

Thus, as clinicians we consider cough as a manifestation of disease; yet, as scientists, we think of cough as a product of physiologic mechanisms. These diseases and mechanisms involve the spectrum of adult medical and pediatric disciplines, including otolaryngology, pulmonology and chest physicians, allergy and immunology, gastroenterology, neurology, cardiology, infectious disease, speech and swallowing pathologists, as well as psychiatry. It is particularly timely for this discussion of cough as a true interdisciplinary problem, since we now consider both “macrophysiologic” (interplay of diseases) and “microphysiologic” perspectives (interplay of mechanisms).
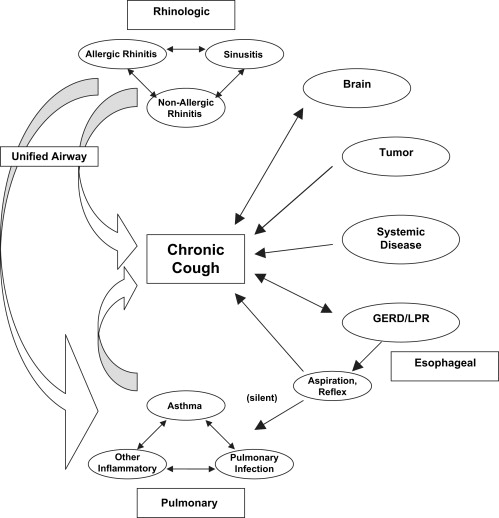
The list of diseases that may induce cough is growing, along with an appreciation of the inter-relatedness of these diseases, as described in Fig. 1 . For example, emerging evidence now supports our long-held observation that the upper and lower airway diseases are closely related as an unified airway, and that allergy plays an important role in exacerbating both upper and lower airway disease. There is also a spectrum of both asthmatic and non-asthmatic lower airway inflammatory disease that often has overlapping clinical signs. Asthmatic, allergic, infectious and other irritant and inflammatory processes in the nose and lung similarly have complex and synergistic physiologic relationships.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


