Purpose
To assess by Fourier-domain optical coherence tomography (FDOCT) changes produced in iridocorneal angle measurements in patients undergoing Visian Implantable Collamer Lens (ICL) V4c (STAAR Surgical AG) placement.
Design
Prospective interventional case series.
Methods
In 50 eyes of 25 myopic subjects consecutively scheduled for ICL implant, FDOCT (RTVue; Optovue Inc) iridocorneal angle measurements were made before and 1 and 3 months after surgery. Trabecular-iris angle (TIA) and angle opening distance 500 μm anterior to the scleral spur (AOD 500 ) were compared among the quadrants nasal, temporal, and inferior, and correlations with ocular variables including lens vault were examined.
Results
Preoperative TIA was 48.7 ± 8.7, 48.2 ± 8.7, and 48.7 ± 9.3 degrees for the nasal, temporal, and inferior quadrants, with no differences ( P = 1.000). Following ICL implant, corresponding values fell to 31.2 ± 11.5, 30.0 ± 10.7, and 29.7 ± 8.1 degrees at 1 month postsurgery, indicating angle narrowing of 34%–42%, and to 30.6 ± 12.3, 30.1 ± 11.9, and 29.8 ± 12.3 degrees, respectively, at 3 months postsurgery. Angle measurements failed to vary between 1 month and 3 months postsurgery ( P = .481). In 8 eyes, iridotrabecular contact attributable to surgery was observed. One month after surgery, vault measurements correlated with TIA (R = −.309; P = .048). Six variables were identified as predictors of TIA at 1 month postsurgery (R 2 = .907).
Conclusions
Although considerable angle narrowing was detected 1 month after ICL V4c implant, this narrowing remained stable at 3 months postsurgery. Factors predictive of TIA could serve to identify suitable candidates for ICL placement.
The Visian Implantable Collamer Lens (ICL; STAAR Surgical AG, Nidau, Switzerland) is a precrystalline phakic intraocular lens designed for implant in the posterior chamber to correct myopia, hyperopia, and astigmatism. Besides being safe, the technique has multiple benefits over keratorefractive procedures, such as rapid visual recovery, a stable refractive state, and better vision quality. The latest-generation ICL V4c has a central hole or AquaPORT (STAAR Surgical AG, Nidau, Switzerland) for aqueous humor flow that avoids the need for iridotomy shown by earlier models (including V4b) and possible complications such as raised intraocular pressure (IOP), hyphema, or iritis.
The new V4c model is, nevertheless, not exempt from several potential complications related to ICLs. Such complications are mostly associated with the vault distance between the posterior ICL surface and the anterior surface of the crystalline lens. Hence, when this distance is insufficient, there is an increased risk of developing cataract, while an excessive distance may induce glaucoma owing to angle closure, or pupillary block, pigment dispersion, or abnormal pupil dynamics.
Although many studies have examined modifications produced following the implant of this new ICL, including elevated IOP, cataract and endothelial abnormalities, vaulting after accommodation, or different light conditions, to date only a few investigations have addressed anterior chamber angle changes produced in response to ICL V4c placement. The first studies to assess angle width following ICL implant were based on gonioscopy examination. In one such study, Abela-Formanek and associates observed that trace pigmentation in the trabecular meshwork was common after ICL implant, though no direct impact on IOP was noted, and Chun and associates reported that the presence of an ICL narrowed the angle. However, this type of examination has several shortcomings, including its subjective nature and patient discomfort. Later, authors such as Chung and associates observed, through ultrasound biomicroscopy (UBM), angle narrowing in response to the previous ICL model V4b, which requires iridotomy. Also through UBM, Lim and associates associated the ICL V4b placement with angle narrowing in patients with a shallow anterior chamber. UBM is nevertheless invasive and time consuming, and has been superseded in terms of resolution and availability by optical coherence tomography (OCT), which allows for more detailed angle assessment. So far, the angle effects of placement of ICL V4c with its central hole in the absence of iridotomy are unknown.
The purpose of the present study was to examine the effects on iridocorneal angle measurements made by Fourier-domain OCT (FDOCT) of ICL V4c implant and to establish possible correlations between angle modifications and lens vault, IOP, or preexisting angle width. Finally, we identified factors that could be predictive of postoperative angle width.
Methods
This prospective interventional case series study examined 50 eyes of 25 patients consecutively scheduled for ICL implant from June 1, 2013 to February 28, 2015 at the practice Centro Internacional de Oftalmología Avanzada in Madrid (Spain). The study protocol adhered to the tenets of the Declaration of Helsinki and received institutional review board approval prospectively from the above center. This observational study was registered in EudraCT (number 2015-004742-25). Before the study outset, all subjects enrolled signed a consent form once the nature of the study had been explained to them in detail.
Inclusion criteria were age 20–45 years and a stable refractive state at least in the previous 2 years. Exclusion criteria were hyperopia, anterior chamber depth <2.8 mm, history of glaucoma or ocular inflammation, preexisting corneal disease, and endothelial cell count <2500 cells/mm 2 .
General Examination Protocol
Before surgery, all patients underwent a standard examination that included general medical history, measurement of visual acuity, slit-lamp anterior biomicroscopy, posterior segment ophthalmoscopy, tonometry (Canon TX 10 pneumotonometer; Canon Inc, Tokyo, Japan), endothelial cell count (Tomey), corneal topography (Pentacam, Oculus Inc, Wetzlar, Germany), biometry (IOL Master; Carl Zeiss, Meditec, Dublin, California, USA), and FDOCT (RTVue; Optovue Inc, Fremont, California, USA).
Following ICL placement, visual outcome was assessed by measuring uncorrected visual acuity (UCVA) and best-corrected visual acuity (BCVA) using the Snellen chart (logMAR scale). The Pentacam was used to measure the depth of the anterior chamber from the endothelium. Axial length, corneal diameter, and pupil diameter were measured using the IOL Master.
The following variables were recorded in the postoperative period: UCVA, BCVA, spherical error, IOP by Goldmann applanation tonometry, lens vault, endothelial cell count, and iridocorneal angle measurements by FDOCT.
Fourier-Domain Optical Coherence Tomography
The RTVue 100 instrument used has a scan speed of 26 000 A-scans per second, an 840 nm laser diode, and a 5–8 μm axial resolution. A CAM-L lens was used for examination of the anterior segment. Following our study protocol, examinations were performed on the nasal, temporal, and inferior quadrants (3, 6, and 9 o’clock) under mesopic conditions with the device’s software set to Angle mode. In this mode, a 3 × 2.3 mm area was subjected to 32 B-scans, each composed of 1024 A-scans, centered at the limbus. B-scan duration was 0.04 seconds.
Images were obtained by a trained examiner (J.I.F.V.) with the patient sitting and looking at a fixed point inside the device. Only images of a quality indicated by a signal strength intensity (SSI) greater than 30 were accepted. Each quadrant was scanned 3 times and the examiner chose the image showing the best quality and least noise.
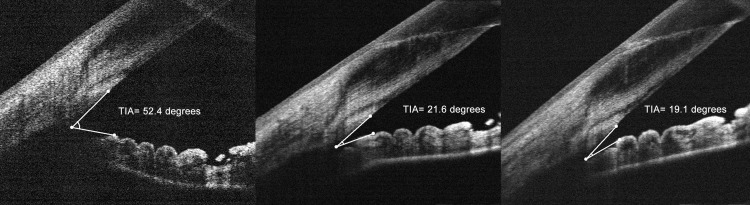
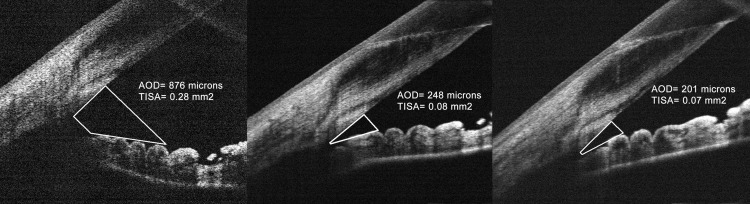
The measurements made on these images were trabecular-iris angle (TIA), angle opening distance 500 μm from the scleral spur (AOD 500 ), and trabecular-iris space area 500 μm from the scleral spur (TISA 500 ), parameters that have been described in ultrasound biomicroscopy and standardized in the last years to objectively quantify the angle. TIA was measured by tracing a line of 500 μm from the angle recess toward the Schwalbe line and another line on the surface of the iris to the point perpendicular to the first line ( Figure 1 ). AOD 500 was measured as the perpendicular distance from the trabecular meshwork 500 μm anteriorly from the scleral spur to the anterior iris surface. TISA 500 was defined as the area bounded anteriorly by the AOD, posteriorly by a line drawn from the scleral spur perpendicular to the plane of the inner scleral wall to the opposing iris, superiorly by the inner corneoscleral wall, and inferiorly by the iris surface ( Figure 2 ). The vault was also measured manually with FDOCT by tracing a line from the center of the anterior pole of the crystalline lens to the posterior pole of the ICL.
Implantable Collamer Lens Characteristics and Surgical Implant Technique
The ICL V4c is a 1-piece intraocular lens (IOL) made of collamer, a hydrophilic material composed of collagen and polyhydroxyethylmethacrylate-based copolymer. The lens is available in spherical powers ranging from −18.0 to +10.0 diopters (D) and astigmatic corrections of 1.0–6.0 D. Lens size was defined in this study using the manufacturer calculator software according to the horizontal white-to-white distance (WTW) obtained using the IOL Master (Carl Zeiss Meditec, Jena, Germany).
The IOLs implanted were 26 spherical and 24 toric ICL V4c with a central AquaPORT, all in myopic patients. Spherical and toric lenses had the same characteristics. They were all aligned with the 180 degree meridian and rotated a maximum of 5–10 degrees.
All operations were performed by the same surgeon (A.M.M.) at the Centro Internacional de Oftalmología Avanzada in Madrid (Spain). The surgical technique consists of a corneal paracentesis and instillation of intracamerular lidocaine 1%. The anterior chamber is filled with a hydroxypropyl methylcellulose solution as viscoelastic (OcuCoat; Bausch & Lomb, Rochester, New York, USA). A 3.2 mm clear corneal incision is made through which the ICL is inserted with an injector (STAAR Surgical Co). With the help of a hook, the lens is correctly positioned. After elimination of remnants of viscoelastic with saline, 1 mg of cefuroxime sodium is injected and incisions are hydrated to complete the surgical procedure. Postoperative treatment consists of 4 drops per day of moxifloxacin for 7 days and tobramycin and dexamethasone 0.1% 4 times daily tapered over 30 days.
Statistical Analysis
All statistical tests were performed using the software package SPSS (Statistical Package for the Social Sciences, v18.0; SPSS Inc, Chicago, Illinois). Quantitative data are provided as their means and standard deviations, while qualitative data are expressed as frequency distributions. The Kolmogorov-Smirnov test was used to check the normality of the measurements made. Univariate correlations were identified using the Pearson correlation test, or Spearman Rho in the case of non-normally distributed data (spherical error; angle opening distance 500 μm from the scleral spur, and trabecular-iris space area 500 μm from the scleral spur). The measurements from both eyes of the subjects were analyzed, performing an appropriate test taking the correlation of both eyes into account and not calculating them as independent. The analysis was adjusted for the cluster patient, using Stata software, version 12.0 (2011) (Stata Corp, College Station, Texas, USA). Differences between preoperative quadrants were assessed using analysis of variance (ANOVA) with Bonferroni adjustment, whereas differences between 1 and 3 months postoperative were assessed using paired t test. The sample size was calculated observing that at least 24 eyes had to be studied for TIA measurements to detect a 30% (15 degrees approximately) difference between preoperative and postoperative measurements with alpha of 0.05 and beta of 0.10. A multivariate linear stepwise regression model was used to assess which preoperative factors could be used to predict postoperative TIA by calculating R 2 . Significance was set at P < .05.
Results
The study’s inclusion criteria were fulfilled by 50 eyes of 25 patients of mean age 29.96 ± 5.9 (range 21–44) years; 64% of patients (n = 16) were women. The lenses implanted were 26 spherical and 24 toric ICL V4c, and the minimum follow-up time was 3 months. The implanted ICL showed a mean size of 13.2 ± 0.24 (range 12.6–13.7) mm, mean spherical power of −11.26 ±3.37 (range −18 to −3.5) diopters, and mean cylinder of 1.5 ± 1.49 (range 0–5). Before surgery, anterior chamber depth (ACD) was 3.26 ± 0.26 (range 2.95–3.97) mm, axial length was 26.64 ± 2.08 (range 23.66–31.53) mm, and WTW distance was 12.02 ± 0.33 (11.4–12.7) mm. The remaining baseline characteristics of the study population are provided in Table 1 .
| Variable | Preoperative | 1 Month Postoperative | 3 Months Postoperative | |||
|---|---|---|---|---|---|---|
| Mean ± SD | Range | Mean ± SD | Range | Mean ± SD | Range | |
| Spherical error (D) | −8.66 ± 4.26 | −21, −2.25 | 0.625 | 0.25, 1 | 0.91 ± 0.37 | 0.5, 1.5 |
| Cylindrical error (D) | −1.47 ± 1.18 | −5, 0 | −1.13 ± 0.5 | −2.25, −0.25 | −1.54 ± 0.29 | −1.75, −1 |
| Spherical equivalent (D) | −9.40 ± 4.14 | −22.00, −2 | −0.04 ± 0.2 | −0.625, 0.625 | 0.01 ± 0.15 | −0.375, 0.75 |
| UCVA (logMAR) | 1.48 ± 0.29 | 1, 2 | 0.06 ± 0.10 | 0.0, 0.4 | 0.05 ± 0.11 | 0.0, 0.4 |
| BCVA (logMAR) | 0.07 ± 0.12 | 0.0, 0.4 | 0.04 ± 0.11 | 0.0, 0.3 | 0.04 ± 0.10 | 0.0, 0.2 |
| ECC (cells/mm 2 ) | 2795.7 ± 177.3 | 2515, 3268 | 2645.7 ± 236.1 | 2063, 3084 | 2606.5 ± 236.8 | 2012, 3009 |
| IOP (mm Hg) | 16.6 ± 3.08 | 10, 21 | 16.91 ± 3.93 | 9, 24 | 16.08 ± 2.87 | 10, 25 |
| Lens vault (μm) | Not applicable | 584.5 ± 241.0 | 188, 1210 | 526.8 ± 257.6 | 80, 1150 | |
In all patients, preoperative TIA values were over 20 degrees, whereas following surgery 12 eyes (24%) had a TIA of less than 20 degrees.
Preoperative TIA was 48.7 ± 8.7, 48.2 ± 8.7, and 48.7 ± 9.3 degrees for the nasal temporal and inferior quadrants, with no differences detected among quadrants ( P = 1.000, ANOVA). Following ICL implant, corresponding values fell to 31.2 ± 11.5, 30.0 ± 10.8, and 29.7 ± 8.1 degrees at 1 month postsurgery, and to 30.6 ± 12.3, 30.1 ± 11.9, and 29.8 ± 12.3 degrees at 3 months postsurgery. No differences in angle measurements were detected between 1 month and 3 months postsurgery ( P = .481, paired t test). This indicates that the mean narrowing in TIA produced both 1 month and 3 months after ICL implant was around 34.5%–42% ( Table 2 ).
| Parameter | Preoperative | 1 Month Postoperative | 3 Months Postoperative | |||
|---|---|---|---|---|---|---|
| Mean ± SD | 95% CI | Mean ± SD | 95% CI | Mean ± SD | 95% CI | |
| TIA nasal (degrees) | 48.7 ± 8.7 | 46.2–51.2 | 31.2 ± 11.5 | 27.8–34.7 | 30.6 ± 12.3 | 26.8–34.4 |
| TIA temporal (degrees) | 48.2 ± 8.7 | 45.8–50.8 | 30.0 ± 10.8 | 26.8–33.2 | 30.1 ± 11.9 | 26.4–33.8 |
| TIA inferior (degrees) | 48.7 ± 9.3 | 46.1–51.1 | 29.7 ± 8.1 | 26.6–32.8 | 29.8 ± 12.3 | 26.0–33.6 |
| AOD 500 nasal (μm) | 765.8 ± 223.8 | 702.2–829.4 | 384.4 ± 167.5 | 334.6–434.1 | 380.5 ± 171.8 | 327.0–432.9 |
| AOD 500 temporal (μm) | 804.6 ± 276.8 | 725.9–883.3 | 369.4 ± 169.9 | 318.8–419.8 | 363.8 ± 167.1 | 311.4–416.2 |
| AOD 500 inferior (μm) | 789 ± 226.6 | 725.3–852.7 | 385.9 ± 158.3 | 336.6–435.2 | 389.2 ± 182.8 | 334.5–443.9 |
| TISA 500 nasal (mm 2 ) | 0.26 ± 0.09 | 0.23–0.28 | 0.13 ± 0.07 | 0.11–0.15 | 0.13 ± 0.06 | 0.11–0.15 |
| TISA 500 temporal (mm 2 ) | 0.27 ± 0.11 | 0.24–0.30 | 0.13 ± 0.06 | 0.11–0.15 | 0.12 ± 0.06 | 0.10–0.14 |
| TISA 500 inferior (mm 2 ) | 0.26 ± 0.09 | 0.23–0.29 | 0.14 ± 0.07 | 0.12–0.16 | 0.14 ± 0.07 | 0.12–0.16 |
Preoperative angle opening distance 500 μm from the scleral spur (AOD 500 ) was 765.8 ± 223.8, 804.6 ± 276.8, and 789.0 ± 228.6 μm for the nasal, temporal, and inferior quadrants, respectively, while corresponding values recorded 1 month and 3 months after surgery were 384.4 ± 167.5, 369.4 ± 169.9, and 385.9 ± 158.3 μm; and 380.5 ± 171.8, 363.8 ± 167.1, and 389.2 ± 182.8 μm, respectively.
Preoperative trabecular-iris space area 500 μm from the scleral spur (TISA 500 ) was 0.26 ± 0.09, 0.27 ± 0.11, and 0.26 ± 0.09 mm 2 for the nasal, temporal, and inferior quadrants, respectively, while corresponding values recorded 1 month and 3 months after surgery were 0.13 ± 0.07, 0.13 ± 0.06, and 0.14 ± 0.07 mm 2 and 0.13 ± 0.06, 0.12 ± 0.06, and 0.14 ± 0.07 mm 2 , respectively.
According to the type of lens implanted, spherical and toric ICL, the degree of decrease of angle measurements was very similar between both groups, with no differences ( P = .215, t test).
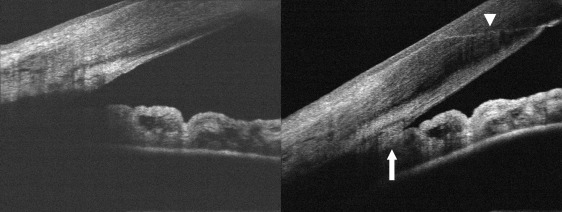
In 8 eyes of 6 patients (8/50; 16%), iridotrabecular contact that was absent before surgery was observed ( Figure 3 ). Preoperatively, trabecular-iris angles in these patients varied widely (from 27 to 56 degrees).
In a multivariate linear regression model designed to identify the main preoperative factors affecting angle width attributable to ICL implant, the following variables were included: preoperative TIA, age, sex, spherical error, ACD, axial length, WTW, and lOL power and size. After the model excluded lens power and size and the sex, the 6 remaining variables showed an adjusted R 2 = 0.907 for the nasal, R 2 = 0.863 for the temporal, and R 2 = 0.849 for the inferior quadrant ( P = .000). At 3 months postoperative TIA showed an adjusted R 2 = 0.815 for the nasal, R 2 = 0.802 for the temporal, and R 2 = 0.789 for the inferior quadrant, respectively.
The following equation was able to explain 90.7% of the variation in 1 month postoperative angle width: One month postoperative nasal trabecular-iris angle = 36.961 + preoperative trabecular-iris angle × 0.786 − 1.044 × age + 4.371 × spherical error − 19.817 × ACD + 9.432 × axial length − 13.305 × white-to-white distance ( Table 3 ). And 3 months postoperative nasal trabecular-iris angle = 34.245 + preoperative trabecular-iris angle × 0.722 − 1.217 × age + 5.219 × spherical error − 18.006 × ACD + 10.114 × axial length − 13.810 × white-to-white distance. Accordingly, the 2 most predictive factors, in the multivariate model for TIA at 1 and at 3 months, were ACD followed by WTW or corneal diameter.
| Variable | B | 95% CI | P Value a |
|---|---|---|---|
| Constant | 36.961 | −45.145, 119.067 | .335 |
| TIA preoperative (degrees) | 0.786 | 0,093, 1.478 | .030 |
| Age (y) | −1.044 | −1.405, −0.683 | .000 |
| Spherical error (diopters) | 4.371 | 2.444, 6.298 | .001 |
| ACD (mm) | −19.817 | −30.573, −9,062 | .002 |
| Axial length (mm) | 9.432 | 4.955, 13.909 | .001 |
| White-to-white distance (mm) | −13.305 | −23.991, −2.620 | .020 |
a Multivariate linear stepwise regression model used to determine the factors that affect postoperative trabecular-iris angle.
Lens vault fell significantly from the 584.5 ± 241.0 (range 188–1270) μm recorded at 1 month postsurgery to 526.8 ± 257.6 (range 80–1150) μm at 3 months postsurgery ( P = .000, t test). Correlations with this variable were observed for 1 month postoperative TIA of R = −0.309 ( P = .048) for the nasal quadrant, R = −0.397 ( P = .007) for the temporal quadrant, and R = −0.300 ( P = .046) for the inferior quadrant. Similar correlations were detected for angle opening distance 500 μm from the scleral spur and trabecular-iris space area 500 μm from the scleral spur (see Table 4 ). However, correlations between vault and 3 months postoperative TIA measurements were weaker: R = −0.176; R = −0.198, and R = −0.222 for the 3 quadrants, respectively ( P = .288). Nine eyes (18%) showed a vault larger than 750 μm at 3 months postsurgery with TIA varying widely from 8 to 41 degrees. In this subgroup, lens vault did not show statistically significant correlation with preoperative TIA in any of the 3 quadrants examined (R < 0.39; P = .791).



