Purpose
To determine differences in riboflavin concentration in the anterior, intermediate, and posterior stroma after 3 corneal cross-linking imbibition techniques (standard epithelial [epi]-off, epi-on, and iontophoresis-assisted administration) of 0.1% riboflavin.
Design
Experimental laboratory investigation of human cadaver corneas not suitable for transplantation.
Methods
Ten corneas underwent imbibition with epi-on (n = 3), epi-off (n = 3), iontophoresis (n = 3), and saline exposure (control; n = 1). Femtosecond laser was used to produce 3 8-mm discs of the superficial (0-150 μm), intermediate (150-300 μm), and deep stroma (>300 μm). Riboflavin concentration was measured with high-performance liquid chromatography. The main outcome measure was riboflavin concentration at the 3 evaluated depths.
Results
The overall stromal concentration of riboflavin was 34.1 ± 7.1 μg/g in epi-off, 7.2 ± 3.7 μg/g in epi-on, and 15.0 ± 5.1 μg/g in iontophoresis. The mean riboflavin content in the superficial slice in the epi-off group was about 2-fold greater than that of the iontophoresis group (50.5 ± 5.3 μg/g and 23.6 ± 2.5 μg/g, respectively) and 4-fold greater than that of the epi-on group (11.7 ± 3.3 μg/g). Similar differences among the 3 groups were observed for the intermediate and posterior stromal slices, presenting an evident reduction of riboflavin concentration with increasing depth in all groups. Slice depth–dependent decrease in riboflavin concentration was statistically significant (general linear model (GLM); F1,6 = 62.265, P < .001), as was the group-dependent variation (GLM; F2,6 = 20.268, P = .002) and the slice depth group interaction (GLM; F2,6 = 18.004, P = .002).
Conclusions
Corneal cross-linking transepithelial iontophoresis imbibition yielded greater and deeper riboflavin saturation with respect to conventional epi-on, while maintaining the advantages of avoiding epithelial removal and shorter procedure time, but did not reach concentrations obtained with standard epi-off.
Keratoconus is a progressive corneal degenerative disorder in which a biomechanical weakness modifies the normal gradual curve into a more conical shape thus thinning the cornea. Substantial visual disturbance, ghost imaging, and decreased visual acuity ensue.
Corneal collagen cross-linking (CXL) is the only conservative treatment currently available to halt or reduce progression by improving the biomechanical rigidity of the corneal stroma. This technique consists of exposure to ultraviolet-A (UVA) irradiation at 370 nm, in the presence of stromal riboflavin (vitamin B2, a chromophore) and a UVA blocking agent. It combines the principles of chemical nonenzymatic CXL with the photo-oxidative CXL where riboflavin is the photosensitizer.
The basic principle behind CXL is that UVA excites the riboflavin in the corneal stroma to its triplet state, thus generating singlet oxygen species. These species can react with various other molecules, inducing the formation of covalent bonds that bridge the amino and carbonyl groups of collagen fibrils and proteoglycan core proteins. This process requires the presence of an adequate concentration of exogenously applied riboflavin to guarantee a sufficient amount of cross-linking while avoiding the absorption of UVA irradiation of deeper ocular tissue, such as the lens and retina, which could result in cellular damage.
Different techniques have been proposed to improve intrastromal penetration of riboflavin molecules. In the standard procedure (epithelial [epi]-off technique), the corneal epithelium is first removed and then drops of 0.1% riboflavin are administered at 1- to 5-minute intervals for 15-30 minutes before irradiation (30 minutes exposure to 370 nm UVA radiation at 3 mW/cm 2 ). Removal of epithelium allows riboflavin penetration, which is otherwise impeded by the epithelial cell tight junctions owing to its molecular weight.
Recently, several methods of transepithelial cross-linking were proposed to allow the penetration of riboflavin across the epithelium. In these procedures (epi-on techniques), removal of the epithelial layer is not necessary because chemical agents or enhancers, such as benzalkonium chloride, sodium ethylenediaminetetraacetic acid (EDTA), and tromethamine, are added individually or concurrently to the riboflavin solution to facilitate passage of riboflavin into the stroma.
A novel approach to promote riboflavin saturation into the corneal stroma is based on iontophoresis, a noninvasive delivery system designed to enhance the penetration of molecules into tissue using a small electric current. This technique was used to deliver drugs in various fields of medicine, including intraocular compartments. It generates a higher concentration compared to agent-free techniques and has been used in ophthalmology mainly for the treatment of posterior segment diseases. Recently the use of iontophoretic systems was proposed for riboflavin intracorneal delivery in CXL.
The present study aimed at determining differences in riboflavin concentration in the anterior, intermediate, and posterior stroma after 3 types of imbibition procedures (standard epi-off, epi-on, and iontophoresis-assisted administration) of 0.1% riboflavin in human donor corneas.
Methods
Riboflavin Imbibitions
After approval by the Review Board of the Department of Medicine and Ageing Sciences (University of Chieti, Italy), 10 human eye bank corneal buttons with scleral rims were included in the study. The mean donor age was 66.8 years (range 56-72 years). The average death-to-enucleation time was 6 hours (range 4 hours and 30 minutes to 11 hours and 15 minutes). The mean storage time (between eye bank procedures and cross-linking imbibitions) was 29.3 hours (range 20-48 hours).
For CXL imbibition, the corneoscleral buttons were mounted on an anterior chamber maintainer (Barron artificial anterior chamber; Katena Products Inc, Denville, New Jersey, USA), filled with Eusol-C storage media (Alchimia s.r.l., Ponte S. Nicolò, Italy) to obtain adequate pressure and stability of the corneal tissue.
Three corneas were treated according to a standard protocol, which consisted of removal of the central 10 mm of corneal epithelium and soaking the stroma with 0.1% riboflavin (Ricrolin; SOOFT Italia S.p.A., Montegiorgio, Italy) for 20 minutes within a dedicated silicon ring (Epi-off group).
Three corneas received riboflavin imbibition via a transepithelial approach. Ricrolin TE (0.1% riboflavin plus enhancers [including destrane T500, edetate sodium, tromethamine, bihydrate sodium phosphate monobasic, and bihydrate sodium phosphate bibasic]; SOOFT Italia S.p.A.) was applied with the same procedure described for the Epi-off group, for 30 minutes, using the same silicon ring imbibition system (Epi-on group). The enhancers in Ricrolin TE facilitate riboflavin penetration into the corneal stroma in the presence of an intact epithelium. In addition, penetration was increased by a longer duration of pretreatment with Ricrolin TE, as per reported protocols.
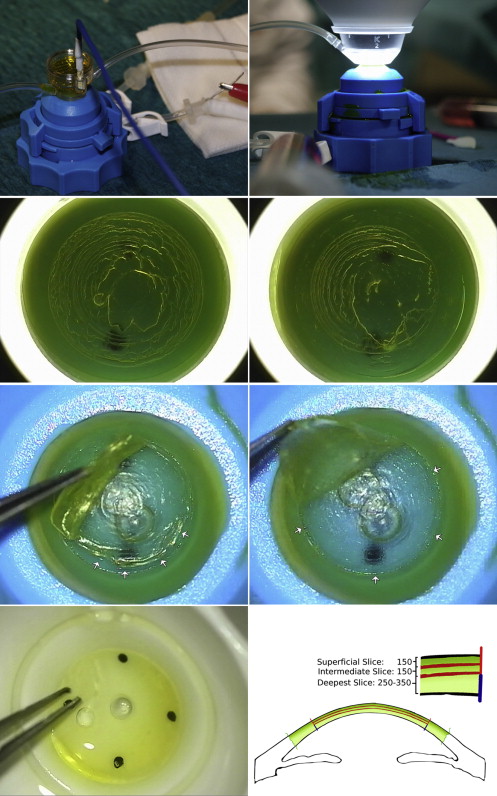
Three corneas were soaked with riboflavin using an iontophoresis system ( Figure 1 ), composed of a power supply (I-ON CXL; SOOFT Italia S.p.A.), 2 electrodes (the return electrode in the artificial system was a stainless steel wire inserted into the saline circuit and the negative electrode was a steel grid contained in a corneal applicator; Iontofor CXL, SOOFT Italia S.p.A.), and a connection cable. Adherence of the corneal applicator to the eye was maintained with a vacuum system.
After connecting the vacuum syringe to the Luer lock connector and verifying that the stop clamp was in the “open” position, the corneal applicator was put onto the cornea to be treated. Light suction was applied with the syringe (at least 1 mL) and the stop clamp was closed. The operator verified that the applicator was secured to the cornea.
The steel grid (negative electrode) was covered with Ricrolin+ (0.1% riboflavin solution specifically formulated to allow quick passage into the corneal stroma, through intact epithelium with corneal iontophoresis; SOOFT Italia S.p.A.).
The electrical generator was in the “OFF” position up to this point. After connecting the 2 electrodes to the power generator (the female red plug to the connector on the Iontofor CXL and the white male plug to the return electrode), the power generator was turned on (acoustic confirmation). The operator selected 1 mA and pressed START again. The procedure took 5 minutes (total current intensity 5 mA). The power supply software indicated the continuity of the procedure (the generator sounds an alarm if the current is interrupted).
The operator controlled that the steel grid was covered with riboflavin solution for the entire duration of the procedure, thus maintaining a regular flow of the electrical current.
After the iontophoretic procedure, the remaining riboflavin was removed through the specific tube and the stop clamp was opened to allow the air to enter the vacuum ring. The applicator was removed from the cornea and the power generator disconnected from the applicator and from the return electrode. The cornea was rinsed with saline solution.
One cornea was used as a control and was washed with a saline solution.
Femtosecond Laser Stromal Dissections
Three stromal slices of the corneal samples were prepared with a 500-kHz VisuMax femtosecond laser (FSL) (Carl Zeiss Meditec, Jena, Germany) immediately after the imbibition or control, maintaining the corneoscleral rims mounted in the artificial anterior chamber with controlled pressure. Before FSL stromal dissections of the corneas that underwent transepithelial riboflavin imbibition (belonging to Epi-on and Iontophoresis group) and in the control cornea, the epithelium was removed using a blunt spatula for a 10-mm diameter. Therefore, all FSL cuts were performed on denuded stroma in order to standardize the thickness of the 2 superficial slices and to ensure that high-performance liquid chromatography (HPLC) was conducted only on stroma.
The central corneal thickness was measured using an ultrasound pachymeter (Optikon 2000 S.p.A; Altair, Rome, Italy).
Each cornea was divided into 3 8.00-mm circular slices by performing 2 sequential lamellar dissections first at 300 and then at 150 μm from the corneal surface. A 90-degree (perpendicular to the corneal surface) side cut was performed. The FSL parameters were set as follows: spot-line separation between 2.0 and 2.5 μm for the lamellar cuts and 3.0 μm for the side cuts. The spot energy was between 135 and 150 nJ.
The 2 anterior stromal slices were removed using corneal graft toothed forceps and blunt spatula. The residual deep corneal slice was freed using an 8.00-mm cornea punch. Stromal slices were placed in histologic screw-capped containers, shielded from the light with aluminum foil, and stored at −20 C for subsequent HPLC analysis.
High-Performance Liquid Chromatography Analysis
HPLC analysis was subsequently performed to quantify the concentration of riboflavin in each volume of tissue.
Corneal samples were vortexed 1 minute in 500 μL of methanol and centrifuged at 13 200 rpm at room temperature. The supernatants were evaporated under a nitrogen stream at 40 C. The dry residue was dissolved in 50 μL of ultrapure water/methanol 70/30 (vol/vol) and vortexed for 1 minute. Tubes were centrifuged for 2 minutes at 13 200 rpm and 5 μL of the supernatant was injected into an HPLC/MS 1100 series system equipped with a simple Quadrupole LC/MSD 1100 (both Agilent Technologies, Santa Clara, California, USA). The HPLC analysis of riboflavin was performed with a Zorbax SB C18 column (2.1 mm, 50 mm, 3.5 μm; Agilent Technologies). The mobile phase (90% 0.1% formic acid and 10% acetonitrile) was used under isocratic conditions at a flow rate of 0.2 mL/min. Mass spectrometer parameters were: ionization mode: API-ES positive; drying gas flow: 11 l/min; nebulizer pressure: 20 psig; drying gas temperature: 350 C; capillary voltage: 4000 V; and mass-to-charge ratio (M/Z): 377.20. The lower limit for riboflavin quantification was 200 ng/mL. Calibration curves were obtained by plotting riboflavin peak area as a function of concentration.
Statistical Analysis
Statistical analysis was performed using SPSS 20.0 (IBM, Armonk, New York, USA). General linear model for repeated measures was used to compare the mean difference of riboflavin concentration over slices in the 3 treatment groups. A priori–specified contrast analysis was used for within–treatment group comparisons of riboflavin concentration.
Data were expressed as median and interquartile range (IQR) and graphed as a box-whisker plot. Statistical significance was assigned at P ≤ .05.
Results
The 3 groups did not present statistically significant differences in terms of donor age, death-to-enucleation time, and storage time ( Table ). Central corneal thickness values ranged between 566 and 630 μm (mean 592 μm) in the Epi-off group, between 545 and 614 μm (mean 575 μm) in the Epi-on group, and between 542 and 619 μm (mean 580 μm) in the Iontophoresis group. Differences in corneal thickness were not statistically significant.
| Patient | Age of Donor | Death-to-Enucleation | Storage Time | Treatment | Riboflavin Concentration (ng/g of Stroma) | ||
|---|---|---|---|---|---|---|---|
| Time (Hours) | (Hours) | Protocol | Superficial | Intermediate | Deep | ||
| 1 | 64 | 5.5 | 36 | Epi-off | 55 756 | 39 630 | 27 014 |
| 2 | 71 | 7.0 | 20 | Epi-off | 55 830 | 49 274 | 18 891 |
| 3 | 69 | 11.25 | 24 | Epi-off | 39 898 | 33 066 | 16 274 |
| 4 | 64 | 6.5 | 32 | Epi-on | 17 938 | 14 116 | 8153 |
| 5 | 71 | 4.5 | 46 | Epi-on | 10 500 | 7320 | 2938 |
| 6 | 56 | 8.0 | 32 | Epi-on | 6745 | 5215 | 4251 |
| 7 | 69 | 9.25 | 28 | Iontophoresis | 19 430 | 15 215 | 4083 |
| 8 | 72 | 8.5 | 48 | Iontophoresis | 23 277 | 17 333 | 10 277 |
| 9 | 66 | 5.25 | 32 | Iontophoresis | 28 009 | 24 540 | 14 816 |
| 10 | 66 | 4.5 | 22 | Control | 0 | 0 | 0 |
| Mean ± SD Group Concentration | |||||||
| Epi-off | 50 494 ± 5298 | 40 656 ± 4707 | 20 726 ± 3233 | ||||
| Epi-on | 11 728 ± 3289 | 8884 ± 2686 | 5114 ± 1566 | ||||
| Iontophoresis | 23 572 ± 2481 | 19 029 ± 2822 | 9725 ± 3111 | ||||
| Control | 0 | 0 | 0 | ||||
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


