Purpose
To compare the efficacy of customized corneal cross-linking (CXL) with standard CXL.
Design
Prospective, nonrandomized comparative clinical study.
Methods
In a prospective study at the Institut für Refraktive und Ophthalmo-Chirurgie (IROC), Zurich, Switzerland, 40 eyes of 40 patients with documented progressive primary keratoconus were treated with customized CXL (n = 20) or standard CXL (n = 20) and followed for 1 year. Customized irradiation patterns had an energy fluence of 9 mW/cm 2 and total energy levels ranging from 5.4 J/cm 2 up to 10 J/cm 2 and were centered on the maximum of the posterior float. The control group received homogenous irradiation with a fluence of 9 mW/cm 2 and a total energy of 5.4 J/cm 2 . Scheimpflug tomographies, endothelium cell count, best spectacle-corrected visual acuity (BSCVA), and anterior segment optical coherence tomography (OCT) were compared preoperatively and 1 year postoperatively.
Results
Pachymetry and ΔK max showed significant changes 1 year postoperatively within each group. Epithelial healing time, ΔK max , and regularization index (RI) were significantly better in the customized CXL group. Two out of 19 eyes (11%) in the standard group but 7 out of 19 eyes (37%) in the customized CXL group showed a flattening of 2 or more diopters ( P = .03). The RI was 5.2 ± 2.7 D in the customized group vs 4.1 ± 3.1 D in the control group ( P = .03). Statistically significant correlations between RI and preoperative K max , preoperative pachymetry, and preoperative posterior float were found only in the customized group.
Conclusions
Customized CXL seems to be as safe as standard CXL with stronger flattening in K max and RI, and a faster epithelial healing period.
Nearly 20 years ago, corneal cross-linking (CXL) by means of riboflavin and ultraviolet (UV) light was proposed as a therapeutic approach to strengthen biomechanical and biochemical properties of the cornea (Seiler T, et al. Conservative therapy of keratoconus by enhancement of collagen cross-links. IOVS 1996;37:ARVO E-Abstract 4671). Meanwhile, there is clinical evidence that CXL is a useful operation to stop the progression of both primary and secondary keratectasia, with a failure rate of approximately 3%–10% and a complication rate of 1%–13%. In standard CXL, a circular 9 mm area of the corneal surface is de-epithelialized and during the period of reepithelialization the cornea is vulnerable. Not surprisingly, it is during the early postoperative period that most of the complications, such as infections and ulcerations, may occur.
Biomechanical modeling of the cross-linked cornea revealed that for the stabilization of the keratoconus there is no need to strengthen the entire cornea, but similar results could be obtained if only the weak parts of the keratoconus cornea were to be treated. Following this strategy, weaker parts of the cornea need to be more strongly treated (more applied energy inducing more radicals) and more stable parts of the cornea treated with less or even no UV light. Such customized CXL employs UV light with a defined intensity profile.
This approach raises the question of the location of the weakest area of the cornea. Since an objective measurement of the elastic modulus is clinically not yet available, we have to rely on geometric parameters of the cornea, such as the point of maximal curvature or of maximal posterior float.
In this prospective study, the 1-year results of customized CXL are compared to a control group that received standard epi-off CXL with 9 mW/cm 2 .
Methods
Study Groups and Protocol
Twenty eyes of 20 patients with documented progressive primary keratoconus (progression was defined as an increase of K max of at least 1 diopter [D] within up to 1 year, measured by corneal tomography [Pentacam HR 70700; Oculus, Wetzlar, Germany]) were enrolled in this study. Excluded were eyes with previous ocular surgery, penetrating trauma, glaucoma, or aphakia; endothelial cell count less than 2300 cells/mm 2 ; corneas with no distinctive posterior float area; corneas with pellucid marginal degeneration; corneal scars that may interfere with Scheimpflug photography; history of recurrent erosions; patients younger than 18 years; pregnancy and breastfeeding; nonavailability for follow-up examinations during 1 year; neurodermatitis; and connective tissue diseases. The study protocol was approved by the institutional review board of the Institut für Refraktive und Ophthalmo-Chirurgie (IROC). Of the 20 patients, 19 completed the 1-year follow-up (dropout rate: 5%), all patients completed the 6-month follow-up. After completion of the study group, standard epi-off CXL was applied to a control group that was matched to the study group regarding group size, inclusion criteria, age, and sex. Also in this group, only 1 eye per patient was included.
The patients were examined preoperatively, early postoperatively (daily until epithelium healing), and at 1 month, 6 months, and 12 months after customized CXL or standard CXL. At every follow-up, except early postoperative, a standard examination was performed consisting of autorefractometry and autokeratometry (Humphrey Model 599; Zeiss, Jena, Germany), corneal topography (Keratograph C; Oculus), Scheimpflug imaging (Pentacam HR 70700; Oculus), optical coherence tomography (OCT) (SS-1000; Tomey, Nagoya, Japan), manifest refraction using the fogging technique, uncorrected (UDVA) and best spectacle-corrected visual acuity (BSCVA), applanation tonometry, endothelial cell count (SP-02; Costruzione Strumenti Oftalmici, Scandicci Firenze, Italy) and slit-lamp examination. Patients were asked not to use contact lenses during the first postoperative month and 2 weeks before each examination.
Treatments
The control group underwent a standard CXL procedure including a circular epithelium debridement with a diameter of 9.0 mm (Epi clear; Orca Surgical, Caesarea, Israel) and application of 0.1% riboflavin in 16% dextran T500 for 30 minutes. Ultrasound pachymetry at the thinnest point was repeated every 10 minutes (SP-100; Tomey). If pachymetry fell below 400 μm the imbibition with riboflavin was continued using hypo-osmolar riboflavin 0.1% drops until the thickness was 400 μm. The cornea was irradiated with 9 mW/cm 2 for 10 minutes (UVX 2000; IROC Innocross, Zurich, Switzerland).
The customized CXL group underwent a similar procedure except using a smaller eccentric debridement area and a customized UV irradiation profile (Mosaic System; Avedro Inc, Waltham, Massachusetts, USA). The profiles were designed as a concentric superposition of 3 circular areas ( Figure 1 ) centered on the maximum of the posterior float (reference: sphere, 8 mm approximation). The inner circle’s diameter was equal to the shortest diameter of the posterior float minus 0.5 mm (range, 1.9–2.9 mm); the outer circle’s diameter was 1 mm bigger than the maximal diameter of the posterior float (range, 5.2–6.5 mm). The middle circle’s diameter was the mean of the other 2 diameters. The radiance exposure in the inner circle was 10 J/cm 2 , in the middle 7.5 J/cm 2 , and in the outer 5.4 J/cm 2 . The fluence was 9 mW/cm 2 . Small eye movements were compensated by the eye tracker of the Mosaic System.
For both groups, antibiotic ointment (Floxal; Bausch & Lomb, Zug, Switzerland) and a bandage contact lens were applied to the eye and patched until epithelial healing. Thereafter, topical treatment consisted of fluorometholone eye drops (FML; Allergan, Zurich, Switzerland) 3 times per day for 1 week and taper during weeks 2 and 3.
Evaluation
The following parameters were used for quantitative evaluation: BSCVA, K max , maximal posterior float, central endothelial cell count, pachymetry of the thinnest point, and maximal depth of the demarcation line. Optical pachymetry using Scheimpflug tomography was discarded for follow-up evaluation because information from the rear surface may be erroneous in hazy corneas. A new parameter (regularization index; RI) was introduced to describe the regularization of the corneal surface within a 6 mm circle around the apex ( Figure 1 ): absolute amount of maximal flattening (usually in steep areas) plus absolute amount of maximal steepening (usually in flat areas). Comparisons of parameters between the 2 groups were performed using the Mann-Whitney U test. Comparisons of parameters at different times were performed by means of the Wilcoxon rank sum test. Correlations and their significance were tested using the Spearman rank correlation test. All calculations were performed with WinSTAT for Excel (R. Finch Software, 2015, Bad Krozingen, Germany). Statistical significance was accepted if P < .05.
Results
The demographic and preoperative tomographic parameters of the 2 groups are listed in Table 1 . The 2 groups did not show any significant difference preoperatively.
| cCXL (n = 19) | sCXL (n = 19) | P Value | |
|---|---|---|---|
| Age (y) | 28.7 ± 6.3 | 25.9 ± 6.7 | .21 |
| Side (OD:OS) | 8:11 | 9:10 | .73 |
| Sex (M:F) | 15:4 | 13:6 | .42 |
| Endothelial cell count (cells/mm 2 ) | 2824 ± 256 | 2899 ± 277 | .55 |
| K max (D) | 57 ± 6.7 | 55.3 ± 5.3 | .31 |
| Thinnest pachymetry (μm) | 463 ± 42 | 447 ± 35 | .15 |
| BSCVA (logMAR) | 0.31 ± 0.26 | 0.35 ± 0.32 | .82 |
| Posterior float (μm) | 72 ± 35 | 65 ± 23 | .44 |
In 1 eye in the customized group sterile infiltrates occurred; all other eyes showed an uneventful postoperative course. The epithelium erosion was fluorescein positive for 2.56 ± 0.50 days in the customized CXL group and 3.19 ± 0.73 days in the standard CXL group; this difference was statistically significant ( P = .02).
The demarcation line at 1 month after surgery had a substantially different appearance in the 2 groups: whereas it had a more Gaussian shape with a peak depth of 77% ± 15% (absolute 338 ± 77 μm) of the thinnest pachymetry in the customized CXL group, it showed uniform surface parallel depth of 81% ± 10% (absolute 357 ± 51 μm) in the standard CXL group ( Figures 1 and 2 ). The maximal depth of the demarcation line was in both groups not statistically different ( P = .50).
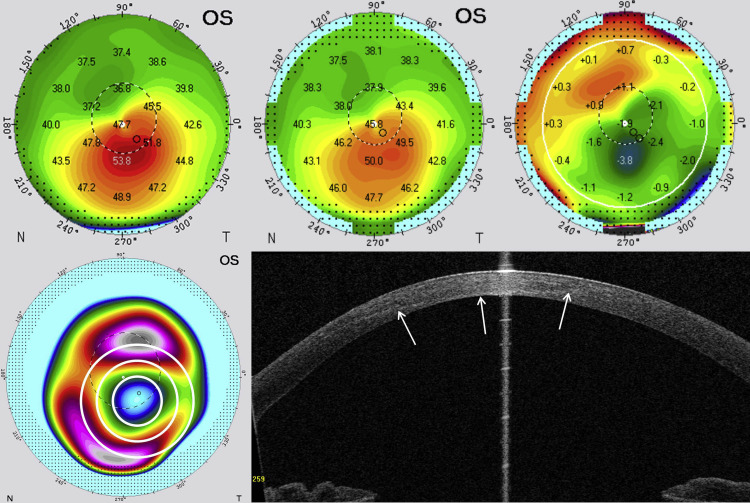
A typical example of the change in corneal tomography after customized CXL is depicted in Figure 1 , including the sagittal maps preoperatively and 1 year postoperatively and the treatment plan as an overlay in the posterior float map. The difference map shows steepening of 1.5 D in the previously flat areas and flattening of 3.8 D in the steep areas, resulting in an RI of 5.3 D. In contrast, an example of the control group is represented in Figure 2 with an RI of 2.8 D.
The maximal curvature, K max , decreased during the first year after CXL in both groups. In the customized CXL, K max decreased by −1.7 ± 2.0 D, significantly different from −0.9 ± 1.3 D in the standard CXL ( P = .03). The comparison of the tomographic changes is depicted in Table 2 . In addition, the distribution of K max decrease was different, as shown in Table 3 : only 2 out of 19 eyes (11%) in the standard group but 7 out of 19 eyes (37%) in the customized CXL group showed a flattening of 2 or more diopters ( P = .03, 1-sided significance). On the other hand, 1 eye of the customized CXL group showed progression in K max ( Figure 3 ), which needs special consideration because the steepening occurred outside the treatment area.
| Preoperative Customized CXL | 1-Year Follow-up Customized CXL | P Value Customized CXL | Preoperative Standard CXL | 1-Year Follow-up Standard CXL | P Value Standard CXL | |
|---|---|---|---|---|---|---|
| Thinnest pachymetry (μm) | 463 ± 42 | 446 ± 44 | .0002* | 447 ± 35 | 429 ± 46 | .006* |
| K max (D) | 57.0 ± 6.7 | 55.4 ± 7.5 | .001* | 55.2 ± 5.3 | 54.4 ± 4.5 | .004* |
| BSCVA (logMAR) | 0.31 ± 0.26 | 0.24 ± 0.2 | .08 | 0.35 ± 0.32 | 0.31 ± 0.32 | .31 |
| Maximum posterior float (μm) | 72 ± 35 | 73 ± 36 | .20 | 65 ± 23 | 70 ± 28 | .02* |
| Endothelial cell count (cells/mm 2 ) | 2824 ± 256 | 2861 ± 197 | .47 | 2899 ± 277 | 2883 ± 299 | .73 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


