Purpose
To compare astigmatic keratotomy (AK) outcomes in high astigmatism after deep anterior lamellar keratoplasty (DALK) and after penetrating keratoplasty (PK) in keratoconus patients.
Design
Prospective, comparative, interventional case series.
Methods
This study comprised 20 eyes that underwent DALK and 24 eyes that underwent PK. After suture removal, all eyes had more than 5 diopters (D) of astigmatism and underwent standard manual 1-pair, 90-degree, and 90% corneal thickness AK incisions. The main outcome measures included preoperative and postoperative manifest refraction, uncorrected visual acuity, best spectacle-corrected visual acuity, surgically induced astigmatism, Orbscan II (Bausch & Lomb) corneal topography results, keratometric astigmatism, and complications.
Results
All eyes completed 6 months of follow-up. The overcorrection rate was 35% and 41.6% in the DALK and PK groups, respectively ( P = .75). At 6 months after AK, logarithm of the minimal angle of resolution uncorrected visual acuity improved from 0.88 ± 0.20 to 0.54 ± 0.26 and from 1.0 ± 0.34 to 0.53 ± 0.26 in the DALK and PK groups, respectively ( P = .01 to P <.01). Best spectacle-corrected visual acuity improved from 0.16 ± 0.09 to 0.13 ± 0.08 and from 0.16 ± 0.12 to 0.11 ± 0.08 in the DALK and PK groups, respectively ( P = .13 to P = .01). The mean refractive cylinder was decreased 2.74 ± 1.44 D in the DALK group and 3.18 ± 2.96 D in the PK group ( P = .35). Surgically induced astigmatism was 6.10 ± 3.27 D in the DALK group and 7.15 ± 2.98 D in the PK group ( P = .36).
Conclusions
The manual AK for the treatment of postkeratoplasty astigmatism after DALK and PK in keratoconus patients is a safe and effective surgical procedure, allowing similar refractive cylinder reduction and improvement in uncorrected visual acuity and best spectacle-corrected visual acuity.
High regular or irregular corneal astigmatism is a cause of visual impairment after corneal transplantation despite a clear corneal graft. Many studies have reported the presence of more than 5 diopters (D) of astigmatism after penetrating keratoplasty (PK). Deep anterior lamellar keratoplasty (DALK) with the big-bubble technique is a surgery developed with the aim of solving some limitations of PK. It consists of the replacement of diseased corneal stroma with donor stroma, whereas the patient’s own endothelium is retained. DALK has several advantages over PK, such as preservation of endothelium, reducing long-term use of steroids, and fast visual rehabilitation. A regular corneal surface may be expected after DALK surgery because of the better donor–host conformity and wider graft diameter. However, similar visual, refractive, and astigmatic results have been reported after DALK and PK surgery.
Several procedures attempting to manage postkeratoplasty astigmatism have been reported in the literature, including relaxing incisions with or without compression sutures, wedge resections, astigmatic keratotomy, photorefractive keratectomy, laser in situ keratomileusis, femtosecond laser arcuate keratotomy, and toric phakic intraocular lens implantation.
Although laser in situ keratomileusis has good results in mild and moderate astigmatism after keratoplasty, astigmatic keratotomy (AK) is the most widely used technique for high astigmatism after keratoplasty, because it is a safe and simple procedure, not affecting the central visual axis. AK has some disadvantages, including unpredictable results and development of irregular astigmatism. Different types of incisions in depth, arc length, and distance from the corneal center have been described for AK. Theoretically, deeper, more central, and longer incisions have a greater effect. However, integrity of the Descemet membrane may be affected with DALK surgery, and this also could affect AK results. The effect of intact continuity of the Descemet membrane on AK results for the treatment of high astigmatism after DALK still has not been investigated clinically. In this study, we compared the outcomes of manual AK for postkeratoplasty astigmatism management after DALK and PK in keratoconus patients. To the best of our knowledge, this is the first study comparing the outcomes of AK in patients with postkeratoplasty astigmatism who previously had undergone DALK and PK surgery.
Methods
Patient Selection
The study was a prospective, comparative, interventional case series that included 44 eyes of 40 consecutive patients who had been diagnosed with high symmetrical regular astigmatism after DALK procedures (20 eyes; DALK group) and PK procedures (24 eyes; PK group) for keratoconus. In all of these cases, manual AK was selected as treatment for the residual astigmatism. All patients received an explanation of the purpose of the study as well as advantages and disadvantages of the procedure.
Informed consent was obtained from all patients in accordance with the Declaration of Helsinki, and the Institutional Review Board of Kartal Training and Research Hospital, Istanbul, Turkey approved the study before it commenced. Eyes with at least 5 D of postkeratoplasty astigmatism were included. Best-corrected or pinhole visual acuity of all eyes was 20/40 or better, and all participants had a corneal graft well centered relative to the corneal light reflex, a corneal light reflex within 0.5 mm of the center of the entrance pupil, and a minimum of 10 central keratoscope rings of the corneal topography system accurately digitized in all eyes. Other inclusion criteria were no complications related to graft surgery, graft suture removal time of more than 1 year, a minimum follow-up of 3 months after suture removal, and stable refractive error. Eleven eyes of 10 patients required early resuturing (5 eyes in the DALK group and 6 eyes in the PK group) because of the overcorrection within 1 month of the manual AK incisions.
Surgical Technique
The incision site of the cornea was detected according to the steepest corneal meridian on the Orbscan II corneal topographic map. The steepest corneal meridian and arc length were marked using a corneal marker. Minimal corneal thickness was detected by intraoperative corneal pachymetry (Pacline Ultrasound Pacimetry; Opticon, Bologna, Italy). The incision site was placed 0.5 mm inside the host cornea. A pair of standard incisions was made in the steepest meridian through 90% of the corneal depth and with arc lengths of 90 degrees. All the operative procedures were performed by the same experienced surgeon (A.K.) and were carried out under topical anesthesia. After surgery, all patients were prescribed topical lomefloxacin 0.3% (Okacin; Novartis, Basel, Switzerland) and dexamethasone 0.1% (Maxidex; Alcon, Puurs, Belgium) eye drops to be applied 4 times daily for 4 weeks.
Measurement Protocol
All eyes were examined before surgery and at the first day, first week, first month, third month, and sixth month after surgery. At each follow-up visit, slit-lamp examination, applanation tonometry, and outcome measurements, including uncorrected visual acuity (UCVA), best spectacle-corrected visual acuity (BSCVA), manifest refraction, and corneal topography (Orbscan II; Bausch & Lomb, Rochester, New York, USA), were performed. All complications were also recorded. UCVA and BSCVA were measured in decimal Snellen scale and were converted to the logarithm of the minimal angle of resolution (logMAR) scale for analysis. The Alpins method of vector analysis was used to evaluate corneal astigmatic changes. All of these calculations were performed using ASSORT software (ASSORT Pty. Ltd, Cheltenham, Australia), which is especially designed for using Alpins vectorial analysis. The following vectors were determined and evaluated: targeted induced astigmatism (TIA) as the vector of intended change in cylinder for each treatment, surgically induced astigmatism (SIA) as the vector of the real change achieved, and difference vector as the additional astigmatic change that would enable the initial surgery to achieve its intended target. Additionally, the following parameters derived from the relationship between these vectors were calculated and analyzed at each postoperative visit:
- 1
Magnitude of error: the arithmetic difference between the magnitudes of the SIA and TIA.
- 2
Angle of error: the angle described by the vectors of the achieved correction (SIA) and the intended correction (TIA).
- 3
Flattening effect: the amount of astigmatism reduction achieved by the effective proportion of the SIA at the intended meridian. It was calculated using a previously described mathematical relationship.
- 4
Torque: the amount of astigmatic change induced by the SIA, because of nonalignment of the treatment, that has been ineffective in reducing astigmatism at the intended meridian, but causes rotation and a small increase in the existing astigmatism. It was calculated using a previously described mathematical relationship.
- 5
Coefficient of adjustment: calculated by dividing TIA by SIA. Its value is preferably 1.0 and it is the inverse of the correction index.
- 6
Correction index: the inverse of the coefficient of adjustment. It is greater than 1.0 if an overcorrection occurs and less than 1.0 if there is an undercorrection.
- 7
Index of success: calculated by dividing the difference vector by the TIA. It is a relative measure of success and is also preferably 0.
- 8
Flattening index: calculated by dividing the flattening effect by the TIA.
With this methodology, all polar coordinates of astigmatism were converted to Cartesian (x, y) coordinates. Refractive measurements from the spectacle plane were vertexed to the corneal plane using a nominal vertex distance of 12.00 mm.
Statistical Analysis
SPSS software version 11.5 (SPSS for Windows software; SPSS, Inc, Chicago, Illinois, USA) was used for statistical analyses between both the DALK and PK groups. First, it was proven by means of the Kolmogorov-Smirnov test that data samples did not follow a normal distribution. Then, the Wilcoxon rank-sum test was used in intragroup data analysis, and the Mann–Whitney U test was used for intergroup data analysis. The Spearman correlation test was used to investigate the correlation between different variables. A P value less than .05 was considered statistically significant.
Results
All patients completed the 6-month follow-up period. The mean interval from keratoplasty to AK was 22.6 ± 6 months (range, 14 to 38 months) in the DALK group and 28.5 ± 14.4 months (range, 16 to 88 months) in the PK group ( P = .06). The preoperative patient data are shown in Table 1 .
| DALK | PK | P Value a | |
|---|---|---|---|
| Age (yrs) | 25.6 ± 3.2 | 30.2 ± 8.5 | .09 |
| Interval between keratoplasty and astigmatic keratotomy (mos) | 22.6 ± 6.0 | 28.5 ± 14.4 | .06 |
| Interval between keratoplasty and suture removal (mos) | 16.1 ± 3.94 | 17.3 ± 4.1 | .24 |
| Interval between suture removal and astigmatic keratotomy (mos) | 6.5 ± 3.9 | 11.3 ± 15.2 | .27 |
| Donor trephine size (mm) | 8.0 ± 0.23 | 7.95 ± 0.4 | .52 |
| UCVA (logMAR) | 0.88 ± 0.20 | 1.0 ± 0.34 | .20 |
| BSCVA (logMAR) | 0.16 ± 0.09 | 0.16 ± 0.12 | .71 |
| Spherical equivalent (D) | −4.53 ± 2.51 | −5.29 ± 2.79 | .35 |
| Refractive cylinder (D) | −6.24 ± 0.75 | −6.48 ± 1.45 | .31 |
| Keratometric astigmatism (D) | 7.44 ± 1.98 | 7.92 ± 1.46 | .12 |
Visual Acuity
In the DALK group, logMAR UCVA improved from 0.88 ± 0.20 before surgery to 0.54 ± 0.26 at 6 months after surgery ( P = .01). In the PK group, UCVA improved from 1.0 ± 0.34 before surgery to 0.53 ± 0.26 at 6 months after AK ( P < .01). BSCVA improved with surgery from 0.16 ± 0.09 to 0.16 ± 0.12 and from 0.13 ± 0.08 to 0.11 ± 0.08 in DALK and PK groups, respectively ( P = .13 to P = .01). In addition, as shown in Tables 1 and 2 , no statistically significant differences among groups were found before surgery and after surgery ( P ≥ .05). There was no significant difference in UCVA and BSCVA between the 3-month and 6-month postoperative values in either group ( Table 2 ). UCVA improved 1.9 Snellen lines in the DALK group (range, no change to gain of 6 lines) and 2.3 Snellen lines in the PK group (range, no change to gain of 7 lines) at 6 months after AK. Although improvement in BSCVA in the DALK group was not significant, the BSCVA improved 0.6 Snellen lines in the DALK group (range, loss of 1 line to gain of 3 lines) and 1.1 Snellen lines in the PK group (range, loss of 1 line to gain of 3 lines).
| DALK | PK | P Value a | |
|---|---|---|---|
| UCVA (logMAR) | |||
| Third month | 0.53 ± 0.30 | 0.57 ± 0.27 | .79 |
| Sixth month | 0.54 ± 0.26 | 0.53 ± 0.26 | .78 |
| P value b | .93 | .11 | |
| BSCVA (logMAR) | |||
| Third month | 0.11 ± 0.09 | 0.13 ± 0.11 | .84 |
| Sixth month | 0.13 ± 0.08 | 0.11 ± 0.08 | .51 |
| P value b | .32 | .11 | |
| Spherical equivalent (D) | |||
| Third month | −3.12 ± 2.93 | −3.32 ± 2.39 | .99 |
| Sixth month | −2.94 ± 2.71 | −3.11 ± 2.17 | .98 |
| P value b | .08 | .07 | |
| Refractive cylinder (D) | |||
| Third month | −3.84 ± 1.69 | −3.75 ± 1.66 | .94 |
| Sixth month | −3.53 ± 1.62 | −3.31 ± 2.18 | .41 |
| P value b | .45 | .12 | |
| Keratometric astigmatism (D) | |||
| Third month | 4.24 ± 1.85 | 3.73 ± 1.94 | .45 |
| Sixth month | 4.17 ± 1.78 | 3.72 ± 2.18 | .37 |
| P value b | .39 | .94 |
Refractive and Keratometric Analysis
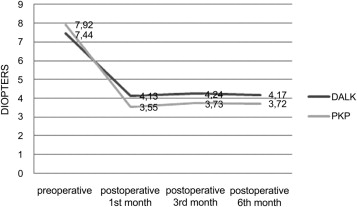
The mean refractive cylinder 6 months after AK surgery was decreased from 6.24 ± 0.75 D to 3.53 ± 1.62 D in the DALK group and from 6.48 ± 1.45 D to 3.31 ± 2.17 D in the PK group, respectively ( P < .001 to P = .001). The mean refractive cylinder reduction was 2.74 ± 1.44 D in the DALK group and 3.18 ± 2.96 D in the PK group ( P = .35). The decrease in refractive cylinder was 43% ± 25% in the DALK group and 52% ± 30% in the PK group. Keratometric astigmatism decreased 3.27 ± 2.15 D in the DALK group and 4.27 ± 2.57 D in the PK group ( P = .20; Figure ). The mean spherical equivalent 6 months after AK surgery decreased from −4.53 ± 2.51 D to −2.94 ± 2.71 D in the DALK group and from −5.29 ± 2.79 D to −3.11 ± 2.17 D in the PK group, respectively ( P ≤ .001 to P ≤ .001). There was no significant difference in refractive cylinder, keratometric astigmatism, or spherical equivalent between the postoperative values and the 3- and 6-month postoperative values ( Table 2 ). All patients had symmetrical astigmatism before surgery, whereas 7 eyes (35%) in the DALK group and 9 eyes (37.5%) in the PK group had asymmetrical astigmatism at 6 months after surgery.
Vector Analysis
Refractive Alpins indices also were calculated for each group for the 3- and 6-month follow-up, and they are summarized in Table 3 . A trend to a slight postoperative undercorrection of cylinder was observed in the DALK group (magnitude of error negative), but differences in this vector index among groups did not reach statistical significance. No statistically significant differences in the remaining Alpins indices were found between groups at 6 months after surgery. On average, the largest rotation of the intended treatment was observed in the DALK group (largest magnitude of torque vector), although differences among groups did not reach statistical significance, probably because of the largest variability of data observed in the DALK group.
| DALK | PK | P Value a | |
|---|---|---|---|
| TIA | |||
| Third month | 6.27 ± 0.79 | 6.43 ± 1.47 | .46 |
| Sixth month | 6.26 ± 0.79 | 6.53 ± 1.62 | .29 |
| P value b | .99 | .98 | |
| SIA | |||
| Third month | 6.22 ± 3.22 | 7.15 ± 2.39 | .29 |
| Sixth month | 6.10 ± 3.27 | 7.15 ± 2.98 | .36 |
| P value b | .97 | .89 | |
| DV | |||
| Third month | 4.72 ± 2.64 | 6.10 ± 5.0 | .98 |
| Sixth month | 4.63 ± 3.96 | 4.19 ± 3.87 | .34 |
| P value b | .91 | .19 | |
| AOE | |||
| Third month | 5.75 ± 25.2 | −4.75 ± 34.2 | .34 |
| Sixth month | 2.24 ± 17.61 | −7.14 ± 27.77 | .23 |
| P value b | .99 | .72 | |
| Absolute AOE | |||
| Third month | 19.5 ± 16.3 | 19.9 ± 27.8 | .21 |
| Sixth month | 13.88 ± 10.52 | 15.68 ± 23.81 | .12 |
| P value b | .39 | .58 | |
| MOE | |||
| Third month | −0.09 ± 3.21 | 0.73 ± 2.47 | .40 |
| Sixth month | −0.08 ± 3.16 | 0.71 ± 2.78 | .59 |
| P value b | .73 | .89 | |
| CI | |||
| Third month | 0.97 ± 0.51 | 1.16 ± 0.43 | .32 |
| Sixth month | 0.97 ± 0.49 | 1.17 ± 0.54 | .41 |
| P value b | .86 | .75 | |
| IOS | |||
| Third month | 0.74 ± 0.37 | 0.83 ± 0.80 | .54 |
| Sixth month | 0.63 ± 0.27 | 0.64 ± 0.59 | .17 |
| P value b | .72 | .48 | |
| COA | |||
| Third month | 1.69 ± 1.77 | 1.11 ± 0.56 | .50 |
| Sixth month | 1.46 ± 1.11 | 0.87 ± 0.93 | .24 |
| P value b | .55 | .24 | |
| TOR | |||
| Third month | 2.72 ± 1.95 | 1.77 ± 1.58 | .07 |
| Sixth month | 2.08 ± 1.42 | 1.71 ± 1.98 | .16 |
| P value b | .48 | .53 | |
| SE | |||
| Third month | 5.08 ± 3.75 | 7.09 ± 3.88 | .10 |
| Sixth month | 5.54 ± 3,32 | 6.97 ± 4.22 | .41 |
| P value b | .28 | .86 | |
| FI | |||
| Third month | 0.76 ± 0.60 | 0.62 ± 0.98 | .64 |
| Sixth month | 0.77 ± 0.67 | 0.75 ± 0.88 | .72 |
| P value b | .20 | .47 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


