Purpose
To identify optic nerve head (ONH) cupping reversal and associated optical coherence tomography (OCT) and Humphrey visual field changes in pediatric glaucoma.
Design
Retrospective observational case series.
Methods
Sequential surgical cases of juvenile open-angle glaucoma (OAG) or primary congenital glaucoma (PCG) with sustained postoperative intraocular pressure (IOP) reduction. Group 1 had preoperative and postoperative ONH photographs and OCT; Group 2 had preoperative clinical ONH assessment and postoperative imaging. Cupping evaluation was confirmed by masked glaucoma and neuro-ophthalmology specialists.
Results
Of 80 cases, 9 eyes (9 children) met criteria for Group 1; 24 eyes (19 children) met criteria for Group 2. Group 1: Five of 9 eyes (56%) demonstrated cupping reversal, with preoperative vs postoperative mean IOP 34.2 ± 6.6 mm Hg vs 10.6 ± 4.1 mm Hg ( P < .00001) and mean average retinal nerve fiber layer (RNFL) 71.0 ± 30 μm vs 62.8 ± 24 μm ( P = .4), respectively. RNFL was stable in 4 of 5 eyes (all juvenile OAG), but thinned (Δ = −41 μm) in 1 eye with PCG. Humphrey visual fields (reliable in 2 of 3 eyes) showed no significant change. Group 2: Fourteen of 24 PCG eyes (58%) demonstrated cupping reversal, with preoperative vs postoperative mean IOP 36.1 ± 8.9 mm Hg vs 13.3 ± 2.1 mm Hg ( P < .00001). Two eyes had thin RNFL postoperatively despite healthy-appearing ONH. Postoperative RNFL showed statistically significant linear correlation with preoperative (but not postoperative) cup-to-disc ratio. Limitations include small numbers, few reliable Humphrey visual fields, and absent preoperative imaging (Group 2).
Conclusion
Some eyes with IOP reduction and ONH cupping reversal show continued RNFL thinning postoperatively. The preoperative ONH cup-to-disc ratio predicted the postoperative RNFL better than the postoperative “reversed and smaller” cup-to-disc ratio. Cupping reversal in pediatric glaucoma may not predict improved ONH health and deserves further study.
Optic nerve head (ONH) cupping reversal—the improvement of optic disc appearance after marked intraocular pressure (IOP) reduction—has generally been considered an indicator of successful treatment in pediatric glaucoma. Multiple theories have been proposed to explain this phenomenon, including anterior movement of the lamina cribrosa, rebound shrinkage of the elastic neonatal scleral canal, hypertrophy and/or proliferation of glial cells, and increase in retinal nerve fiber layer (RNFL) height. Since age-dependent elasticity of scleral tissue is the basis for many of these theories, pressure-induced posterior bowing of the lamina cribrosa and/or outward displacement of the scleral canal may have a higher tendency to rebound anteriorly after substantial IOP reduction in younger eyes. Multiple studies in both human and primate glaucoma models have confirmed the higher incidence of cupping reversal in younger eyes. The functional significance of this phenomenon, however, remains unknown. In 1995, using a monkey model, Burgoyne and associates aimed to determine a relationship between optic disc compliance and axonal loss; their data supported the premise that despite the presence of a hyper-compliant disc, moderate axonal loss may have already occurred at the initial rise in IOP.
Although cupping reversal is more commonly seen after IOP reduction in children than in adults, it has been more thoroughly studied in the latter group, including the use of stereoscopic ONH photographs, confocal scanning laser ophthalmoscopy, and optical coherence tomography (OCT) of the peripapillary RNFL. Among the few studies using an objective means of evaluating ONH cupping reversal in pediatric glaucoma, a single case report used OCT imaging.
OCT imaging of the peripapillary RNFL may further elucidate the above theories of ONH cupping reversal: if RNFL height is normal, rebound elasticity of the ocular tissues seems more likely; however, if RNFL height is decreased, at least some proliferation of nonfunctioning glial tissue may be present. Longitudinal clinical data in adults with cupping reversal have been conflicting as to whether or not ONH cupping reversal is a true indicator of reversal of optic nerve functional damage, as seen on visual field testing. In children, however, where ONH cupping reversal is more prevalent, there are no data on the functional status of this phenomenon.
Our study is a retrospective analysis of both ONH cupping reversal in juvenile open-angle glaucoma (juvenile OAG) cases (where pre- and postintervention studies are more easily obtained) and primary congenital glaucoma (PCG) cases (where ONH cupping reversal is perhaps more readily seen). We hypothesize that ONH cupping reversal after surgical IOP reduction in pediatric glaucoma does not uniformly indicate minimal original ONH glaucomatous damage. The purpose of our study was to investigate a possible correlation between ONH cupping reversal after sustained IOP reduction in children with glaucoma and the corresponding status of the RNFL and, when possible, visual fields in these eyes.
Subjects and Methods
Subjects for this study were selected by chart review, from consecutive glaucoma surgical procedures, for all children (aged 2 months to 18 years) with juvenile OAG or PCG operated by 1 pediatric glaucoma specialist (S.F.F.) between August 26, 1997 and May 28, 2013. Only children previously diagnosed with juvenile OAG or PCG meeting eligibility requirements were included in the study. Juvenile OAG was defined as elevated IOP (>21 mm Hg) in an otherwise anatomically normal eye associated with definite glaucomatous optic nerve damage, as determined by a single clinician (S.F.F.). PCG was defined as enlarged corneal diameter with Haab striae and/or corneal edema, with or without abnormal ONH cupping or elevated IOP, and in the absence of any other ocular anatomic abnormalities to suggest a different etiology for glaucoma (eg, aniridia, Axenfeld-Rieger, post cataract removal, or secondary to trauma, uveitis, or other primary insult). This study was approved by the Institutional Review Board of Duke University Medical Center and is in accord with all Health Insurance Portability and Accountability Act (HIPAA) regulations. The included subjects were also enrolled as part of a larger database of pediatric glaucoma having OCT imaging. For the purposes of this study, “sustained IOP reduction” was defined as IOP reduced >30% from preoperative measurement, and “controlled glaucoma” was defined as IOP ≤21 mm Hg with or without IOP-reducing medication and considered clinically adequate for the status of the optic nerve and glaucoma severity.
To simplify data analysis, we divided the study eyes into 2 groups, based on whether or not preoperative ONH imaging was available. Hence, the first study group (Group 1) included children with either juvenile OAG or PCG, for whom at least 1 eye met all the following inclusion criteria: (1) documented glaucoma surgical procedure that produced sustained IOP reduction for >4 months after surgery; (2) controlled glaucoma; (3) reliable preoperative and postoperative OCT imaging of the peripapillary RNFL (and macula), with postoperative imaging taken within 24 months after surgery; (4) preoperative and postoperative stereoscopic ONH photographs, with postoperative photographs taken at the time of the postoperative OCT; and (5) pre- and postoperative Humphrey visual fields (when available and reliable) taken within 24 months after surgery.
Stereoscopic ONH photographs from pre- and postoperative imaging sessions were reviewed by 2 graders (a pediatric glaucoma specialist and a pediatric neuro-ophthalmologist) who were masked to the clinical information, as well as to which images were preoperative vs postoperative. Graders determined both a vertical and horizontal cup-to-disc ratio for each stereoscopic image, as well as any other notable features of the ONH they observed. ONH cupping reversal was determined to be present or absent by a third investigator based on the graders’ evaluation, and was defined as ONH cup/disc decline of ≥0.2 in either the vertical or horizontal plane and/or decrease in focal rim narrowing. Other characteristics (including pallor and peripapillary atrophy or disc tilting) reported by the graders were also recorded. The 2 graders were allowed to come to consensus when there was a disagreement.
The second group (Group 2) included children with PCG and subjective clinical documentation of ONH cupping (but no photographic documentation or OCT imaging) prior to glaucoma surgical intervention in either 1 or both eyes, who met similar postoperative inclusion criteria to those described above for the first group. The inclusion criteria were as follows: (1) PCG with clinician-documented (by S.F.F.) ONH characteristics and cupping performed during a clinic visit or examination under anesthesia before glaucoma surgery; (2) documented glaucoma surgical procedure producing sustained IOP reduction for >12 months after surgery; (3) controlled glaucoma (note that this definition allowed for completion of a planned second goniosurgery within 2 months of the first surgery); (4) postoperative OCT imaging taken 12–120 months postoperatively (with IOP continuously controlled); and (5) postoperative stereoscopic ONH photographs taken within 24 months of the postoperative OCT. ONH cupping reversal was similarly determined by comparing the chart-documented ONH cup-to-disc ratio vs masked review of postoperative stereoscopic optic nerve photographs as for Group 1.
Exclusion criteria for both groups included history of premature birth (<36 weeks gestational age) and congenital optic nerve anomalies or other neurologic diagnoses that could affect optic nerve appearance (including history of hydrocephalus, cerebral ischemia, optic pathway pathologies).
Data were collected from chart review on all study subjects, including: (1) age at glaucoma diagnosis; (2) age at surgical intervention; (3) optotype visual acuity preoperative (when available) and postoperative (Snellen visual acuity testing preferred, but when unable, HOTV linear/crowding bars was standardly used); (4) cycloplegic refraction, postoperative, recorded as spherical equivalent; (5) central corneal thickness, when available, measured by handheld contact pachymeter (Pachmate DGH55; DGH Technology Inc, Exton, Pennsylvania, USA in clinic and Pachette; DGH Technology Inc during examinations under anesthesia); (6) axial length (by immersion, ultrasound) immediately before surgery, if available, and again at the next examination under anesthesia (within 1 year); (7) IOP prior to surgical intervention; (8) IOP measurement at least 30 days after surgical intervention, with all IOP measurements recorded, preferably in clinic, using Goldmann applanation tonometry (when available), Icare (Icare TAO1i; Icare Finland Oy, Finland), or Tono-pen (Tono-pen XL; Medtronic Solan, Jacksonville, Florida, USA) for smaller children; and using Tono-pen XL when taken during an examination under anesthesia; (9) additional sequential IOP measurements (and number of glaucoma medications) at scheduled clinic visits and scheduled examinations under anesthesia after surgical intervention up until the time of the postoperative assessments (OCT, stereoscopic ONH photographs, and/or Humphrey visual field testing), whichever came last; and (10) date and quality of all ONH photographs taken before and after the surgical intervention.
For OCT images, additional data were collected, including date, reliability indices, and peripapillary RNFL for all images taken before and/or after the surgical intervention using Stratus time-domain (TD) OCT (OCT-3; Carl Zeiss Meditec, Dublin, California, USA) and—when available—Spectralis spectral-domain (SD) OCT (software V.5.1.3.0; Heidelberg Engineering, Dossenheim, Germany) for the Group 1 eyes, and SD OCT only for the Group 2 eyes. All SD OCT RNFL scans were reviewed for plotting errors by a trained OCT reader masked to ONH status (M.A.E.), and, when present, the plotting lines were adjusted using the edit mode of the Spectralis review software. When comparing 2 OCT scans of the same eye, a change in average RNFL thickness of ≥10 μm was considered significant and a change of <10 μm was considered to be stable. Charts were reviewed for date, reliability indices, mean deviation (MD), and pattern standard deviation (PSD) for all Humphrey visual fields (24-2, threshold testing) (Carl Zeiss Meditec) taken before and/or after the surgical intervention.
For analysis of data, eligible eyes (1 or both) of each subject were included. Subject characteristics were tabulated with the use of number and percent for categorical data, and with the use of mean, median, range, and standard deviation (SD) for continuous variables. Comparisons of pre- vs postoperative cup-to-disc and OCT values were performed by paired t test and Wilcoxon rank-sum testing when appropriate. All statistical tests were 2-sided and the threshold for significance was set at α = 0.05. All values are reported as mean ± SD unless otherwise noted. Linear regression was performed when appropriate. Software used included Microsoft Excel (Microsoft Corporation; 2007), JMP Pro11.0.0 (SAS Institute Inc, Cary, North Carolina, USA; 2013) and Graphpad prism 6 (Graphpad Software, San Diego, California, USA; 2014).
Results
Characteristics of Group 1 Versus Group 2 Eyes (and Children)
Overall, children in Group 1 were older than those in Group 2 at both diagnosis (11.7 ± 4.6 years [median 12, range 4–18] vs 8 ± 7.4 months [median 5, range 1–24], P < .0001, respectively) and surgery (12.4 ± 4.6 years [median 13, range 5–18] vs 22 ± 35 months [median 7, range 2–135], P < .0001, respectively). Group 1 eyes were almost entirely juvenile OAG (8/9) while Group 2 eyes were solely PCG.
Group 1 (Both Preoperative and Postoperative Photographs and Optical Coherence Tomography Available)
After chart review of 80 consecutive children having glaucoma surgery (juvenile OAG or PCG), 8 of 17 total juvenile OAG subjects and 1 of 63 total PCG subjects (total 9 eyes of 9 children) met all eligibility requirements. The subjects included 4 white, 2 black, and 3 other (1 Asian, 1 Indian, 1 Hispanic) ethnicities. The male-to-female ratio was 5:4, with mean age 11.7 ± 4.6 years (median 12, range 4–18) at diagnosis and 12.4 ± 4.6 years (median 13, range 5–18) at surgery. Median visual acuity pre- and postoperatively was 20/20 (range 20/20–4/200). Only 1 eye had documented loss of vision (from 20/20 to 20/70) after surgery ( Table 1 , Subject 18); this eye had tenuous central fixation attributable to advanced ONH damage and visual field loss. Median postoperative refractive error (spherical equivalent) was −2.00 diopters (range plano to −8.00), with 3 of 9 eyes (33%) having spherical equivalent ≥−6.00 diopters. Median postoperative central corneal thickness was 547 μm (range 495–605). Mean IOP preoperative vs postoperative for all Group 1 eyes was 34.2 ± 6.6 mm Hg vs 10.6 ± 4.1 mm Hg ( P < .0001) with mean duration of IOP reduction 12.2 ± 7.3 months before postoperative testing.
| Subject | Eye | Glaucoma Diagnosis | Surgery | IOP (mm Hg) | Mean Cup:Disc a | ONH Description | Mean RNFL Thickness (μm) | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Post b | Pre | Post | Post | Pre | Post | ||||
| With ONH Cupping Reversal | ||||||||||
| 1 | OS | Juvenile OAG | Trabeculotomy | 40 | 10.5 | 0.9 | 0.85 | Temporal and nasal pallor, thicker nasal rim, c notch 5 o’clock | 51 | 48 |
| 2 | OD | Juvenile OAG | Mitomycin C Trabeculectomy | 36 | 9.5 | 0.9 | 0.68 | Temporal pallor | 54 | 54 |
| 3 | OD | Juvenile OAG | Mitomycin C Trabeculectomy | 39 | 7.5 | 0.9 | 0.75 | Total pallor, thicker nasal rim c | 43 d | 51 d |
| 5 e | OS | PCG | Mitomycin C Trabeculectomy | 30 | 4 | 0.9 | 0.7 | 98 d | 56 d | |
| 4 | OS | Juvenile OAG | Goniotomy | 30 | 14 | 0.83 | 0.58 | 109 d | 105 d | |
| Overall | 34 | 11 | 0.89 | 0.71 | 71 | 63 | ||||
| Without ONH Cupping Reversal | ||||||||||
| 17 | OS | Juvenile OAG | Trabeculotomy | 32 | 16 | 1 | 1 | 37 | 33 | |
| 18 | OD | Juvenile OAG | Mitomycin C Trabeculectomy | 21 | 7 | 1 | 1 | Total pallor | 29 | 33 |
| 10 e | OS | Juvenile OAG | Trabeculotomy | 42 | 16 | 0.95 | 0.83 | 101 d | 62 d | |
| 25 | OS | Juvenile OAG | Trabeculotomy | 38 | 11 | 0.35 | 0.35 | 85 d | 88 d | |
| Overall | 33 | 13 | 0.83 | 0.79 | 63 | 54 | ||||
a Cup:disc = optic nerve head cup-to-disc ratio.
b Post (IOP) = median IOP from >30 days after surgery until the time of the first postoperative imaging.
c Comparison of preoperative photograph assessment and postoperative photograph assessment indicated a significant change in rim thickness in Subjects 1 (OS) and 3 (OD).
d Denotes those peripapillary RNFL thicknesses determined by Stratus optical coherence tomography (OCT) imaging; all others determined by Spectralis OCT imaging.
e Note decrease in RNFL after surgical IOP reduction in eyes of Subjects 5 (OS) and 10 (OS).
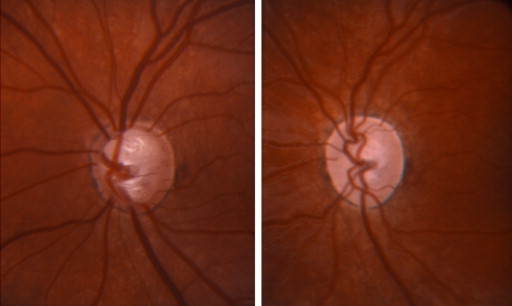
ONH cupping reversal was identified in 5 of 9 included eyes (4/8 juvenile OAG and 1 PCG, Figure 1 ). The remaining 4 eyes (all juvenile OAG) did not show ONH cupping reversal ( Table 1 ). There was a trend, but no statistically significant difference, in the mean age at glaucoma diagnosis for children with vs without ONH cupping reversal (10.5 ± 2.4 years vs 14.8 ± 4.0 years [median 9 vs 10 years], respectively, P = .07); the same held true for mean age at surgery for children with vs without ONH cupping reversal (11.3 ± 2.1 years vs 15.5 ± 4.4 years [median 16.5 vs 17.5 years], respectively, P = .1). Mean IOP for the eyes with vs without ONH cupping reversal was similar preoperatively (34.2 ± 6.6 mm Hg vs 33.3 ± 9.1 mm Hg, respectively, P = 1) as well as postoperatively (10.6 ± 4.1 mm Hg vs 12.5 ± 4.4 mm Hg, respectively, P = .2), P < .001 preoperative vs postoperative IOP for each respective subset. Mean duration of IOP reduction between surgery and postoperative imaging for eyes with vs without ONH cupping reversal was 9.6 ± 5.1 months vs 15.5 ± 5.1 months, respectively, P = .35. Mean duration of IOP reduction between pre- and postoperative imaging for eyes with vs without ONH cupping reversal was 14.0 ± 8.9 months vs 17.8 ± 11.3 months, respectively, P = .6. At the time of postoperative imaging, eyes with vs without ONH cupping reversal were on a similar number of topical glaucoma medications (1.4 ± 1.9 vs 1.8 ± 1.3, respectively, P = .9).
For the 5 eyes that did show ONH cupping reversal, the average pre- vs post-ONH cup-to-disc ratio was 0.89 ± 0.03 vs 0.71 ± 0.10 ( P = .008). Mean average peripapillary RNFL preoperatively vs postoperatively was 71.0 ± 30 μm vs 62.8 ± 24 μm ( P = .5). RNFL was stable in 4 of 5 eyes with ONH cupping reversal (all juvenile OAG), but thinned (ΔRNFL = −41 μm) in 1 of 5 eyes (the only PCG subject, Table 1 ). There was also a decline in total macular volume before vs after surgery in this eye (6.81 mm 3 vs 6.46 mm 3 ). Three of the 5 eyes had pre- and postoperative Humphrey visual field testing; however, only 2 of 3 were reliable (Subjects 2 and 4, Table 1 ). In these 2 eyes, there was no clinically significant difference noted in pre- and postoperative testing (MD, PSD, or scotoma; data not shown).
For the 4 eyes (all juvenile OAG) that did not show ONH cupping reversal, the average pre- vs postoperative ONH cup-to-disc ratio was 0.83 ± 0.32 vs 0.79 ± 0.31 ( P = .3). Mean average peripapillary RNFL preoperatively vs postoperatively was 63.2 ± 36 μm vs 53.9 ± 24 μm ( P = .5). RNFL was stable in 3 of 4 eyes without ONH cupping reversal but thinned (ΔRNFL = −39 μm) in 1 of 4 eyes. There was no reliable presurgical macular OCT scan for comparison in this 1 eye. Three out of 4 eyes had pre- and postsurgical Humphrey visual field testing. Only 1 out of the 3 had reliable testing and showed no clinically significant change from pre- to postoperative tests (Subject 25, Table 1 ).
Neither the preoperative nor the postoperative mean RNFL showed a statistical difference for those eyes that did show reversal of ONH cupping vs those that did not show reversal ( P = .46 for preoperative, P = .62 for postoperative comparison, respectively).
Group 2 (Preoperative Imaging Not Available Owing to Corneal Clouding and Young Age)
In Group 2, 19 of 63 total reviewed PCG cases (30%) were found to meet the eligibility requirements (total 24 eyes of 19 children). The children included 8 white, 9 black, and 2 other (1 Asian, 1 Hispanic) ethnicities. The male-to-female ratio was 5:7. The mean age at diagnosis was 8 ± 7.4 months (median 5, range 1–24) and at surgery was 22 ± 35 months (median 7, range 2–135; the delay often included completion of planned 2-stage angle surgery), respectively ( Table 2 ). The median visual acuity postoperatively was 20/30 (range 20/20–20/400). The most common cause of visual impairment in this group was amblyopia secondary to corneal scarring (17 of 24 eyes had documented Haab striae). The median postoperative refractive error (spherical equivalent) was −0.31 diopters (range +0.50 to −10.50), with 2 of 24 eyes (8.3%) ≥−6.00 diopters. Median postoperative central corneal thickness (available in 14 of 24 eyes) was 508 μm (range 387–589). Mean IOP preoperatively vs postoperatively was 37.3 ± 8.1 mm Hg vs 13.2 ± 2.8 mm Hg ( P < .00001), with a mean duration of IOP reduction before postoperative testing of 66 ± 31 months. Preoperative vs postoperative mean axial length—23.27 vs 22.88 mm, respectively—was available in 14 of 24 eyes (58%), but was not significantly changed ( P = .6) after a mean interval of 1 ± 2 months.
| Subject | Eye | Surgery | IOP (mm Hg) | Mean Cup:Disc a | ONH Description | Mean RNFL Thickness (μm) | ||
|---|---|---|---|---|---|---|---|---|
| Pre | Post b | Pre | Post | Post | Post | |||
| With ONH Cupping Reversal | ||||||||
| 8 | OD | Goniotomy | 33 | 11 | 1 | 0.78 | 34 | |
| 8 | OS | Goniotomy | 29 | 11 | 1 | 0.83 | Total pallor | 36 |
| 7 | OS | Ahmed | 38 | 15 | 1 | 0.68 | Notch 5 o’clock | 37 |
| 9 c | OS | Mitomycin C Trabeculectomy | 43 | 9 | 0.75 | 0.43 | Temporal pallor, notch 12 o’clock | 68 |
| 15 c | OD | Goniotomy | 56 | 16 | 0.38 | 0 | 70 | |
| 14 | OD | Goniotomy | 44 | 12 | 0.55 | 0.38 | 99 | |
| 16 | OS | Goniotomy | 47 | 12 | 0.35 | 0 | 100 | |
| 13 | OS | Goniotomy | 34 | 14 | 0.5 | 0.35 | 102 | |
| 12 | OD | Goniotomy | 24 | 13 | 0.6 | 0.3 | 106 | |
| 6 | OD | Goniotomy | 39 | 15 | 0.63 | 0.15 | 106 | |
| 12 | OS | Goniotomy | 29 | 13 | 0.6 | 0.38 | 108 | |
| 13 | OD | Goniotomy | 31 | 15 | 0.6 | 0.5 | 114 | |
| 10 | OD | Goniotomy | 30 | 16.5 | 0.75 | 0.45 | 123 | |
| 11 | OD | Goniotomy | 28 | 14 | 0.65 | 0.45 | 126 | |
| Overall | 36 | 13 | 0.67 | 0.40 | 88 | |||
| No ONH Cupping Reversal | ||||||||
| 19 | OS | Mitomycin C Trabeculectomy | 40 | 4 | 1 | 1 | Total pallor | 28 |
| 7 | OD | Ahmed | 40 | 12 | 0.8 | 1 | Total pallor | 42 |
| 23 | OS | Goniotomy | 39 | 18 | 0.6 | 0.83 | Notch 6 o’clock | 57 |
| 21 | OD | Baerveldt | 31 | 15 | 0.88 | 0.85 | Notch 7 o’clock | 75 |
| 22 | OD | Goniotomy | 28 | 11.5 | 0.6 | 0.75 | 76 | |
| 5 | OD | Goniotomy | 36 | 12 | 0.75 | 0.68 | 86 | |
| 24 | OD | Goniotomy | 40 | 14.5 | 0.5 | 0.73 | 87 | |
| 26 | OS | Goniotomy | 37 | 14.5 | 0.38 | 0.25 | 90 | |
| 27 | OD | Goniotomy | 49 | 14 | 0.35 | 0.4 | 91 | |
| 27 | OS | Goniotomy | 51 | 14 | 0.3 | 0.25 | 96 | |
| Overall | 39 | 13 | 0.62 | 0.67 | 73 | |||
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


