Visual acuity (VA) criteria were 20/40 or better for eyes without macular edema and 20/200 or better for those with macular edema. Eyes with macular edema were analyzed separately as one arm of the study.
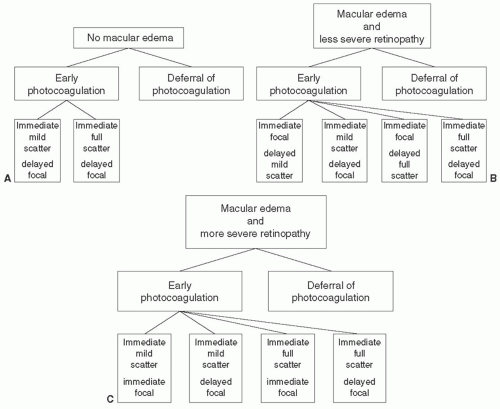 FIGURE 7B.1 (A) Early Treatment Diabetic Retinopathy Study (ETDRS) photocoagulation treatment scheme for eyes without macular edema and moderate-to-severe nonproliferative or early proliferative retinopathy. Eyes were assigned randomly to early photocoagulation or deferral of photocoagulation. Eyes assigned to early photocoagulation were further assigned randomly to either mild or full scatter (panretinal) photocoagulation. (From Early Treatment Diabetic Retinopathy Study Research Group. Early Treatment Diabetic Retinopathy Study design and baseline characteristics. ETDRS Report No 7. Ophthalmology. 1991;98:741-756.) (B) ETDRS photocoagulation treatment scheme for eyes with macular edema and less severe retinopathy (mild-to-moderate nonproliferative retinopathy). Eyes were assigned randomly to early photocoagulation or to deferral of photocoagulation. Eyes assigned to early photocoagulation were further assigned randomly to either mild or full scatter (panretinal) photocoagulation, and to either immediate focal or delayed focal treatment. For eyes assigned to immediate focal treatment, the assigned scatter treatment was not applied initially, but only if severe nonproliferative retinopathy or worse developed during follow-up. (From Early Treatment Diabetic Retinopathy Study Research Group. Early Treatment Diabetic Retinopathy Study design and baseline characteristics. ETDRS Report No 7. Ophthalmology. 1991;98:741-756.) (C) ETDRS photocoagulation treatment scheme for eyes with macular edema and more severe retinopathy. Eyes were assigned randomly to early photocoagulation or to deferral of photocoagulation. Eyes assigned to early photocoagulation were further assigned randomly to either mild or full scatter (panretinal) photocoagulation, and to either immediate focal or delayed focal treatment for at least 4 months. (From Early Treatment Diabetic Retinopathy Study Research Group. Early Treatment Diabetic Retinopathy Study design and baseline characteristics. ETDRS Report No 7. Ophthalmology. 1991;98:741-756.) |
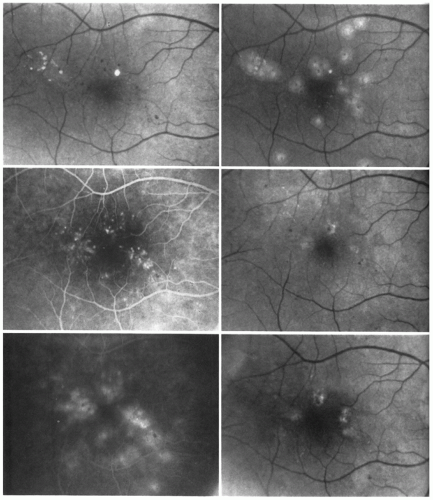 FIGURE 7B.2 Focal treatment of microaneurysms. The right eye of a 69-year-old woman with diabetes of 22 years’ duration. Top left: At baseline visit, definite retinal thickening could be seen (with stereoscopic examination) nasal to the center of the macula and above it, probably involving the center. A few small microaneurysms and hard exudates are visible in the thickened area. Visual acuity was 20/30. Center left: Mid-phase angiogram shows microaneurysms surrounding the center of the macula most within 1,000 µm of the center and some within 500 µm. Bottom left: Late-phase angiogram shows leakage from the microaneurysms. Top right: Posttreatment photograph shows mild-to-moderate intensity focal treatment of most of the microaneurysms. The microaneurysms closest to the center have not been treated. Center right: One year after treatment, the center of the macula appears flat. Hard exudates and microaneurysms have decreased. Visual acuity was 20/50. Bottom right: Between the 1- and 2-year visits, additional focal photocoagulation was applied. At the 2-year visit, the center of the macula appears flat and no microaneurysms or hard exudates can be seen. Visual acuity was 20/25. (From Early Treatment Diabetic Retinopathy Study Research Group. Treatment technique and clinical guidelines for photocoagulation of diabetic macular edema. ETDRS Report No 2. Ophthalmology. 1987;94:761-774.) |
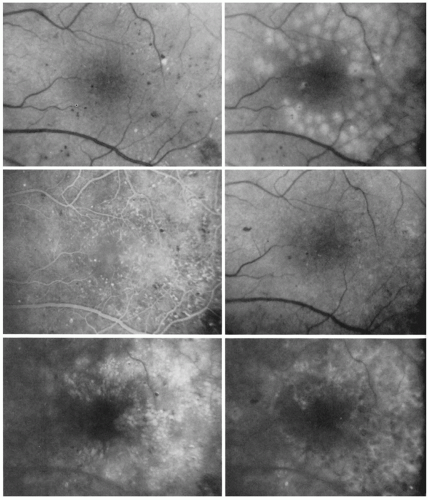 FIGURE 7B.3 Focal treatment of microaneurysms combined with a grid patter to areas of diffuse fluorescein leakage and capillary dropout. The left eye of a 49-year-old man with diabetes of 22 years’ duration. Top left: The pretreatment photograph shows extensive retinal thickening with a few scattered microaneurysms and small hard exudates temporal to the center of the macula. Retinal thickening at the center is mild. Visual acuity was 20/40. Center left: Mid-phase angiogram shows moderate capillary dilation above and temporal to the center of the macula, with mild perifoveal capillary dropout. Scattered microaneurysms are also present. Bottom left: Late-phase angiogram shows extensive small cystoid spaces above, below, and temporal to the center of the macula. Some of the large microaneurysms fill only partially with fluorescein. Top right: Posttreatment photograph shows focal burns to microaneurysms and a grid pattern of burns above, below, and temporal to the macula. Center right: Four months later, microaneurysms and hard exudates have decreased. Retinal thickening is less and no longer involves the center of the macula. Visual acuity was 20/25. Bottom right: Late-phase angiogram shows treatment scars but most of the microaneurysms and cystoid spaces have disappeared. (From Early Treatment Diabetic Retinopathy Study Research Group. Treatment technique and clinical guidelines for photocoagulation of diabetic macular edema. ETDRS Report No 2. Ophthalmology. 1987;94:761-774.) |
TABLE 7B.1 Specific Techniques for Scatter (Panretinal) and Focal Photocoagulation in the Early Treatment Diabetic Retinopathy Study | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
TABLE 7B.2 Definition of Clinically Significant Diabetic Macular Edema | ||||||||
|---|---|---|---|---|---|---|---|---|
| ||||||||
foveal involvement, treatment resulted in a lesser, but significant, benefit (6% for treated eyes vs. 16% untreated at 2 years). In contrast, in eyes with macular edema that did not meet the definition of CSDME, there was no benefit associated with treatment (see Fig. 7B.4).5,6,7
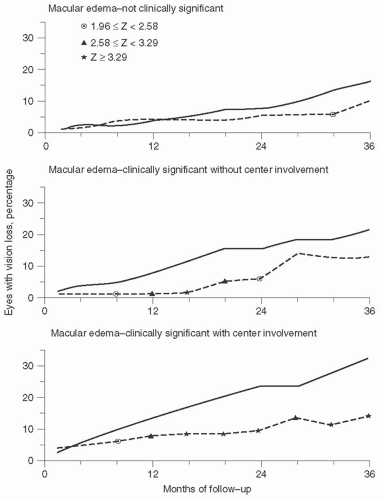 FIGURE 7B.4 Comparison of percentages of eyes with macular edema that experienced moderate visual loss classified by severity of macular edema and assigned to immediate focal treatment (broken line) or to deferral of treatment (solid line). (From Early Treatment Diabetic Retinopathy Study Research Group. Photocoagulation for diabetic macular edema. Early Treatment Diabetic Retinopathy Study Report No 4. Int Ophthalmol Clin. 1987; 27:265-272.) |
but not statistically significant, difference in visual field scores. Eyes assigned to focal photocoagulation demonstrated slightly more paracentral scotomata on Goldmann visual fields using the I-2 test object.6
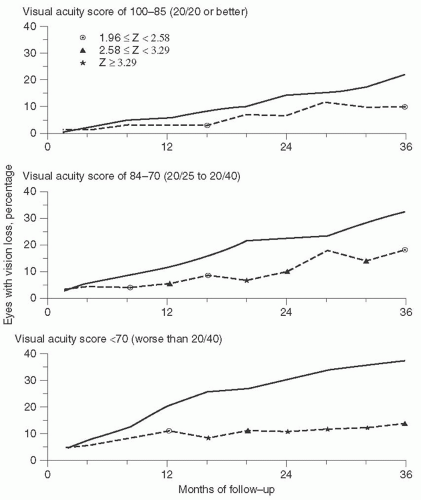 FIGURE 7B.5 Comparison of percentages of eyes with clinically significant diabetic macular edema that experienced moderate visual loss classified by baseline visual acuity and assigned to immediate focal treatment (broken line) or to deferral of treatment (solid line). (From Early Treatment Diabetic Retinopathy Study Research Group. Photocoagulation for diabetic macular edema. Early Treatment Diabetic Retinopathy Study Report No 4. Int Ophthalmol Clin. 1987; 27:265-272.) |
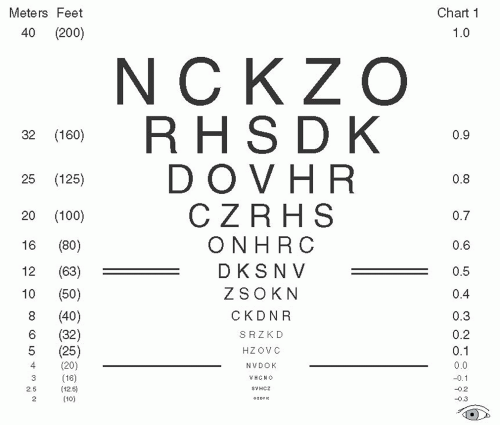 FIGURE 7B.6 One of the three Early Treatment Diabetic Retinopathy Study visual acuity charts. Fourmeter testing distance with this chart yields the following Snellen equivalent lines: 20/10, 20/12.5, 20/16, 20/20, 20/25, 20/31.5, 20/40, 20/50, 20/63, 20/80, 20/100, 20/125, 20/160, and 20/200. At 1 m, the following additional Snellen equivalent lines of visual acuity could be measured: 20/250, 20/315, 20/400, 20/500, 20/630, and 20/800. Note that every three lines is a doubling of the visual angle and that there are five letters on each line. (From Early Treatment Diabetic Retinopathy Study Research Group. Early Treatment Diabetic Retinopathy Study design and baseline characteristics. ETDRS Report No 7. Ophthalmology. 1991;98:741-756.) |
treatment remains unknown. Furthermore, the ETDRS used specific treatment guidelines for macular focal photocoagulation. Alternative laser treatment strategies have since been developed, including modified versions of the ETDRS protocol. The relative benefits of different treatment strategies are difficult to assess since a direct comparison with the ETDRS results is not possible.
 FIGURE 7B.7 Triamcinolone acetonide (Kenalog-40, Bristol-Myers Squibb). (Photograph courtesy of Ronald C. Gentile, MD, New York, NY.) |
clinical trials dedicated to the investigation of diabetic retinopathy. There are currently over a hundred participating clinical sites.15 Its establishment represented a unique paradigm where multiple centers, from academic institutions to private practices, could rapidly organize large trials.
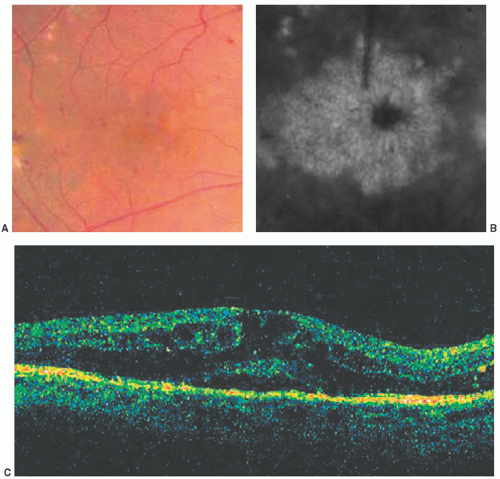 FIGURE 7B.8 The right eye of a 49-year-old man with diabetes of 18 years’ duration. Clinically significant diabetic macular edema was present despite a history of prior focal photocoagulation. Visual acuity was 20/200. (A) Fundus photograph of the macula shows cystoid retinal thickening, a few small retinal hemorrhages, and prior focal laser spots. (B) Late-phase fluorescein angiogram shows leakage in a petalloid pattern. (C) Optical coherence tomography shows cystic retinal thickening. |
and no expectations for requiring PRP in the subsequent 4 months. Patients with any history of intravitreal steroid treatment or pars plana vitrectomy, or those with recent periocular steroids or photocoagulation treatment were excluded. Also excluded were those with histories of open-angle glaucoma, steroid-induced ocular hypertension that required intervention, and intraocular pressure (IOP) of 25 mmHg or more. Baseline characteristics showed that the DRCR.net study patients were slightly older with better glycemic control compared to the ETDRS and PKC-DRS2 participants.17 Other variables were similar.
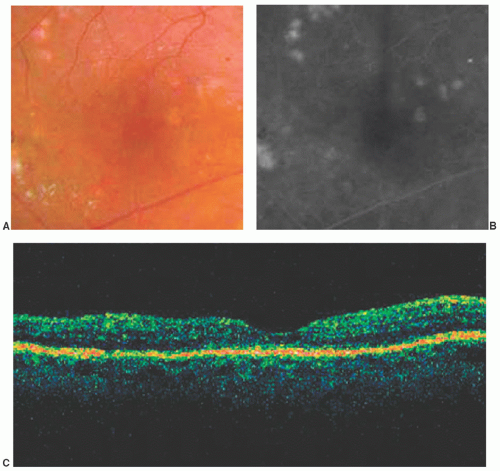 FIGURE 7B.9 Same patient as in Figure 8, 3 months after intravitreous injection of triamcinolone acetonide 4 mg. Visual acuity was 20/80. (A) Fundus photograph shows resolution of macular edema. (B) Late-phase fluorescein angiogram shows resolution of leakage. (C) Optical coherence tomography shows resolution of retinal thickening. (Three months later the patient developed recurrent edema and underwent repeat injection, with subsequent resolution of the edema.) |
certain failure criteria as a fail-safe system. Patients were followed every 4 months, and retreated based on VA and OCT parameters. The primary endpoint was mean VA, and the secondary outcome measure was central subfield retinal thickness. At the time, this DRCR.net study was the first phase III DRS to use the OCT data.
 FIGURE 7B.10 Fluocinolone acetonide intravitreous sustained release implant (Retisert). |
 FIGURE 7B.11 Fluocinolone acetonide intravitreous sustained release insert and its injector (Iluvien). |
 FIGURE 7B.12 Dexamethasone intravitreous sustained release implants (Ozurdex), 350 and 700 µg doses, and the injector. |
starting at 16 months and persisting to 2 years the laser group developed the best mean VA (see Fig. 7B.13). At 2 years, the mean ± SD change in VA was +1 ± 17 letters in the laser group, — 2 ± 18 letters in the 1-mg group (p = 0.02), and − 3 ± 22 letters in the 4-mg group (p = 0.002). The number of treatments in each arm was similar. A subgroup analysis of pseudophakic eyes showed that the respective changes in mean visual acuities were + 2 ± 18, +2 ± 17, and −1 ± 19 letters. This analysis was performed because intravitreal steroids are strong risk factors for developing cataract.
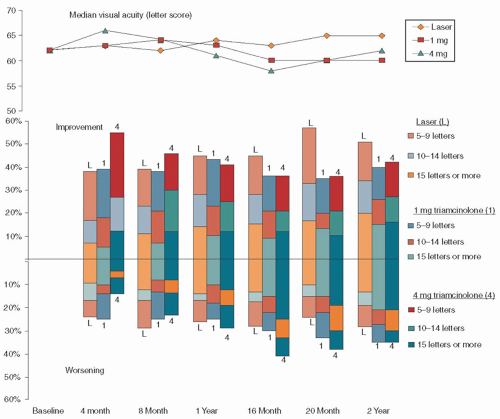 FIGURE 7B.13 Diabetic Retinopathy Clinical Research Network (DRCR.net), Protocol B. The study compared the efficacies of focal/grid photocoagulation, and 1 or 4 mg of intravitreal triamcinolone, in the treatment of diabetic macular edema. The top graph demonstrates the changes in visual acuity over 2 years. The bottom graph shows the percentages of eyes in each treatment group with the corresponding letters gained or lost at each time point. (From Diabetic Retinopathy Clinical Research Network. A randomized trial comparing intravitreal triamcinolone acetonide and focal/grid photocoagulation for diabetic macular edema. Ophthalmology. 2008;115:1447-1449.) |
observed at one or more visits in 40% of those in the 4-mg group, 20% in the 1-mg group, and 10% in the laser group (all p < 0.001). Cataract surgery was performed in 51% of the 4-mg group, 23% of the 1-mg group, and 13% of the laser group, during the course of the study (p < 0.001). A unique adverse event in this study was intravitreal silicone oil droplets that were found in some eyes due to the use of staked silicone syringes. The protocol was amended to use luer cone syringes instead, which eliminated the problem.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


