Purpose
To evaluate the effect of scan quality on the diagnostic accuracies of optic nerve head (ONH), retinal nerve fiber layer (RNFL), and ganglion cell complex (GCC) parameters of spectral-domain optical coherence tomography (SD OCT) in glaucoma.
Design
Cross-sectional study.
Methods
Two hundred fifty-two eyes of 183 control subjects (mean deviation [MD]: −1.84 dB) and 207 eyes of 159 glaucoma patients (MD: −7.31 dB) underwent ONH, RNFL, and GCC scanning with SD OCT. Scan quality of SD OCT images was based on signal strength index (SSI) values. Influence of SSI on diagnostic accuracy of SD OCT was evaluated by receiver operating characteristic (ROC) regression.
Results
Diagnostic accuracies of all SD OCT parameters were better when the SSI values were higher. This effect was statistically significant ( P < .05) for ONH and RNFL but not for GCC parameters. In mild glaucoma (MD of −5 dB), area under ROC curve (AUC) for rim area, average RNFL thickness, and average GCC thickness parameters improved from 0.651, 0.678, and 0.726, respectively, at an SSI value of 30 to 0.873, 0.962, and 0.886, respectively, at an SSI of 70. AUCs of the same parameters in advanced glaucoma (MD of −15 dB) improved from 0.747, 0.890, and 0.873, respectively, at an SSI value of 30 to 0.922, 0.994, and 0.959, respectively, at an SSI of 70.
Conclusion
Diagnostic accuracies of SD OCT parameters in glaucoma were significantly influenced by the scan quality even when the SSI values were within the manufacturer-recommended limits. These results should be considered while interpreting the SD OCT scans for glaucoma.
Spectral-domain optical coherence tomography (SD OCT) is a recent technique that enables imaging the ocular structures with higher resolution and faster scan rate compared to the previous version of this technology (Stratus OCT; Carl Zeiss Meditec, Inc, Dublin, California, USA). Several studies have reported good diagnostic ability of SD OCT in glaucoma. Two factors that are known to influence the diagnostic ability of SD OCT in glaucoma are severity of disease and size of the optic disc. Diagnostic accuracy of SD OCT parameters is shown to be significantly better in eyes with more severe damage. Sensitivity of optic nerve head (ONH) parameters of SD OCT are shown to be greater in large optic discs compared to small discs.
In addition to the above 2 factors, another factor that has been found to affect the parameter measurements of OCT is the quality of scan. Various studies with Stratus OCT have found a significant effect of scan quality on ONH, retinal nerve fiber layer (RNFL), and macular measurements. Kim and associates have also reported a significant effect of scan quality on the RNFL measurements of SD OCT. Evaluating the influence of scan quality on the diagnostic ability of imaging devices in glaucoma, Sung and associates found that the scan quality affected the diagnostic performance of the RNFL parameters of Stratus OCT. In a study on normal subjects of Indian origin with SD OCT, Rao and associates found that signal strength of the scan, a measure of scan quality, affected the measurements of ONH but not the RNFL or ganglion cell complex (GCC) parameters; ONH rim measurements increased and cup measurements decreased with increasing signal strengths. However, the effect of scan quality on the diagnostic ability of SD OCT in glaucoma has not been evaluated.
The aim of this study was to evaluate the effect of scan quality on the diagnostic performance of ONH, RNFL, and GCC parameters of SD OCT in glaucoma.
Methods
This was an observational, cross-sectional study of consecutive subjects referred by general ophthalmologists to a tertiary eye care facility between September 2010 and November 2012 for a glaucoma evaluation. Informed consent was obtained from all subjects to participate in the study and the Institutional Review Board of L. V. Prasad Eye Institute approved the methodology. All methods adhered to the tenets of the Declaration of Helsinki for research involving human subjects.
Inclusion criteria were age ≥18 years, best-corrected visual acuity of 20/40 or better, and refractive error within ±5 diopters (D) sphere and ±3 D cylinder. Exclusion criteria were presence of any media opacities that prevented good-quality optic disc photographs and SD OCT imaging and any retinal (including macular) disease other than glaucoma that could confound the evaluations. All participants underwent a comprehensive ocular examination, which included a detailed medical history, best-corrected visual acuity measurement, slit-lamp biomicroscopy, Goldmann applanation tonometry, gonioscopy, dilated fundus examination, standard automated perimetry (SAP), digital optic disc photography, and SD OCT imaging with RTVue (Optovue Inc, Fremont, California, USA).
SAP was performed using a Humphrey Field analyzer, model 750 (Zeiss Humphrey Systems, Dublin, California, USA), with the Swedish interactive threshold algorithm (SITA) standard 24-2 algorithm. Visual fields (VF) with fixation losses and false-positive and false-negative response rates of less than 20% were considered reliable. VFs were considered glaucomatous if the pattern standard deviation had a P value of less than .05 and the glaucoma hemifield test result was outside normal limits.
Digital optic disc photographs were obtained by trained technicians (Visupac 4.2.2; Carl Zeiss Meditec Systems GmbH, Pirmasens, Germany). Photographs consisted of a 50-degree image centered on the optic disc, a similar image centered on the macula, a 30-degree image centered on the optic disc, and a 20-degree image centered on the disc. All these images also consisted of 1 colored and 1 red-free image each. Each photograph was evaluated by 2 of the 4 experts (H.L.R., S.S., N.S.C., and C.S.G.) independently, who were masked to the clinical examination results of the subjects and also the results of visual field and imaging examinations. Experts classified the optic disc photographs into glaucomatous and nonglaucomatous based on the presence of focal or diffuse neuroretinal rim thinning, localized notching, or nerve fiber layer defects. Discrepancies between the 2 experts were resolved by consensus. Eyes in which a consensus could not be reached were excluded from analysis. Eyes in which a classification to either glaucoma or control group was not possible by both the experts (true disc suspects) were also excluded from the analysis.
SD OCT examination was performed with the RTVue (software version 5.1.0.90). RTVue uses a scanning laser diode with a wavelength of 840 ± 10 nm to provide images of ocular microstructures. The protocols used for imaging with RTVue in this study were ONH (optic nerve head) and GCC (ganglion cell complex). These protocols have been explained earlier. All patients had both SD OCT protocols as well as the VF testing performed on the same day.
Scan quality of the SD OCT image on RTVue was based on the signal strength index (SSI). SSI is a proprietary measure of the average signal strength across the scan. The SSI can range from 0 (no signal) to 100 (very strong signal). The stronger the OCT signal, the higher the SSI. As per the manufacturers’ guidelines, all scans with an SSI score of <30 were excluded from the analysis. Eyes in which the segmentation algorithm failed were also excluded.
Optic Nerve Head Scan
The ONH protocol consists of 12 radial scans 3.4 mm in length and 6 concentric ring scans ranging from 2.5-4.0 mm in diameter, all centered on the optic disc. ONH protocol calculates various parameters that describe the ONH and also generates a polar RNFL thickness map, which is the RNFL thickness measured along a circle 3.45 mm in diameter centered on the optic disc.
Ganglion Cell Complex Scan
The GCC scan is designed to automatically measure the inner retinal thickness, which includes the nerve fiber layer, ganglion cell layer, and the inner plexiform layer, collectively called the GCC. The parameters generated by the GCC analysis are the average, superior, and inferior GCC thickness; average superior minus inferior GCC thickness; and superior minus inferior thickness standard deviation. In addition to the above parameters, the GCC protocol provides 3 other parameters called GLV (global loss volume), FLV (focal loss volume), and RMS (root mean square). These have been explained previously.
Statistical Analysis
Descriptive statistics included mean deviation (MD) and standard deviation for normally distributed variables and median and interquartile range (IQR) for non-normally distributed variables.
Receiver operating characteristic (ROC) regression modeling technique was used to evaluate the influence of SSI on the diagnostic abilities of the ONH, RNFL, and GCC parameters in glaucoma. This modeling approach was initially described by Medeiros and associates for evaluation of the influence of covariates on the performance of diagnostic tests in glaucoma. This methodology allows the evaluation of the influence of covariates on the diagnostic performance of the test, so that ROC curves for specific values of the covariate of interest can be obtained. Also, it allows adjustment for the possible confounding effects of other covariates (disease severity and optic disc size in this case). Details of the modeling procedure have been described previously. The model was adjusted for the differences in optic disc size and SSI values between the control group and glaucoma group. Parameters were estimated using probit regression. To obtain confidence intervals (CI) for regression parameters, a bootstrap resampling procedure was used (n = 1000 resamples). As measurements from both eyes of the same subject are likely to be correlated, the standard statistical methods for parameter estimation lead to underestimation of standard errors. Therefore, the cluster of data for the study subject was considered as the unit of resampling when calculating standard errors. Statistical analyses were performed using commercial software (Stata ver. 11.2; StataCorp, College Station, Texas, USA).
Results
Six hundred and seventy eight eyes of 382 consecutive subjects referred for glaucoma evaluation to our center were analyzed. Forty-two eyes with unreliable VFs and 7 eyes with poor-quality disc photographs were excluded. Further, 12 eyes with segmentation algorithm failure on SD OCT, 7 eyes with SSI <30 on ONH scans, 3 eyes with SSI <30 on GCC scans, and 3 eyes with SSI <30 both on ONH and GCC scans were excluded. Of the remaining, 145 eyes in which the masked optic disc classification on photographs did not correlate with the VF classification were excluded, leaving behind 459 eyes for the analysis. Of these, 207 eyes with the optic disc and VF classification as “glaucoma” formed the glaucoma group and 252 eyes with optic disc and VF classification as “nonglaucoma” formed the control group. Table 1 shows the demographic, visual field, and SD OCT parameters of the 2 groups. All VF and SD OCT parameters were significantly different in the glaucoma compared to the control group. Glaucoma patients had significantly smaller optic discs than the control subjects. SSI values were statistically significantly higher in the control compared to glaucomatous group, though the difference was actually small. SSI values of GCC scans were significantly higher than those of ONH scans ( P < .001). SSI values of both ONH and GCC scans were statistically significantly associated with age of the subject and severity of glaucoma, with SSI scores being lower in older-aged subjects and eyes with more severe damage; the associations, however, were weak (coefficient of determination, R 2 < 0.05 for all associations).
| Control Group (n = 252 Eyes of 183 Subjects) | Glaucoma Group (n = 207 Eyes of 159 Patients) | P Value | |
|---|---|---|---|
| Age (y) | 54 (45, 62) | 55 (48, 63) | .34 |
| Disc area (mm 2 ) | 2.21 (1.84, 2.56) | 1.95 (1.61, 2.34) | <.001 |
| Mean deviation (dB) | −1.84 (−3.08, −0.70) | −7.31 (−14.60, −4.65) | <.001 |
| Pattern standard deviation (dB) | 1.68 (1.47, 1.98) | 7.62 (3.80, 10.35) | <.001 |
| Visual field index (%) | 99 (98, 99) | 82 (63, 92) | <.001 |
| Optic nerve head parameters | |||
| Signal strength index | 51 (45, 59) | 48 (41, 55) | .003 |
| Cup area (mm 2 ) | 1.37 (0.97, 1.84) | 1.59 (1.26, 1.98) | <.001 |
| Rim area (mm 2 ) | 0.81 (0.51, 1.08) | 0.27 (0.12, 0.53) | <.001 |
| Temporal rim area (mm 2 ) | 0.07 (0.03, 0.15) | 0.03 (0.01, 0.09) | <.001 |
| Superior rim area (mm 2 ) | 0.26 (0.18, 0.35) | 0.11 (0.03, 0.20) | <.001 |
| Nasal rim area (mm 2 ) | 0.25 (0.12, 0.35) | 0.05 (0.02, 0.15) | <.001 |
| Inferior rim area (mm 2 ) | 0.19 (0.11, 0.29) | 0.03 (0.01, 0.09) | <.001 |
| Rim volume (mm 3 ) | 0.06 (0.03, 0.10) | 0.01 (0.00, 0.03) | <.001 |
| Cup volume (mm 3 ) | 0.40 (0.20, 0.66) | 0.54 (0.33, 0.82) | <.001 |
| Cup-disc area ratio | 0.64 (0.48, 0.78) | 0.87 (0.73, 0.94) | <.001 |
| Horizontal cup-disc ratio | 0.89 (0.76, 0.97) | 0.98 (0.93, 1.00) | <.001 |
| Vertical cup-disc ratio | 0.80 (0.71, 0.89) | 0.96 (0.89, 0.99) | <.001 |
| Retinal nerve fiber layer parameters | |||
| Temporal quadrant (μm) | 77.0 (70.3, 84.6) | 63.2 (54.3, 72.2) | <.001 |
| Superior quadrant (μm) | 123.9 (111.8, 135.6) | 91.3 (80.8, 107.9) | <.001 |
| Nasal quadrant (μm) | 80.5 (71.8, 88.5) | 65.9 (55.3, 74.9) | <.001 |
| Inferior quadrant (μm) | 129.3 (115.4, 141.7) | 89.5 (81.3, 101.8) | <.001 |
| Average thickness (μm) | 103.5 (94.6, 109.9) | 78.2 (70.6, 87.5) | <.001 |
| Ganglion cell complex parameters | |||
| Signal strength index | 61 (54, 69) | 59 (51, 67) | .01 |
| Average (μm) | 93.5 (88.6, 98.9) | 76.9 (70.4, 84.4) | <.001 |
| Superior (μm) | 94.1 (88.7, 98.4) | 80.1 (71.2, 88.5) | <.001 |
| Inferior (μm) | 93.7 (88.3, 99.4) | 73.9 (67.1, 82.8) | <.001 |
| GCC FLV (%) | 1.2 (0.3, 2.5) | 6.7 (4.0, 9.7) | <.001 |
| GCC GLV (%) | 5.8 (2.7, 10.0) | 21.9 (14.4, 27.9) | <.001 |
| GCC RMS | 0.1 (0.1, 0.1) | 0.2 (0.1, 0.2) | <.001 |
Table 2 shows the estimates of the coefficients of the ROC regression model for the ONH rim area. The results indicated that the diagnostic performance of rim area increased as the MD decreased (ie, disease severity increased), as evidenced by the statistically significant negative coefficient associated with disease severity (−0.04; P = .002). The significant positive coefficient associated with SSI (0.03; P = .03) indicated that the diagnostic performance of rim area increased as the SSI increased. The top row of Figure 1 shows the ROC curves and AUCs of rim area calculated at arbitrary SSI values of 30, 50, and 70 according to the ROC regression model separately at MD levels of −5 (Top row, left), −10 (Top row, center), and −15 dB (Top row, right), indicating mild, moderate, and severe glaucomatous damage, respectively.
| Parameter | Optic Nerve Head Rim Area | Average RNFL Thickness | Average GCC Thickness | |||
|---|---|---|---|---|---|---|
| Coefficient (95% CI) | P Value | Coefficient (SE) | P Value | Coefficient (SE) | P Value | |
| Intercept | −0.48 (−1.88, 0.94) | .50 | −1.16 (−2.49, 0.15) | .08 | −0.14 (−1.65, 1.64) | .86 |
| MD | −0.04 (−0.06, −0.02) | .002 | −0.10 (−0.15, −0.06) | <.001 | −0.06 (−0.11, −0.03) | .002 |
| SSI | 0.03 (0.00, 0.06) | .03 | 0.04 (0.02, 0.07) | .001 | 0.02 (−0.01, 0.04) | .18 |
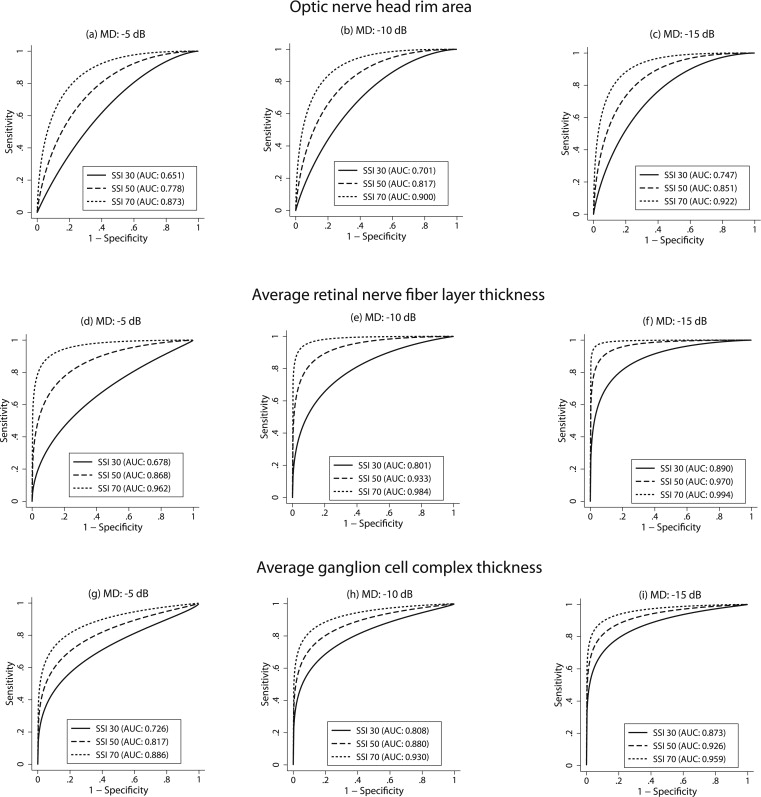
Table 2 also shows the estimates of the coefficients of the ROC regression model for the average RNFL thickness parameter. The results indicated that the diagnostic performance of average RNFL thickness increased as the MD decreased, as evidenced by the statistically significant negative coefficient associated with disease severity (−0.10; P < .001). The significant coefficient associated with SSI (0.04; P = .001) indicated that the diagnostic performance of average RNFL thickness increased as the SSI increased. The middle row of Figure 1 shows the ROC curves and AUCs of RNFL thickness calculated at arbitrary SSI values of 30, 50, and 70 according to the ROC regression model separately at MD levels of −5 (Middle row, left), −10 (Middle row, center), and −15 dB (Middle row, right).
Table 2 also shows the estimates of the coefficients of the ROC regression model for the average GCC thickness parameter. The results of the model showed a significant influence of disease severity on the diagnostic accuracy of average GCC thickness. The effect size of the SSI on the diagnostic performance of average GCC thickness (0.02; P = .18) was, however, smaller than that on the diagnostic performance of ONH (by 33%) and RNFL (by 50%) parameters. The bottom row of Figure 1 shows the ROC curves and AUCs of average GCC thickness calculated at arbitrary SSI values of 30, 50, and 70 according to the ROC regression model separately at MD levels of −5 (Bottom row, left), −10 (Bottom row, center), and −15 dB (Bottom row, right).
Table 3 shows similar analysis for the inferior quadrant ONH rim area, RNFL, and GCC thickness parameters. Table 4 shows similar analysis for the superior quadrant ONH rim area, RNFL, and GCC thickness parameters. These results regarding the effect of SSI on the AUCs of the regional SD OCT parameters were essentially similar to the effect of SSI on the AUCs of the global parameters.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


