, 280-450) gram force in the Marlex group. There were significant differences between the 3 groups ( P < .001 by one-way ANOVA), and post hoc tests revealed that the Marlex group showed a significantly higher resistance to separation at the myoscleral union compared to the other groups ( Figure 3 ). No significant difference was observed between the Silicone group and the Conventional group.



