Purpose
To use micro–ribonucleic acid (microRNA) profiles in the vitreous for differential diagnosis of primary vitreoretinal lymphoma and uveitis.
Design
Prospective cross-sectional study.
Methods
This prospective cross-sectional study included 17 diffuse large B-cell primary vitreoretinal lymphoma and 12 uveitis patients. The supernatant of ocular fluid was subjected to total RNA extraction, followed by complementary deoxyribonucleic acid (cDNA) synthesis. Selected samples (primary vitreoretinal lymphoma, n = 3; uveitis, n = 3) were arrayed by a real-time polymerase chain reaction (RT-PCR)-based microRNA panel that detects 168 human mature microRNAs. The markers promising in distinct levels between uveitis and lymphoma were further tested for in all the other 23 samples by individual RT-PCR analysis.
Results
Of 168 microRNAs in the array, 66.5% were detectable with consistent higher microRNA-484, microRNA-197, and microRNA-132 in the primary vitreoretinal lymphoma vitreous and higher microRNA-155, microRNA-200c, and microRNA-22* in the uveitic ocular fluids. The results were normalized by different combinations of 7 control microRNAs (microRNA-103, microRNA-191, microRNA-42-5p, microRNA-16, microRNA-425, microRNA-93, and microRNA-451). After optimization, normalization against microRNA-16 was equally as reliable as the average of the 7 control microRNAs. Individual assays of all samples supported the pattern yielded from the array analysis. But only microRNA-155 was significantly higher in the uveitic vitreous compared to that with lymphoma.
Conclusions
Mature microRNAs are detectable in ocular fluid samples. Primary vitreoretinal B-cell lymphoma and uveitis might be characterized by distinct microRNA signatures. Quantification of ocular microRNA-155 might be helpful in the differential diagnosis of these 2 diseases.
Primary vitreoretinal lymphoma, also known as primary intraocular lymphoma, is a subset of primary central nervous system lymphoma and is mostly classified as a diffuse large B-cell lymphoma. Primary vitreoretinal lymphoma affects the retina, vitreous, and optic nerve head, with the most common symptoms being blurred or decreased vision attributable to tumor cells in the vitreous and retina. In general, primary vitreoretinal lymphoma cells first emerge between the retinal pigment epithelium (RPE) and Bruch membrane, followed by infiltration in the neuroretina, optic nerve head, and vitreous. Primary vitreoretinal lymphoma is a fatal ocular malignancy owing to its frequent involvement with the brain; thus, it is important to have the diagnosis early and treat it promptly. However, the clinical appearances of primary vitreoretinal lymphoma can be quite similar to uveitis, leading to a misdiagnosis of a uveitic entity and initial treatment with anti-inflammatory agents such as corticosteroids, which can further confound the diagnosis. The ratio of interleukin-10 (IL-10) to interleukin-6 (IL-6) or interferon (IFN)-gamma in the vitreous has been used for assisting differential diagnosis because B-cell primary vitreoretinal lymphomas secrete high levels of IL-10, whereas uveitis leads to high IL-6 and IFN-gamma levels.
Micro–ribonucleic acids, also known as microRNAs, are small noncoding RNA molecules that play a key regulatory role in many biological processes. MicroRNAs belong to a highly conserved class of 17-25 nucleotide RNA molecules, which have multiple roles in negative regulation of gene expression including transcript degradation, transcript sequestering, and translational suppression, as well as possible involvement in positive regulation of gene expression via transcriptional and translational activation. The microRNA expression is deregulated in cancer through multiple mechanisms, such as gene amplification, deletion, mutation, and epigenetic silencing. There is now ample evidence that microRNAs are involved in the initiation and progression of cancer. MicroRNAs are stably present within microvesicles (exosomes) in many biofluids, including serum, plasma, urine, cerebrospinal fluid, aqueous humor, and vitreous. The extracellular microRNAs can be isolated even after long-term storage. Recently, studies have reported the high relative stability of microRNAs in biofluids and the correlation of microRNA expression profiles with diseases and disease states. A technique breakthrough for detecting short microRNAs by stem-loop quantitative real-time polymerase chain reaction (RT-PCR) has sparked tremendous interest in using microRNAs from biofluids as biomarkers for many diseases. In this study, we used quantitative RT-PCR to determine the microRNA profiles in the vitreous samples from primary vitreoretinal lymphoma and uveitis patients.
Methods
Study Subjects
This prospective cross-sectional study followed the tenets of the Declaration of Helsinki and was approved by the Institutional Review Board of National Eye Institute (NEI), National Institutes of Health (NIH). All participants signed the informed consent forms. Demographic and clinical features of study participants are listed in Table 1 . The study included 17 primary vitreoretinal B-cell lymphoma and 12 uveitis patients. The diagnosis of primary vitreoretinal lymphoma was based on the definitive identification of malignant lymphoid cells in the eye. The uveitis patients were diagnosed as having mostly noninfectious uveitis (only 1 case with Propionibacterium acnes endophthalmitis), posterior uveitis, or panuveitis. Vitreous specimens from all lymphoma patients and 9 uveitis patients were obtained through a standard 3-port pars plana vitrectomy and centrifuged (200 g , 10 minutes, room temperature) to collect supernatant. Three aqueous specimens were obtained from aseptic aqueous aspiration. The supernatant was aliquoted for quantification of cytokines, including IL-10 and IL-6, by enzyme-linked immunosorbent assay (ELISA), and for ribonucleic acid (RNA) extraction.
| Patient No. | Age | Sex | Disease | Comments |
|---|---|---|---|---|
| 1 a | 80 | F | B-cell primary vitreoretinal lymphoma | IgH gene arrangement identified |
| 2 | 67 | M | B-cell primary vitreoretinal lymphoma | IgH gene arrangement identified |
| 3 | 73 | F | B-cell primary vitreoretinal lymphoma | IgH gene arrangement identified |
| 4 a | 76 | M | B-cell primary vitreoretinal lymphoma | IgH gene arrangement identified |
| 5 | 74 | F | B-cell primary vitreoretinal lymphoma | IgH gene arrangement identified |
| 6 | 64 | F | B-cell primary vitreoretinal lymphoma | IgH gene arrangement identified |
| 7 | 69 | M | B-cell primary vitreoretinal lymphoma | IgH gene arrangement identified |
| 8 | 55 | M | B-cell primary vitreoretinal lymphoma | IgH gene arrangement identified |
| 9 | 66 | F | B-cell primary vitreoretinal lymphoma | IgH gene arrangement identified |
| 10 | 63 | F | B-cell primary vitreoretinal lymphoma | IgH gene arrangement identified |
| 11 | 58 | M | B-cell primary vitreoretinal lymphoma | IgH gene arrangement identified |
| 12 | 74 | F | B-cell primary vitreoretinal lymphoma | IgH gene arrangement identified |
| 13 | 70 | M | B-cell primary vitreoretinal lymphoma | IgH gene arrangement identified |
| 14 | 45 | F | B-cell primary vitreoretinal lymphoma | IgH gene arrangement identified |
| 15 | 50 | F | B-cell primary vitreoretinal lymphoma | IgH gene arrangement identified |
| 16 | 80 | F | B-cell primary vitreoretinal lymphoma | IgH gene arrangement identified |
| 17 a | 68 | M | B-cell primary vitreoretinal lymphoma | IgH gene arrangement identified |
| 18 a | 35 | F | Uveitis | Vitreous inflammation granulomatous |
| 19 | 72 | F | Uveitis | Vitreous subacute inflammation |
| 20 | 72 | F | Uveitis | Vitreous chronic inflammation |
| 21 | 60 | F | Uveitis | Aqueous inflammation |
| 22 | 45 | F | Uveitis | Aqueous chronic inflammation |
| 23 | 52 | F | Uveitis | Vitreous infection ( Propionibacterium acnes ) |
| 24 | 69 | F | Uveitis | Vitreous choroid chronic inflammation |
| 25 | 79 | F | Uveitis | Vitreous inflammation granulomatous |
| 26 | 24 | M | Uveitis | Vitreous inflammation granulomatous |
| 27 a | 76 | F | Uveitis | Vitreous chronic inflammation |
| 28 | 52 | F | Uveitis | Aqueous chronic inflammation |
| 29 a | 62 | F | Uveitis | Vitreous chronic inflammation |
Micro–Ribonucleic Acid Array
Total ribonucleic acid including microRNAs in vitreous supernatant was extracted using a commercial column-based system (Qiagen miRNeasy Mini Kit; Qiagen Inc, Gaithersburg, Maryland, USA). Reverse transcription of RNA was performed by using mature microRNA as templates and microRNACURY LNA Universal complementary deoxyribonucleic acid (cDNA) Synthesis Kit according to manufacturer instructions (Exiqon A/S, Vedbaek, Denmark). Six randomly selected samples (primary vitreoretinal lymphoma, n = 3; uveitis, n = 3) were arrayed by an RT-PCR-based microRNA panel that detects 168 human mature microRNAs ( http://www.exiqon.com/microrna-microarray-analysis-microrna-array ) (Exiqon microRNACURY LNA Serum/Plasma Focus microRNA PCR Panel, Part# 203826; Exiqon A/S, Vedbaek, Denmark). RT-PCR was carried out on a StepOnePlus RT-PCR System (Life Technologies, Applied Biosystems Carlsbad, California, USA). Cycling conditions were as follows: 95 C for 10 minutes, 40 cycles of 15 seconds at 95 C, and 60 seconds at 60 C. Fluorescence data were converted into cycle threshold (Ct). The results were normalized by different combinations of 7 control microRNAs (microRNA-103, microRNA-191, microRNA-42-5p, microRNA-16, microRNA-425, microRNA-93, and microRNA-451) as recommended by the manufacturer. The microRNA levels were determined with DataAssist v2.0 Software (Life Technologies, Applied Biosystems). The promising microRNAs with distinct levels between uveitis and lymphoma in the array were further quantified by individual analysis.
Individual Micro–Ribonucleic Acid Assay
The cDNA was synthesized by miScript II RT Kit (Qiagen Inc.). The individual microRNA assay was performed with miScript SYBR Green PCR Kit and miScript Primer Assays according to manufacturer instructions (Qiagen Inc.). A master mix containing 2× QuantiTect SYBR Green PCR Master Mix, 10× miScript Universal Primer, 10× miScript Primer Assay, and RNase-free water was prepared for the primer assay specific to the microRNA of interest. The assays for microRNA-484, microRNA-197, microRNA-132, microRNA-155, microRNA-200c, microRNA-22*, and the reference microRNA-16 were performed in the same plate in triplicate using StepOnePlus real-time PCR system (Life Technologies, Applied Biosystems). Cycling conditions were as follows: 95 C for 10 minutes, 40 cycles of 15 seconds at 95 C, and 60 seconds at 60 C followed by a melting curve analysis. To determine the Ct values, the threshold level of fluorescence was set manually in the early phase of PCR amplification. ABI SDS 1.3.1 software and the 2 −ΔΔCt method was used to determine the relative microRNA level that was first normalized by the level of microRNA-16 from the same cDNA sample and again normalized to the microRNA level in the lower expression group.
Quantitation of Vitreous Interleukin-10 and Interleukin-6 and Immunoglobulin Heavy Chain Gene Rearrangement
The IL-10 and IL-6 levels in vitreous supernatant were measured by ELISA (Quantikine; R&D Systems, Abingdon, UK). Immunoglobulin heavy chain (IgH) gene rearrangement was detected by PCR of extracted DNA from cells collected from ocular fluids using primer pairs of complementarity determining region (CDR) 3, framework region (FR) 3A, and/or FR2A. All 3 primer sets are included in the CDR3 region of the IgH gene, and all can detect rearrangement(s) in CDR3.
Statistical Analysis
The means for microRNA level (fold changes that are in normal distribution) between primary vitreoretinal lymphoma and uveitis groups were compared using the Student’s t test. Differences were considered significant when P < .05. The interaction of microRNA and transcriptional factors were predicted using the web-based transMicroRNA database.
Results
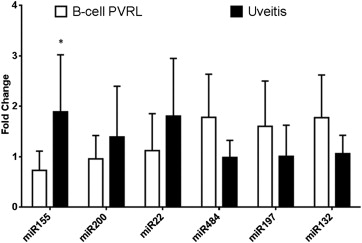
Six vitreous samples (primary vitreoretinal lymphoma, n = 3; uveitis, n = 3) out of 29 samples were selected for array analysis of 168 human mature microRNAs ( Table 1 ). The array detected 110 microRNAs (66.5%) in these samples out of 168 microRNAs printed in the array when the cutoff was set as Ct < 36. For balancing the sample input, the results were normalized by different combinations of 7 control microRNAs (microRNA-103, microRNA-191, microRNA-42-5p, microRNA-16, microRNA-425, microRNA-93, and microRNA-451) as recommended by the manufacturer. After optimization, the normalization against microRNA-16 showed as equally reliable as the average of the 7 control microRNAs. MicroRNA-484, microRNA-197, and microRNA-132 were consistently higher in the primary vitreoretinal lymphoma vitreous compared to that of uveitis, while microRNA-155, microRNA-200c, and microRNA-22* were consistently higher in the uveitis vitreous compared to that of lymphoma. The average microRNA levels of 3 primary vitreoretinal lymphoma and 3 uveitis samples normalized against microRNA-16 are plotted in Figure 1 .
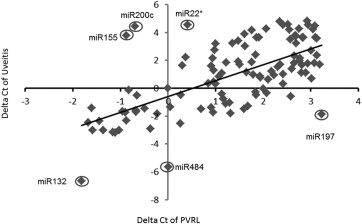
The markers with distinct levels between uveitis and lymphoma were further quantified in the other 23 samples. No difference of microRNA155 between the specimens from aqueous and vitreous in uveitis was measured. After calibration against microRNA-16, groupwise comparisons indicated lower microRNA-484, microRNA-197, and microRNA-132, but higher microRNA-155, microRNA-200c, and microRNA-22*, in the primary vitreoretinal lymphoma than those in uveitic fluids. The microRNA patterns from the individual assays were consistent with those from the array analysis. However, the comparison only shows that microRNA155 in B-cell primary vitreoretinal lymphoma is significantly lower than that in uveitis ( Figure 2 ). Heavy overlap of microRNA155 levels between B-cell primary vitreoretinal lymphoma and uveitis samples was noted.