The symptom of cough may result from a multitude of etiologies involving different parts of the aerodigestive tract. This article focuses on the association of cough and swallowing dysfunction in the sense that cough may be an indicator of swallow dysfunction and in the importance of cough in preventing aspiration and aspiration-related disorders. Whereas these associations have been known for a long time, research is starting to connect the dots, allowing targeting of strategies aimed at diagnosing and preventing illness in certain dysphagic patients.
The cough reflex is a highly developed and essential airway protective mechanism. The primary developmental obstacle for evolution from aquatic to earth subsistence was the ability to protect the lower airway from the incursion of liquid and food. Thus, in order of phylogenetic importance, the three functions of the larynx are airway protection, respiration, and phonation. Reflexive glottic closure has evolved into one of the primary methods of airway protection. Stimulation of peripheral afferents innervated by the internal branch of the superior laryngeal nerve (SLN) triggers the laryngeal adductor response (LAR). The LAR is a rapid stimulation of the thyroarytenoid muscles in response to ipsilateral SLN stimulus. Its purpose is to protect the airway from invading food and liquid from above. Bilateral stimulation of the SLN results in sphincteric closure of the glottis at three different levels: (1) aryepiglottic folds, (2) false vocal folds, and (3) true vocal folds.
The LAR can be measured clinically with laryngopharyngeal sensory testing. An air pulse stimulus can be administered to the laryngeal mucosa innervated by the SLN through a specialized endoscope and the magnitude of the stimulus necessary to elicit the LAR is measured. The importance of the LAR has been established. Individuals with dysphagia and an absent LAR aspirate thin liquid nearly 94% of the time in comparison to an aspiration rate of 17% for individuals with an intact LAR. Once a food or liquid bolus has penetrated the laryngeal defenses, the cough reflex provides the final protective mechanism to expel the invading material.
Viewed from a mechanical perspective, coughing involves several important coordinated actions ( Fig. 1 ). The initial phase typically involves inhalation. During this phase, the vocal folds are fully abducted, allowing for deep, rapid inflow of air. The second phase consists of forceful exhalation against a closed glottis. Maximal adduction of the vocal folds and contraction of the aryepiglottic folds results in sphincteric closure of the glottis and supraglottis. During this phase, pressure is built up in the subglottis. This pressure results in narrowing of the upper trachea to up to one-sixth of its normal diameter, allowing for airflow rates nearing the speed of sound through this segment. Structurally, the appearance of the larynx at this point is similar to that seen during the oropharyngeal phase of deglutition. However, the epiglottis is not retroverted, as the larynx remains in a low position. Additionally, the pressures generated at the glottic and subglottic levels are different during these two tasks. During swallowing, pressure generated at the glottic level from vocal cord closure is significantly higher than during cough. Conversely, subglottic pressure is much higher with a cough than with a swallow. The third phase of the cough involves violent ejection of the air from the lungs after release of the laryngeal muscles. This release of air allows for the expulsion of secretions, mucus, or foreign material from the tracheobronchial tree. Passage of the air produces sound through the vibration of mucosa along the trachea, larynx, and vocal tract.
The cough reflex arc is initiated in sensory nerve endings and receptors located in the respiratory epithelium throughout the tracheobronchial tree. There are a few receptor types that are believed to trigger the cough reflex: mechanoreceptors, nociceptors, and so-called cough receptors. Mechanoreceptors respond to mechanical stimuli. This may be due to pressure on the mucosa (as may occur with aspirating a piece of food) or stretching of the mucosa (as may occur in the lungs with bronchospasm). Nociceptors respond to irritant or proinflammatory chemicals such as capsaicin, bradykinin, and citric acid that come in contact with the mucosa. In addition to these two receptor types, recent evidence has supported the presence of a separate primary receptor called the cough receptor, which responds to punctuate mechanical stimuli, low chloride solutions, and acids. This last receptor type is believed to exist largely in the larynx and trachea.
Regardless of the trigger, the suprathreshold stimulation of the respiratory mucosa results in an afferent signal, which ultimately results in the cough sequence. The reflex arc involves afferent neurons traveling in the vagus nerve, which converge on the cough center, located in the medulla at the nucleus tractus solitarius. These neurons directly trigger efferent neurons, which bilaterally innervate the laryngeal adductor muscles (from the nucleus ambiguus via the vagus nerve), intercostal muscles, abdominal wall, diaphragm, and pelvic floor (in the cervical and thoracic spinal cord via phrenic and spinal motor nerves).
Here, there are overlaps with the swallowing sequence. The same afferent and efferent pathways used for coughing are used for a swallowing sequence. The different outcome (cough versus swallow) may be due to a difference in the initial trigger (food bolus in the oropharynx versus direct stimulation of the laryngeal mucosa) or different signaling based on the sensory receptors or afferent nerves. Additionally, though the neural anatomy is similar, there may be some important differences in the functional aspect of the signaling pathways. A recent article that examined the role of the internal branch of the superior laryngeal nerve found that blockade of this nerve alters laryngeal closure during swallowing, but does not affect voluntary closure during cough. Jafari and colleagues concluded that this nerve might be involved in providing feedback to central neural pathways involved in laryngeal closure during the pharyngeal phase of swallowing.
Laryngeal closure is an important component of the cough reflex. Closure allows for buildup and release of subglottic pressure. The inability to close the glottis or supraglottis, as occurs with vocal fold paralysis, may result in a weak or ineffective cough, allowing secretions to accumulate in the trachea and lower airways, especially in otherwise weak or compromised patients. In addition, the presence of vocal fold paralysis in a patient has been found to increase the incidence of aspiration by 15% when compared with other patients referred for dysphagia evaluation. This can be a critical issue, especially in patients with compromised pulmonary function. Improving glottal closure, therefore, is an important consideration in preventing aspiration, restoring pulmonary function, and preventing deterioration.
Glottal insufficiency is typically addressed by vocal fold injection augmentation or laryngeal framework surgery. Both of these interventions aim to statically move the vocal fold toward the midline to allow for glottal closure. Whereas such procedures are commonly performed and successful outcomes have been reported, there is, as yet, no large-scale, carefully performed study demonstrating benefit from glottal closure procedures alone for dysphagia resulting from unilateral vocal fold paralysis or paresis.
Cough and dysphagia
Cough is a brainstem-mediated, protective mechanism that functions, in part, to evict aspirated food and liquid from the lower respiratory tract. Oropharyngeal dysphagia with associated laryngeal penetration or aspiration should, therefore, be included in the differential diagnosis of persons with chronic cough. Symptoms and findings that suggest that the cough is associated with penetration or aspiration include increased cough with thin—as opposed to thick—liquids, a history of stroke or progressive neurologic disease, a history of oropharyngeal dysphagia, a history of head and neck cancer or head and neck surgery, the presence of a wet vocal quality, hoarseness, and coughing with meals as opposed to after meals. Postcibal cough is typically a sign of gastroesophageal or esophagopharyngeal reflux. Some patients with a hypersensitive larynx also report coughing with meals and it is important to differentiate persons with a hypersensitive larynx from persons with oropharyngeal dysphagia who are at risk for aspiration. Alternative names for the hypersensitive larynx include vocal cord dysfunction and paradoxic vocal fold motion impairment. Patients with a hypersensitive larynx often report dyspnea or stridor with inspiration, excessive throat clearing, disproportionate throat mucus, neck tightness, intermittent dysphonia, and cough with spicy foods, vinegar, second hand tobacco, and perfumes. They are frequently diagnosed with asthma but fail treatment with inhaled corticosteroids and beta-agonists. The disorder is more prevalent in young overachieving female athletes. Cough attributable to vocal cord dysfunction is successfully treated with respiratory retraining. The goal of respiratory retraining is to create a rhythmic pattern by focusing on breathing with minimal expiratory force. If the history suggests that cough may be due to laryngeal penetration or tracheal aspiration, a diagnostic workup is indicated.
Fundamentals of swallow assessment
The oropharyngeal stage of swallowing may be evaluated by a clinical bedside assessment, endoscopy, or fluoroscopy. The bedside swallow evaluation involves administering a patient ice chips, water, or food and monitoring for cough, wet vocal quality, or voice change. Cervical auscultation and pulse oximetry may be added to increase diagnostic sensitivity. The predictive value of the bedside swallow evaluation is limited, however. Recent research has focused on improving the accuracy of bedside examinations. The assessment of voluntary cough strength (through measures of airflow dynamics) appears to demonstrate promise in improving sensitivity and specificity for the identification of aspirators.
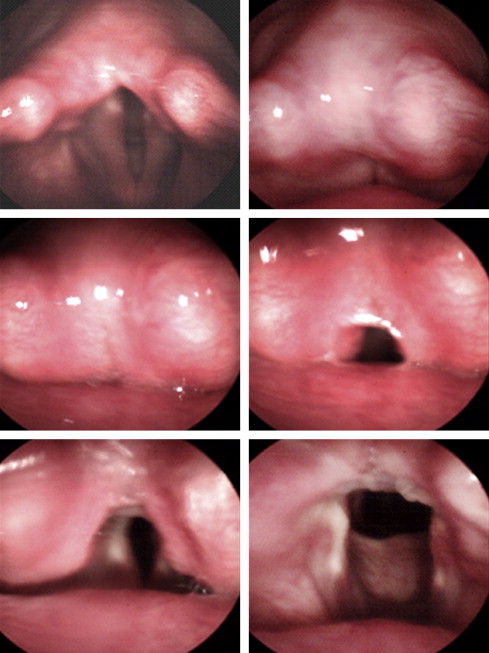
The gold standard swallowing assessment, however, has traditionally been the videofluoroscopic swallow evaluation (VSE) or modified barium swallow. The VSE involves administering the patient barium sulfate under real-time fluoroscopic video recording. The rheology of the barium may be manipulated to test for aspiration with thin liquid or a variety of different viscosities. Aspiration with solid food can also be evaluated by adding barium to paste, puree, and solid food consistencies. The degree of laryngeal penetration and aspiration can be quantified with a validated penetration and aspiration scale (PAS). Cough during the study is easily visualized and its association with aspiration is noted. An alternative to the VSE is the flexible endoscopic evaluation of swallowing or FEES. If the LAR is assessed with an air pulse stimulator during the FEES, the examination is referred to as a flexible endoscopic evaluation of swallowing with sensory testing or FEESST. A FEES and FEESST are performed in an unsedated patient sitting upright in an examination chair. A small caliber endoscope is passed through the nasal cavity and positioned in the pharynx above the tip of the epiglottis ( Fig. 2 ). The entire examination is recorded for later slow-motion playback. The larynx is evaluated for lesions, masses, and edema. Pooling of saliva is a major risk factor for swallowing impairment, and aspiration and its presence in the pyriform sinuses is noted ( Fig. 3 ). Vocal fold mobility is evaluated by having the patient perform the “eee-sniff maneuver.” Having the patient say “eee” maximally adducts and sniffing maximally abducts the vocal folds. The presence of glottal insufficiency is a major risk factor for aspiration. Nearly one quarter of patients with a paralyzed vocal fold will aspirate. Laryngeal sensation is assessed with elicitation of the LAR with an air pulse stimulator or with the tip of the laryngoscope placed onto the aryepiglottic fold. An absent LAR is a significant risk factor for aspiration.




