Purpose
To evaluate the correlation of retrobulbar volume change, resected orbital fat volume, and proptosis reduction after fatty decompression.
Design
Cross-sectional and prospective study.
Methods
Twenty-two patients (44 orbits) with Graves ophthalmopathy underwent fatty decompression. Preoperative orbital computed tomography (CT) imaging with a 2-mm cut was compared with postoperative imaging carried out 6 months after fatty decompression. The relationship of retrobulbar volume change, resected orbital fat volume, and proptosis reduction was analyzed by Pearson correlation. Linear regression was performed using resected fat volume or proptosis reduction as independent variables and retrobulbar volume change as a dependent variable to validate the effect of fatty decompression.
Results
Mean proptosis reduction was 4.1 ± 0.9 mm. Mean volume of resected orbital fat was 4.4 ± 1.2 mL. Mean retrobulbar volume change in computed tomographic imaging was 3.2 ± 1.0 cm 3 . The change in retrobulbar volume was correlated strongly with proptosis reduction and volume of resected orbital fat. Linear regression revealed the following equation for Retrobulbar volume change: 0.546 × Hertel change + 0.945 or 0.293 × Volume of resected orbital fat + 1.917.
Conclusions
Fatty decompression can reduce proptosis for patients with disfiguring Graves ophthalmopathy. Because of the close correlation of retrobulbar volume change with volume of resected orbital fat and proptosis reduction, we propose that orbital fat removal may be accompanied by decreased retrobulbar volume after fatty decompression. Evidence of decreased retrobulbar volume may result in effective proptosis reduction.
Although the technique of orbital decompression continues to evolve, postoperative diplopia remains a significant complication in all such procedures. Inferomedial wall decompression, even when it leaves an intact strut of bone at the maxillary–ethmoidal junction, continues to carry a significant risk for consecutive diplopia and globe displacement. Previous reports indicated that extensive removal of orbital fat may reduce proptosis with few complications. It is increasingly popular for oculoplastic surgeons to remove orbital fat to rehabilitate patients with cosmetically disfiguring exophthalmos, exposure keratopathy, and even compressive optic neuropathy. The advantages of fatty decompression include preservation of the orbital wall and less surgically induced diplopia. In this study, we evaluated the correlation between the amount of orbital fat removed, retrobulbar volume change determined by computed tomography (CT) imaging, and proptosis reduction after fatty decompression.
Methods
Setting and Patients
This prospective cross-sectional study was conducted from January 2006 through January 2007 in the Thyroid Eye Disease Clinic at the National Taiwan University Hospital, Taipei, Taiwan. A total 44 orbits from 22 consecutive patients with Graves ophthalmopathy having self-described disfiguring exophthalmos (9 males, 13 females) were enrolled. The inclusion criteria for fatty decompression were euthyroid status for more than 3 months, having inactive status according to the clinical activity score, and stable Hertel exophthalmometry readings for more than 6 months. Local administrative and ethics committees approved all aspects of this study. Signed, informed consent to participate was obtained from all patients. Exclusion criteria included medical history of eyelid, orbital, or intraocular inflammation; prior orbital surgery; compressive optic neuropathy; or episodes of trauma other than Graves disease. CT imaging of most patients showed proptosis of the fat-predominant type. All patients received oral corticosteroids for 3 to 6 months without orbital irradiation before fatty decompression. All patients underwent fatty decompression via the transforniceal approach on 44 orbits performed by the same surgeon (S.-L.L.).
Surgical Technique and Evaluations
Fatty decompression was performed according to a previously described technique. Orbital fat was resected via a transforniceal swinging eyelid approach, and prolapsing orbital fat was resected from the orbital margin deep into the intraconal space. Special effort was made to remove intraconal fat. The desired volume (3 to 7 mL) of adipose tissue was removed.
Preoperative evaluation included visual acuity, Hertel exophthalmometry, direct biomicroscopic examination of the optic disc, intraocular pressure, fluorescein corneal staining, margin reflex distance for lid height, presence of strabismus, and range of extraocular muscle motility. Each patient underwent preoperative axial orbital CT imaging with 2 mm cuts. During surgery, the resected orbital fat was placed within a 10-mL syringe to measure the amount resected.
Postoperative evaluations were performed at 1 week and 1, 3, and 6 months after surgery. Hertel exophthalmometry was performed at each postoperative visit. Each patient underwent CT imaging with 2-mm cuts approximately 6 months after surgery. Retrobulbar orbital volume—defined as the extraocular orbital volume posterior to the equator of the globe—was calculated using computer-assisted digitized drawing software (Mirror, Canfield Clinical System; Canfield Scientific, Inc, Fairfield, New Jersey, USA). The surface area of each 2-mm cut orbital slice was calculated automatically by marking the margin of the retrobulbar orbital area using the Mirror software ( Figure 1 ). The retrobulbar orbital volume was approximated by summing up all surface areas of the retrobulbar space of each 2-mm cut CT image and multiplying by 0.2. By this means, the preoperative and postoperative retrobulbar volume change of CT imaging was determined.

Main Outcome Measures
Baseline characteristics were presented as mean and standard deviation (SD) for continuous variables and number and percentage for categorical variables. Bivariate correlation (Pearson correlation) was used to find the correlation of retrobulbar orbital volume change with the amount of resected orbital fat and the proptosis reduction (Hertel exophthalmometry change). Scatterplots were created to indicate patient variation in correlation coefficients of retrobulbar orbital volume change versus Hertel exophthalmometry change, retrobulbar volume change versus volume of resected orbital fat, and Hertel exophthalmometry change versus volume of resected orbital fat.
General linear regression was performed using the change in retrobulbar volume in the CT imaging as a dependent variable and the amount of resected orbital fat or proptosis reduction as independent variables to validate the effect of fatty decompression. SPSS software version 11.0 for Windows (SPSS, Inc, Chicago, Illinois, USA) was used for all statistical analyses, and the significance level ( P value) was set as .05.
Results
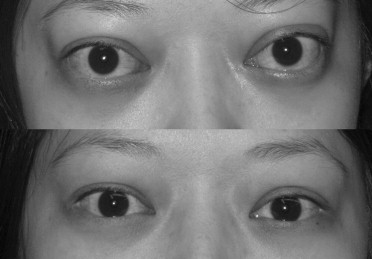
The mean age of patients was 37.9 ± 12.0 years; among the 22 patients, slightly more (n = 13) were female (59.1%; Table 1 ). The mean Hertel values before and after fatty decompression were 22.0 ± 1.8 mm and 17.9 ± 1.2 mm, respectively. The mean postoperative Hertel value change was 4.1 ± 0.9 mm (range, 2.0 to 6.0 mm; Figure 2 ). The average amount of resected orbital fat was 4.4 ± 1.2 mL (range, 1.8 to 9.0 mL). The mean retrobulbar orbital volume as measured by CT imaging before and after fatty decompression was 21.0 ± 3.3 cm 3 and 17.8 ± 3.0 cm 3 , respectively. The average postoperative retrobulbar orbital volume change of CT imaging was 3.2 ± 1.0 cm 3 (range, 1.8 to 5.7 cm 3 ). No postoperative massive retrobulbar hemorrhage, optic nerve damage, hypoglobus, or other cranial or sensory nerve damage was noted.
| Variable | Mean (Range) ± SD or Number (%) |
|---|---|
| Age (yrs) | 37.9 (21 to 60) ± 12.0 |
| Gender | |
| Female | 13 (59.1%) |
| Male | 9 (40.9%) |
| Preoperative Hertel value (mm) | 22.0 (18.0 to 25.0) ± 1.8 |
| Postoperative Hertel value (mm) | 17.9 (16.0 to 20.0) ± 1.2 |
| Hertel change (mm) | 4.1 (2.0 to 6.0) ± 0.9 |
| Volume of resected orbital fat (mL) | 4.4 (1.8 to 9.0) ± 1.2 |
| Preoperative retrobulbar volume of CT (cm 3 ) | 21.0 (14.7 to 26.5) ± 3.3 |
| Postoperative retrobulbar volume of CT (cm 3 ) | 17.8 (12.0 to 22.5) ± 3.0 |
| Retrobulbar volume change of CT (cm 3 ) | 3.2 (1.8 to 5.7) ± 1.0 |
We found a strong correlation in proptosis reduction (Hertel change), volume of resected orbital fat, and postoperative retrobulbar volume change in CT imaging, as shown in Table 2 . In addition, scatterplots of retrobulbar orbital volume change versus Hertel exophthalmometry change, retrobulbar volume change versus volume of resected orbital fat, and Hertel exophthalmometry change versus volume of resected orbital fat with correlation coefficients also showed strong correlation with individual patient variation ( Figures 3, 4, and 5 ).



