Purpose
To describe fluocinolone acetonide implant dissociations in the Multicenter Uveitis Steroid Treatment (MUST) Trial.
Design
Randomized clinical trial with extended follow-up.
Methods
Review of data collected on the first implant in the eye(s) of participants. Dissociation was defined as the drug pellet no longer being affixed to the strut and categorized as spontaneous or surgically related.
Results
A total of 250 eyes (146 patients) had at least 1 implant placed. Median follow-up time after implant placement was 6 years (range 0.5–9.2 years). Thirty-four dissociations were reported in 30 participants. There were 22 spontaneous events in 22 participants; 6-year cumulative risk of a spontaneous dissociation was 4.8% (95% confidence interval [CI]: 2.4%–9.1%). The earliest event occurred 4.8 years after placement. Nine of 22 eyes with data had a decline in visual acuity ≥5 letters temporally related to the dissociation. Thirty-nine implant removal surgeries were performed, 33 with replacement. Twelve dissociations were noted during implant removal surgeries in 10 participants (26%, 95% CI 15%–48%); 5 of these eyes had a decline in visual acuity ≥5 letters after surgery. The time from implant placement to removal surgery was longer for the surgeries at which dissociated implants were identified than for those without one (5.7 vs 3.7 years, P < .001). Overall, visual acuity declined 15 or more letters from pre-implant values in 22% of affected eyes; declines were frequently associated with complications of uveitis or its treatment.
Conclusion
There is an increasing risk of dissociation of Retisert implants during follow-up; the risk is greater with removal/exchange surgeries, but the risk of both spontaneous and surgically related events increases with longevity of the implants. In 22% of affected eyes visual acuity declined by 15 letters. In the context of eyes with moderate to severe uveitis for years, this rate is not unexpected.
The fluocinolone acetonide intraocular implant (Retisert; Bausch and Lomb, Bridgewater, New Jersey, USA) is a Food and Drug Administration (FDA)-approved treatment for noninfectious intermediate, posterior, and panuveitis. The fluocinolone acetonide implant is designed to allow sustained release of corticosteroid for approximately 2.5 years. The implant is made of a non-biodegradable polymer and consists of a suture strut that anchors the implant to the eye wall and a drug pellet containing fluocinolone acetonide, which is glued to the strut. The pellet can become unglued from the strut, which is referred to as a “dissociation”; if the pellet also separates from the strut it is characterized as a “dislocated” pellet.
Dissociation of the drug pellet, with or without dislocation, is a recognized complication of treatment with the fluocinolone acetonide implant and typically has been reported to occur without serious sequelae or visual loss. A retrospective study of 224 patients with 407 implants from 2 centers with a median follow-up of 3.4 years (range 0.9–12 years) reported 17 spontaneous dislocations of the drug pellet; the major risk factor for spontaneous dislocations was time since placement of the implant. Three other retrospective case series have reported a total of 9 cases of spontaneous implant dislocations discovered on clinical examination after patients noticed visual symptoms; these events occurred between 2 and 7 years after implant placement. Dissociations, with or without dislocations, have also been reported in conjunction with surgeries to remove and replace implants. Nicholson and associates reported that the pellet was noted to be dissociated from the strut in 40% of 27 surgical procedures occurring between 2001 and 2010; Itty and associates reported a lower frequency, 14% of 77, noted at the time of implant exchange.
The risk of dissociation and dislocation of fluocinolone acetonide implants has not been evaluated prospectively. We reviewed data from the cohort of patients who were enrolled and followed in the Multicenter Uveitis Steroid Treatment (MUST) Trial and Follow-up Study to evaluate the risks of implant dissociation and dislocation and effects on visual acuity. The trial enrolled 255 participants with noninfectious intermediate, posterior, or panuveitis for which systemic corticosteroids were indicated ; participants were randomly assigned to receive either fluocinolone acetonide implants or systemic treatment for uveitis. The results of the MUST Trial after 2 years and 4.5 years of follow-up have been reported ; vision preservation was similar in both groups; the implant was more effective for suppressing uveitis activity but was associated with more ocular side effects, such as cataract and elevated intraocular pressure, and a higher incidence of glaucoma than systemic treatment. Herein, we report the occurrence of dissociations and dislocations for the first fluocinolone acetonide implant placed in each eye with uveitis in the MUST Trial and Follow-up Study.
Methods
Participants
Details regarding the design, surgical techniques, baseline characteristics, and 2-year and 4.5-year results of the original MUST Trial are reported elsewhere. Briefly, eligible patients 13 years of age or older were enrolled in the MUST Trial at 23 centers in the United States, the United Kingdom, and Australia between December 6, 2005 and December 9, 2008. Patients meeting the eligibility criteria in both eyes were assigned to receive the same treatment in both eyes. Participants under follow-up at the end of the trial period (December 2010) were invited to continue follow-up in the MUST Follow-up Study that commenced in January 2011 and currently is ongoing. All participants signed informed consent statements for the trial approved by the clinical center institutional review boards (IRBs). Participants that continued in the MUST Follow-up Study signed a second IRB-approved consent statement for that study. The clinical trial is registered at ClinicalTrials.gov ( NCT00132691 ). Both MUST studies are in compliance with HIPAA regulations.
Data Collection
Participants were seen every 3 months during the MUST Trial period (December 2005 to December 2010) and every 6 months in the MUST Follow-up Study (January 2011 to database closure for this analysis in March 2015). Visits include slit-lamp and indirect ophthalmic examinations, color fundus photography, and best-corrected visual acuity assessments according to Early Treatment Diabetic Study procedures. Placement and removal of implants were performed by MUST Trial–certified ophthalmic surgeons, and data regarding these surgeries were collected.
This analysis includes all eyes that received a fluocinolone acetonide implant during the course of the MUST Trial or Follow-up Study between December 2005 and March 2015, regardless of the original treatment assignment or uveitis status at baseline. Results are limited to the first implant(s) a participant received in an eye(s) with uveitis during the trial or follow-up study.
Main Outcome Measures
The main outcome was dissociation of the implant; dissociated implants were further classified as being dislocated (separated from the strut) or not. There were 2 circumstances under which the dissociations were identified: (1) spontaneous events identified or confirmed by clinical examination; and (2) events that were identified during implant removal surgery. For events identified during surgery it was not possible to definitively distinguish between pre-existing events and those caused by surgery. Hence, we grouped both types of surgery-related events together in this report. A decline or improvement in visual acuity was defined as a change of 5 or more letters; stable vision was defined as a visual acuity measurement within 5 letters of the comparator measurement.
Statistics
Time to spontaneous dissociation was measured from the date that the implant was placed until the date of the discovery or confirmation of a spontaneous dissociation at a clinic visit. Implanted eyes without a spontaneous dissociation were censored at the date of removal or the date of last follow-up, whichever came first. Kaplan-Meier estimates of the survivor function were used to graphically display the cumulative proportion with a spontaneous dissociation. For surgical dissociations, generalized estimating equations were used to fit regression models while accounting for between-eye correlation. Logistic regression was used to estimate the 95% confidence interval (CI) of the point estimate for probability of dissociation, and linear regression was used to compare the time from implantation to surgery for those who had a dissociation as compared to those that did not. Robust standard error estimates were computed. Statistical analyses were performed using SAS (SAS/STAT User’s Guide Version 9.2; SAS Institute, Cary, North Carolina, USA) and R (The R Project for Statistical Computing, version 2.13.1, http://www.r-project.org/ ).
Results
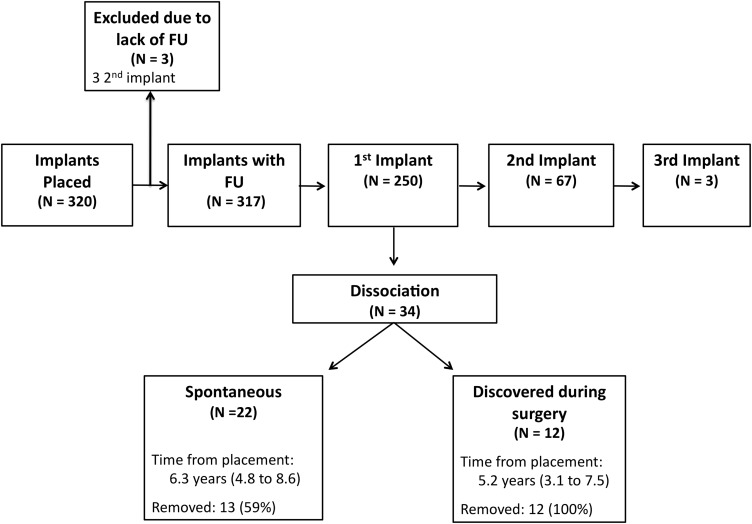
Between December 30, 2005 and February 15, 2015, 320 implants were placed; 250 were first implants, 67 were second implants, and 3 were third implants ( Figure 1 ). The 250 first implants were placed in the eye(s) of 146 of the 255 participants enrolled in the trial and form the basis of this report. Most of these participants, 71% (104 of 146), had implants placed in both eyes. The characteristics of the participants at the visit prior to implant placement surgery were similar to the overall MUST Trial cohort at baseline ( Table 1 ). Sixty-two percent these participants had posterior or panuveitis, and 27% of participants had uveitis associated with a systemic disease. Most participants (59%) self-identified as white, and most were women (74%). The median time since diagnosis of uveitis was 4.5 years (range 0–40.5 years) at the time of implantation. Median baseline visual acuity in the eye(s) with uveitis at baseline was 65 letters, which corresponds to a logMAR of 0.4 and a Snellen equivalent of 20/50. The median follow-up time after placement of the first study implant was 6.0 years (range 0.5–9.2 years). Of the 250 first implants, a total of 34 implants were identified as having dissociated, 29 with dislocation; these events occurred in 30 participants; 4 participants had dissociated implants in both eyes.
| Characteristics | Result |
|---|---|
| Number of patients | 146 |
| Median age at first implantation, years (range) | 48 (13–87) |
| Male, number (%) | 38 (26%) |
| Race, number (%) | |
| White | 86 (59%) |
| African American | 20 (14%) |
| Hispanic | 37 (25%) |
| Other | 3 (2%) |
| Associated systemic disease, n (%) | 39 (27%) |
| Posterior/panuveitis, n (%) | 90 (62%) |
| Bilateral uveitis, n (%) | 131 (90%) |
| Bilateral implants, n (%) | 104 (71%) |
| Eye-level characteristics | |
| Number of eyes | 250 |
| Median years since onset of uveitis (range) a | 4.5 (0.1–40.5) |
| Median visual acuity, letters (range) a | 65 (−10 to 96) |
| Median visual acuity, Snellen equivalent a | 20/50 |
| Macular edema, n (%) a | 83 (36%) |
| Observation years from first implant (range) | 6.0 (0.5–9.2) |
a Number of observations for years of onset of uveitis = 245, visual acuity = 248, and macular edema = 230.
Spontaneous Dissociations
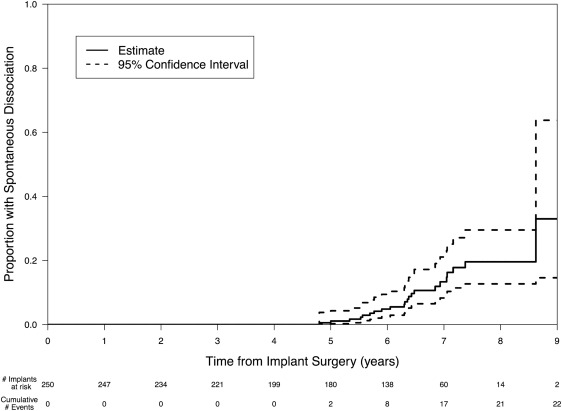
Spontaneous dissociations were identified in 22 eyes of 22 participants between 4.8 and 8.6 years after placement ( Table 2 ). In all cases the drug pellet was dislocated from the strut as well. Only 1 event was observed before 5 years (at 4.8 years) and the cumulative risk climbed to 4.8% (95% CI: 2.4%–9.1%) by 6 years ( Figure 2 ). Most events (68%) were identified after the participant reported visual symptoms such as black spots and blurred or decreased vision; 7 events (32%) were asymptomatic and identified during a clinical examination.
| Participant Number/Eye | Detection Method | Years in Place | Visual Acuity in Logarithmic Acuity Chart Letters a (Months From Reference Point) | Visual Acuity Status b | ||||
|---|---|---|---|---|---|---|---|---|
| Prior to Implant | Prior to Dissociation | At/After Dissociation | Last Measured | Prior to Dissociation vs At/After Dissociation | Prior to Implant vs Last Follow-up | |||
| Implant removed | ||||||||
| S6/right eye | Symptoms | 4.8 | 54 (−0.9) | 45 (−4) | 36 (0) | 66 (32) | Declined | Improved |
| S16/left eye | Symptoms | 5.0 | 75 (−2.6) | 81 (−3) | 70 (0) | 82 (9) | Declined | Improved |
| S7/right eye | Symptoms | 5.3 | 61 (−2.5) | 82 (−18) | 70 (2) | 80 (23) | Declined | Improved |
| S12/left eye | Examination | 5.7 | 37 (−1.3) | 49 (−3) | −10 (3) | −10 (3) | Declined | Declined |
| S26/right eye | Examination | 6.1 | 66 (−1.7) | 35 (−1) | 65 (1.1) | 66 (1.1) | Stable | Stable |
| S4/left eye | Symptoms | 6.3 | 70 (−0.4) | 36 (−4) | 3 (2) | 23 (14) | Declined | Declined |
| S15/left eye | Symptoms | 6.3 | 71 (−0.2) | 60 (−4) | 55 (0) | 67 (3) | Stable | Stable |
| S11/left eye | Symptoms | 6.4 | NA | 59 (−2) | 60 (0) | 36 (5) | Stable | NA |
| S10/left eye | Symptoms | 6.5 | 93 (−0.9) | 85 (−2) | 86 (3) | 87 (8) | Stable | Declined |
| S8/right eye | Symptoms | 7.1 | 77 (−1.3) | 81 (−3) | −10 (1) | 53 (8) | Declined | Declined |
| S29/right eye | Symptoms | 7.2 | 43 (−11) | 44 (−3) | 44 (3) | 44 (3) | Stable | Stable |
| S9/right eye | Symptoms | 7.4 | 69 (−0.5) | 51 (−7) | NA | NA | NA | NA |
| S28/right eye | Examination | 8.6 | 76 (−0.5) | 12 (−4) | 36 (5) | 36 (5) | Stable | Declined |
| Implant remains in eye | ||||||||
| S1/right eye | Symptoms | 5.5 | 61 (−2.1) | 77 (−3) | 85 (1) | 87 (8) | Stable | Improved |
| S2/left eye | Symptoms | 5.6 | 61 (−1.3) | 47 (−6) | 43 (0) | 48 (19) | Stable | Declined |
| S27/left eye | Examination | 5.8 | −10 (−1.6) | −10 (−6) | −10 (0) | −10 (0) | Stable | NA |
| S3/right eye | Examination | 5.9 | 46 (−0.9) | 85 (−8) | 58 (0) | −10 (18) | Declined | Declined |
| S5/right eye | Examination | 6.4 | 52 (−1.7) | 42 (−1) | 25 (5) | 23 (24) | Declined | Declined |
| S13/left eye | Symptoms | 6.4 | 37 (−1.0) | 58 (−1) | 60 (0.7) | 60 (5) | Stable | Improved |
| S17/left eye | Symptoms | 6.8 | 78 (−0.7) | 69 (−2) | 55 (0) | 69 (4) | Declined | Declined |
| S14/right eye | Examination | 6.9 | 77 (−0.1) | 75 (−1) | 70 (0) | 82 (8) | Stable | Stable |
| S30/right eye | Symptoms | 7.0 | 38 (−0.7) | 66 (−2) | 66 (4) | 80 (12) | Stable | Improved |
a 85 letters = 20/20, 70 letters = 20/40, 50 letters = 20/100, and 35 letters = 20/200.
b Declined = decrease in visual acuity of more than 1 line (5 letters) from predissociation visit or from preimplant visits; Improved = increase in visual acuity of more than 1 line.
Thirteen of the dislocated implants and 7 of the corresponding struts were surgically removed; 11 were removed without significant complications. Two eyes had retinal detachments associated with surgery and 1 of these eyes required a second surgery to remove the dislocated drug pellet. A second implant was placed in 6 of the 12 eyes: 4 during and 2 prior to the surgery to remove the first implant.
Twelve eyes had follow-up data on visual acuity after the dissociation. Visual acuity declined by more than 1 line (5 letters) in 6 of the 12 eyes as measured within 5 months of dissociation ( Table 2 , Supplemental Figure 1 , available at AJO.com ). Three of the 6 eyes with declines ranging from 33 to 91 letters did not recover to pre-dissociation visual acuity, although 2 of the 3 showed substantial improvement (ie, 20 to 63 letters). Three eyes with declines ranging from of 9 to 13 letters temporally related to dissociation subsequently improved to a visual acuity exceeding the pre-event acuity. The remaining 6 eyes with follow-up had stable visual acuity after the discovery of the dissociation. Causes cited for the persistent declines were exudative retinal detachment, postoperative air-fluid vitrectomy and subretinal fibrosis, and epiretinal membrane with corneal opacity and a macular hole; other causes of decline cited were macular hole, chorioretinal atrophy, and hypotony with vitreous haze. Overall 6 of 11 eyes with sufficient data to evaluate had visual acuity ranging from −5 to +19 letters of the value measured prior to implant surgery 5.8–9 years after the implant was placed. In the 4 eyes with declines ranging from 6 to 47 letters 6–9 years after surgery, only 1 was directly linked to the removal surgery. In the other 3 cases complications cited as affecting visual acuity were macular edema (2), retinal atrophy (2), retinal detachment (1), and hypotony with vitreous haze (1) (see Supplemental Text for details on individual cases, available at AJO.com ).
Nine dislocated implants were not removed as of October 2015. We did not systematically record the rationale for not removing implants, although some forms noted that there were no vision loss or troublesome symptoms associated with the event so the decision was to continue observation. The observation time after the dislocated implant was identified in these 9 eyes ranged from 0 to 24 months, with a median time of 12 months ( Table 2 , Supplemental Figure 2 ). Three of these 9 eyes had a decline in visual acuity of more than 1 line at the first measurement available after the dissociation was identified. One eye with a history of corneal clarity problems and macular edema, recovered to pre-dissociation visual acuity within 4 months. The remaining 2 eyes with persistent visual acuity loss had other complications: 1 that declined to -10 letters had cystoid macular edema and an epiretinal membrane; the other had hypotony and corneal edema associated with migration of a sustained-release dexamethasone pellet (Ozurdex; Allergan, Inc, Irvine, California, USA) into the anterior chamber. One eye with poor visual acuity prior to implantation (-10 letters) continued to have poor visual acuity throughout follow-up. The remaining 5 eyes had stable visual acuity after the discovery of the dissociation and continued to be stable or improved for the remainder of follow-up. In comparison to the visual acuity prior to implant placement, 4 of these 9 eyes had visual acuity decreases of more than 5 letters 6.2–9.1 years after implant surgery. In addition to the 2 cases noted above, 2 other eyes had 9- and 13-letter declines from their pre-surgery visual acuity that were attributed to glaucoma and corneal clarity with macular dysfunction, respectively (see supplemental Figure 2 , available at AJO.com , for details).
Dissociations Associated With Surgery
There were a total of 39 implant removal/exchange surgeries performed (excluding surgeries performed to remove implants that spontaneously dissociated) at 12 centers to remove the first implant (n = 6) or to replace the initial implant (n = 33). Twelve implant dissociations (26%, 95% CI: 15%–48%) were noted during surgery in 10 participants ( Table 3 ); 7 of these implants were dislocated from the anchoring struts. No complications were noted during surgery for 10 eyes; in the remaining 2 eyes the drug pellet dislocated during surgery and was not removed. The time from implant placement to removal surgery was longer for the surgeries at which a dissociation was identified compared to those without a dissociation, 5.5 vs 3.7 years ( P < .001).



