Purpose
To compare qualitatively and quantitatively Optos fundus camera fluorescein angiographic images of retinal vascular leakage with 9-field montage Topcon fluorescein angiography (FA) images in patients with uveitis. We hypothesized that Optos images reveal more leakage in patients with uveitis.
Design
Retrospective, observational case series.
Methods
Images of all patients with uveitis imaged with same-sitting Optos FA and 9-field montage FA during a 9-month period at a single institution (52 eyes of 31 patients) were graded for the total area of retinal vascular leakage. The main outcome measure was area of fluorescein leakage.
Results
The area of apparent FA leakage was greater in Optos images than in 9-field montage images (median 22.5 mm 2 vs 4.8 mm 2 , P < 0.0001). Of the 49 (45%) eyes with gradable photos, 22 had at least 25% more leakage in the Optos image than in the montage image; 2 (4.1%) had at least 25% less leakage in Optos; and 25 (51%) were similar in the 2 modalities. There were 2 eyes that had no apparent retinal vascular leakage in 9-field montage but were found to have apparent leakage in Optos images. Of the 49 eyes, 23 had posterior pole leakage, and of these, 17 (73.9%) showed more posterior pole leakage in the Optos image. A single 200-degree Optos FA image captured a mean 1.50× the area captured by montage photography.
Conclusions
More retinal vascular pathology, in both the periphery and the posterior pole, is seen with Optos FA in patients with uveitis when compared with 9-field montage. The clinical implications of Optos FA findings have yet to be determined.
Fluorescein angiography (FA) is an important diagnostic modality in uveitis. In posterior uveitides, FA helps with the assessment of retinal and choroidal lesions, subretinal fluid, retinal perfusion, retinal vascular leakage, choroidal neovascularization (CNV), retinal neovascularization, and cystoid macular edema (CME). In anterior and intermediate uveitides, FA helps with assessment of CME and retinal vascular involvement. Most of these pathologies can occur in the retinal periphery in areas not imaged by standard 50-degree FA. Peripheral sweeps and montage photography are commonly used in patients with uveitis when the retinal periphery must be imaged. These techniques are labor intensive, require highly skilled photographers, and do not permit simultaneous imaging of the posterior pole and the periphery.
The Optos fundus camera (Optos, Dunfermline, Scotland, UK) can capture up to 200 degrees of the ocular fundus in a single photograph, greater than the 30- or 50-degree images typically captured by standard fundus cameras. When a single Optos image is compared with standard 7-field montage images, the Optos image includes 3.2 times the area of retina imaged in a standard 7-field montage. Comparison of 9-field fluorescein images with Optos images in our uveitis clinic has shown that the Optos images capture a larger area. For this reason, we hypothesized that Optos fluorescein images would capture more retinal vascular leakage than the 9-field montage.
Furthermore, we hypothesized that Optos fluorescein images reveal more retinal vascular leakage than standard images, even in areas that are captured adequately by both cameras. A fundus camera (eg, Topcon) and a scanning laser ophthalmoscope (SLO; eg, Optos) have fundamentally different illumination and light-capture technologies that result in differing image characteristics. A fundus camera uses the periphery of the objective lens to project the camera’s light source onto the fundus. The center of the lens then focuses reflected light onto the internal optics of the camera. An SLO, on the other hand, uses a narrow scanning laser light source that is focused onto the retina by an ellipsoidal mirror. Because the light source is narrow, a much larger percentage of the pupil is available to capture returning light. The Optos therefore allows not only wide for angle imaging but also produces a qualitatively different FA image.
At the National Eye Institute (NEI), numerous patients with uveitis-related retinal vascular leakage have had FA performed with a standard fundus camera (9-field montage) and the Optos SLO in the same sitting. Here, we review records from the NEI uveitis service to qualitatively and quantitatively compare these images.
Methods
The records of all patients with uveitis who underwent same-sitting 9-field montage and ultrawide field fluorescein angiography using the Optos Optomap Panoramic 200TW between July 1, 2011, and April 10, 2012, were reviewed retrospectively. Most patients undergoing montage fluorescein angiography also had late Optos imaging during this study period. Patients were identified from the NEI OIS Winstation image database (Ophthalmic Imaging Systems, Sacramento, CA). The NEI electronic medical record was reviewed for the following parameters: age, gender, anatomic classification of uveitis, and etiologic diagnosis. Patients were enrolled in one of several prospective NIH Combined Neurosciences Institutional Review Board–approved clinical research protocols, and charts were reviewed retrospectively under the terms of these protocols and in accordance with the Health Insurance Portability and Accountability Act and the Declaration of Helsinki.
Informed consent had been obtained from each patient for participation in a clinical research protocol and for each FA. The angiography procedure involved intravenous injection of 5 mL of sodium fluorescein 10% with the patient seated at the Topcon fundus camera (Topcon Medical Systems, Oakland, NJ). Transit images were obtained of the posterior pole with the Topcon camera, and peripheral imaging of both eyes began at approximately 2 minutes postinfusion. Once requisite peripheral photos for bilateral 9-field montage were completed, late images of the posterior pole were obtained in both eyes at 10 minutes. The patient then moved to the Optos machine for further imaging. Widefield images were obtained with the Optos in both eyes, and color images were also obtained on the Optos machine to assist in clinical correlation. Montage images were made using OIS Winstation software.
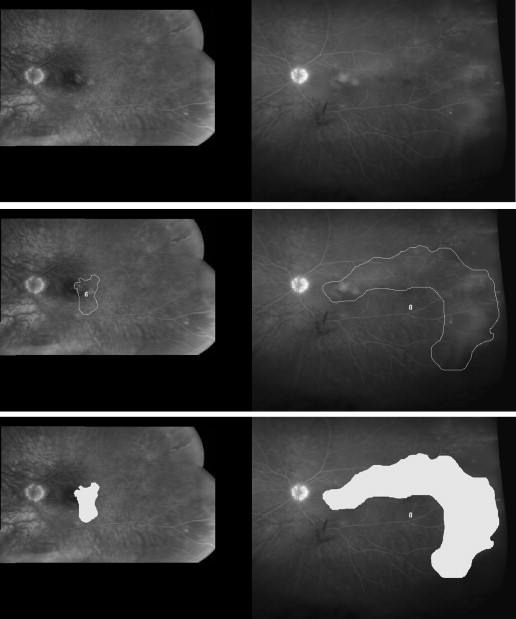
Some patients who met inclusion criteria had more than 1 series of photographs (eg, multiple clinical visits). In these cases, the earliest available visit was included in the study and used for analysis. Multiple late Optos FA images were usually obtained, so 1 representative image was chosen for analysis. Optos images were chosen based on overall image quality and inclusion of the posterior pole and peripheral pathology. Optos and montage images were processed with I2k alignment software (DualAlign, Clifton Park, NY). Alignment was intended to account in part for differential peripheral distortion between the 2 modalities. The histogram equalization function in Image J, a Java-based image processing program, was utilized to account for the variability in contrast between the Optos and montage images. This function allows for pixels to be evenly distributed throughout the image intensity range so the resulting image has a flat histogram. Figure 1 is an example of an aligned, adjusted image that was sent for grading.
Two masked, trained graders (DM, DN) independently analyzed the aligned images. Areas of apparent retinal vascular leakage were outlined using the software Image J in both images. Other hyperfluorescent pathologies, including staining and window defects, were not included in the measurements. The outline of the retinal pathology was verified by a third grader (BN). The outlined area was then assessed for surface area and greatest linear dimension (GLD) in pixels for both the Optos image and the montage. These pixel values were then converted into μm values with the assumption of a retinal vein diameter of 125 μm at the margin of the optic disc. The data were then averaged between the 2 graders to obtain the final values used for analysis. The pairs of photos were assessed for the presence of retinal vascular leakage and categorized as more, less, or same. These categories were defined based on a minimum 1 mm 2 and 25% difference between the 2 modalities. Posterior pole leakage was assessed using 10-minute-later FA images and subjectively categorized as more, same, or less as a secondary exploratory analysis.
To compare the surface area imaged with 9-field montage by the Optos, an artificial eye was used for both Optos and montage imaging. The artificial eye allowed the photographer unlimited time and unlimited eye positioning for ideal image capture. The ratio of the amount of artificial retinal surface area seen in a single Optos image vs the 9-field image was then calculated. A random subset of 10 study eyes was then selected for a similar exploratory analysis. The mean ratio of Optos surface area to montage surface area in these 10 eyes was calculated.
Statistical analyses were performed using SAS software (SAS Institute, Cary, NC). The Wilcoxon signed rank test was used to compare the area and GLD in the Optos images with the measurements in the montage images. It was also used to assess for differences between analyses from aligned and unaligned image pairs.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


