Purpose
To investigate the histopathology in a large series of autopsy eyes from children with abusive head trauma.
Design
Retrospective case-control series.
Methods
One hundred and ten eyes from 55 autopsies examined at an academic tertiary referral center over 21 years were tabulated for histopathology: subdural hemorrhage in the optic nerve sheath, intrascleral hemorrhage, any retinal hemorrhage, ora-extended hemorrhage, cherry hemorrhage, perimacular ridge, and internal limiting membrane tear. Select tissues with cherry hemorrhage were further examined by transmission electron microscopy.
Results
Sixty eyes were identified as “abusive head trauma” (cases), 46 as “alternative cause” (controls), and 4 as “abusive head trauma survivor”. Cases were legally verified or confirmed by confession in all except 1 case. All ocular histopathologic observations from cases were similar or more frequent in infants younger than 16 months of age. When present, a cherry hemorrhage and perimacular ridge were most often found together, and only with a torn internal limiting membrane. Both abusive head trauma survivor cases demonstrated severe optic nerve atrophy and macular ganglion cell loss.
Conclusions
Younger infants may be even more susceptible to damage from vitreomacular traction by rotational and/or acceleration–deceleration forces. Identifying cherry hemorrhages may aid abusive head trauma diagnosis. Survivor abusive head trauma pathology demonstrates unique, irreversible macular and optic nerve damage.
Shaken baby syndrome, currently termed abusive head trauma, was first described in 1974 in regard to the physical abuse of children and is characterized by findings such as the perimacular retinal fold. Controversy now exists regarding the primary mechanism responsible for the ocular findings found in abusive head trauma, despite the overwhelming evidence in support of the theory of acceleration–deceleration forces solely induced by vigorous shaking. Other hypotheses attribute optic nerve sheath and retinal bleeding to a rise in intracranial pressure from myriad other causes, including intracranial hemorrhage or pressure increases elsewhere in the circulation, such as the abdomen and thorax. These other postulations, however, do not fully consider ocular anatomy, as intense cardiopulmonary resuscitation with presumably high intrathoracic pressures in a relatively large study failed to generate retinal hemorrhages in pediatric patients with a normal coagulation profile and platelet count.
Other viewpoints suggest that the combination of hypoxia, brain swelling, and raised central venous pressure may cause extravasation into the subdural space owing to immaturity rather than direct venous rupture required by considerable force. This complexity of multiple contributing inflammatory factors induced by shaking, then, may account for the subdural bleeding within the brain rather than mechanical forces on the bridging veins alone. It was found that shaking forces, when isolated, are insufficient to cause such documented damage and instead require angular acceleration from impact, albeit in the clinical vacuum of a biomechanical model. However, ocular anatomy and its related biomechanics are not addressed. An extra layer of complexity must be considered given the unique anatomy of the vitreous and retinal tissues.
Perimacular folds, a well-established finding associated with abusive head trauma, are described as white retinal ridges surrounding the macula and have long been attributed to the vitreous traction on the neurosensory retina during shaking episodes. Although they are commonly found in cases of abusive head trauma, there have been 3 documented cases of this retinal ridge clinically that were all attributable to severe crush injury, only 1 of which has histopathologic evidence. However, to our knowledge, there are no reports of perimacular ridge formation in instances of minimal trauma or cardiopulmonary resuscitation. Therefore, it is our suspicion that a sufficient amount of acceleration–deceleration forces in conjunction with vitreous traction is required to produce these findings.
Herein, we examine the histopathologic findings of confirmed abusive head trauma cases in the Barbara W. Streeten, MD, Eye Pathology Laboratory. We also describe a unique type of hemorrhage that may be associated with abusive head trauma. Finally, we report unique ocular findings on autopsy of 2 survivors who died 2 years after abusive head trauma diagnosis.
Subjects and Methods
This monocenter, retrospective, case-control series was reviewed at the Barbara W. Streeten, MD, Eye Pathology Laboratory at the State University of New York, Upstate Medical University in Syracuse, New York over a 21-year period (1994–2014). This study met Health Insurance Portability and Accountability Act requirements for research on decedents. Institutional review board review was waived by the State University of New York, Upstate Medical University Institutional Review Board, as the research did not involve information about living individuals.
One hundred and ten autopsy eyes from 55 cases suspicious for child abuse were examined. All eyes were formalin-fixed before gross and histopathologic examination (A.B.G.). Their eye pathology reports were retrospectively tabulated (M.P.B., K.H.U.) for the following findings: subdural hemorrhage in the optic nerve sheath, intrascleral hemorrhage, any retinal hemorrhage, hemorrhage extending to the ora serrata, cherry hemorrhage, perimacular ridge, and internal limiting membrane (ILM) tear (separated/detached from retina). Photomicroscopy was performed using the Olympus D28-CB apparatus (Olympus, Tokyo, Japan). Transmission electron microscopy (TEM) was used for 1 autopsy specimen sample. It required fixation in glutaraldehyde, post-fixation in osmium tetroxide, ethanol dehydration, infiltration with propylene oxide, and embedding before imaging by means of a Tecnai 12 BioTwin transmission electron microscope (Field Emission Incorporated, Hillsboro, Oregon, USA). Statistical analysis was performed by hand for odds ratios, proportion calculations, and population estimations, as well as using Microsoft Excel 2011 (Microsoft Inc, Seattle, Washington, USA) for independent t tests. The pathologic data and findings were analyzed with respect to the medico-legal and clinical history.
Based on histopathologic, clinical, and legal findings, each case (n = number of eyes) was placed in 1 of 3 causal groups: “abusive head trauma” (n = 60), “abusive head trauma survivor” (n = 4), and “alternative cause” (n = 46). All abusive head trauma cases, except 1, were legally verified by confession or conviction. With abusive head trauma survivor eyes, both cases involved severe, documented, nonaccidental shaking at least 2 years prior to death with significant neurologic and visual deficits; ultimate causes of death were most likely from indirectly related, chronic sequellae of the initial abuse. The alternative cause group was composed of eyes inconsistent with abusive head trauma, including suffocation, drowning, other bodily trauma, and sudden infant death syndrome/unknown. This latter group was treated as controls during relevant statistical analyses.
Results
Pathologic observations were found to be statistically more frequent with abusive head trauma (cases) than with alternative cause (controls). For each finding in the abusive head trauma group, the percent prevalence, odds ratio between cases and controls, and the corresponding 95% odds ratio confidence interval were as follows: subdural hemorrhage in the optic nerve sheath, 97%, 1305, 114.7–14 851.0; intrascleral hemorrhage, 63%, 79.5, 10.2–616.9; any retinal hemorrhage, 83%, 33.3, 11.2–99.6; hemorrhage extending to the ora, 70%, 107.3, 13.7–839.4; cherry hemorrhage, 40%, 30.7, 4.0–237.6; perimacular ridge, 42%, 15.7, 3.5–70.9; and ILM tear, 85%, 46.5, 14.5–149.4. The odds ratio for cherry hemorrhage, hemorrhage extending to ora, and intrascleral hemorrhage required substituting 1 for 0 in order to avoid indeterminate calculations for control eyes that lacked each of these 3 associated findings, thereby making the corresponding odds ratio estimations conservative. Perimacular ridges were found in only 2 control eyes, both from the same case: a 16-month-old male infant, who was feeding koi fish in a pond with family nearby, drowned and perished despite shaking resuscitative efforts upon rescue from the pond.
The Table shows pathologic observations of the abusive head trauma group organized relative to laterality, sex, and age. Pathologic findings were more commonly seen bilaterally than unilaterally for every observation. Each one had similar or greater frequency in younger infants. Specifically, subdural hemorrhage (2-tailed, unpaired, independent t tests, P = .030), any retinal hemorrhage ( P = .048), hemorrhage extending to the ora serrata ( P = .024), ILM tear ( P = .002), and formation of the perimacular ridge ( P = .044) were all significantly more frequent in infant eyes younger than 16 months. There was no significant difference regarding age in findings of intrascleral hemorrhage ( P = .306) or cherry hemorrhage ( P = .334). No significant difference with respect to sex was found ( P > .05). The alternative cause group demonstrated zero to few positive findings for each category ( Table ).
| Subdural Hemorrhage | Intrascleral Hemorrhage | Any Retinal Hemorrhage | Hemorrhage Extending to Ora | Cherry Hemorrhage | Perimacular Ridge | Internal Limiting Membrane Tear | |
|---|---|---|---|---|---|---|---|
| Abusive head trauma (eyes, n = 60) | 96.7 ± 2.3 | 63.3 ± 6.3 | 83.3 ± 4.9 | 70.0 ± 6.0 | 40.0 ± 6.4 | 41.7 ± 6.4 | 85.0 ± 4.6 |
| Laterality | |||||||
| Unilateral (cases, n = 30) | 0 | 20.0 ± 7.4 | 20.0 ± 7.4 | 26.7 ± 8.2 | 20.0 ± 7.4 | 10.0 ± 5.6 | 3.3 ± 3.3 |
| Bilateral (cases, n = 30) | 96.7 ± 3.3 | 53.3 ± 9.3 | 73.3 ± 8.2 | 56.7 ± 9.2 | 30.0 ± 8.5 | 36.7 ± 8.9 | 83.3 ± 6.9 |
| Neither (cases, n = 30) | 3.3 ± 3.3 | 26.7 ± 8.2 | 6.7 ± 4.6 | 16.7 ± 6.9 | 50.0 ± 9.3 | 53.3 ± 9.3 | 13.3 ± 6.3 |
| Sex | |||||||
| Female (eyes, n = 36) | 94.4 ± 3.9 | 66.7 ± 8.0 | 83.3 ± 6.3 | 69.4 ± 7.8 | 30.6 ± 7.8 | 36.1 ± 8.1 | 88.9 ± 5.3 |
| Male (eyes, n = 24) | 100 | 58.3 ± 10.2 | 83.3 ± 7.8 | 70.8 ± 9.5 | 54.2 ± 10.4 | 50.0 ± 10.4 | 83.3 ± 7.8 |
| P value a | .2475 | .5199 | 1 | .9103 | .0693 | .2930 | .5431 |
| Age | |||||||
| 1–15 months (eyes, n = 38) | 100 | 65.8 ± 7.8 | 89.5 ± 5.0 | 78.9 ± 6.7 | 42.1 ± 8.1 | 50.0 ± 8.2 | 94.7 ± 3.7 |
| 17–30 months (eyes, n = 22) | 90.9 ± 4.8 | 59.1 ± 7.9 | 72.7 ± 6.9 | 54.5 ± 8.3 | 36.4 ± 8.3 | 27.3 ± 7.9 | 68.2 ± 7.5 |
| P value a | .0301 ∗ | .3055 | .0483 ∗ | .0239 ∗ | .334 | .0440 ∗ | .0025 ∗ |
| Alternative cause (eyes, n = 46) | 2.2 ± 2.2 | 0 | 13.0 ± 5.0 | 0 | 0 | 4.3 ± 3.0 | 10.9 ± 4.6 |
a Two-tailed, unpaired, independent t test.
All 60 abusive head trauma eyes had at least 1 histopathologic finding from the retinal hemorrhages, ocular hemorrhages, or vitreoretinal interface pathology groups, as illustrated in set (Venn) diagrams showing overlapping relationships ( Figure 1 ). Fifty eyes (83%) had retinal hemorrhages, while 10 (17%) did not have a retinal hemorrhage of any kind ( Figure 1 , Left panel). Of those positive for retinal hemorrhages, 42 (84%) had hemorrhages extending to the ora serrata, and 24 (48%) had a cherry hemorrhage. All 24 eyes (100%) with a cherry hemorrhage had hemorrhages extending to the ora serrata. Among the 42 eyes with hemorrhage extending to the ora, 18 (43%) did not have a cherry hemorrhage.

Every abusive head trauma autopsy eye (100%) had at least 1 type of ocular hemorrhage ( Figure 1 , Middle panel). Thirty-three of the 60 eyes (55%) had all 3 types of ocular hemorrhage: retinal hemorrhage, intrascleral hemorrhage, and subdural hemorrhage. Out of the 50 eyes with retinal hemorrhages, only 1 (2%) lacked either a subdural or intrascleral hemorrhage. Within these, 33 (66%) had both subdural and intrascleral hemorrhages, while 15 (30%) had a subdural without intrascleral hemorrhage, and 1 (2%) had an intrascleral without subdural hemorrhage. Subdural hemorrhage was present in 58 eyes (97%), of which 33 (57%) also had retinal and intrascleral hemorrhages. Only 6 of these eyes (10%) positive for subdural hemorrhage had neither retinal nor intrascleral hemorrhages, while 15 (26%) had retinal hemorrhage of any kind without intrascleral hemorrhage, and 4 (6.9%) had intrascleral hemorrhage without retinal hemorrhage. Therefore, 10 eyes (17%) had subdural hemorrhage without retinal hemorrhage, of which 6 had unilateral retinal hemorrhages and 4 lacked retinal hemorrhages bilaterally. Intrascleral hemorrhage was present in 38 eyes (63%): 33 of those eyes (87%) also had subdural and retinal hemorrhages, 4 (11%) had subdural without retinal hemorrhages, and 1 (2.6%) had retinal without subdural hemorrhage. Intrascleral hemorrhage always accompanied a retinal or subdural hemorrhage.
Vitreoretinal interface abnormalities were seen in 51 abusive head trauma eyes (85%) ( Figure 1 , Right panel). ILM tear in isolation was the most common observation in 22 eyes (37%). The incidence of ILM tear with a perimacular ridge and cherry hemorrhage was 20 (33%), while incidence of only ILM tear and a perimacular ridge was 5 (8%) and of only cherry hemorrhage with ILM tear was 4 (6.7%). Every eye with a perimacular ridge or cherry hemorrhage had a torn ILM. In eyes with ILM tear, 20 (39%) also had a cherry hemorrhage and a perimacular ridge, 5 (10%) had a perimacular ridge without a cherry hemorrhage, 4 (7.8%) had a cherry hemorrhage without a perimacular ridge, and 22 (43%) did not have an accompanying perimacular ridge or a cherry hemorrhage. In total, 24 (40%) eyes had a cherry hemorrhage: 20 (83%) also had ILM tears and a perimacular ridge, while 4 (17%) had an ILM tear without a perimacular ridge. There were 25 (42%) eyes out of 60 with perimacular ridges: 20 (80%) also had both cherry hemorrhages and ILM tears, while 5 (20%) had a torn ILM without a cherry hemorrhage.
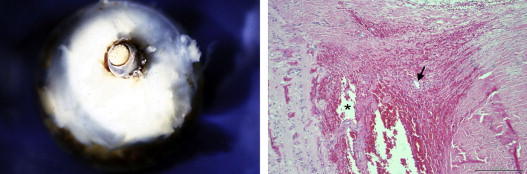
Subdural hemorrhage at the optic nerve has a bluish hue externally. In cross-section, the blood is visible inside the dura ( Figure 2 , Left). Microscopically, intrascleral hemorrhage is found surrounding ruptured intrascleral vessels at the junction of the optic nerve and sclera ( Figure 2 , Right). Intrascleral bleeding is often continuous with the subdural space.
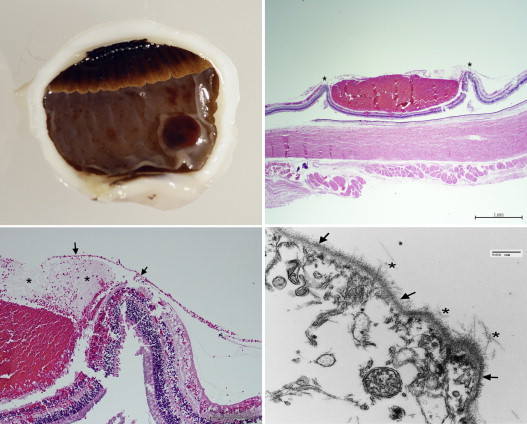
Typical perimacular ridges are elevated, circular retinal folds with a canopy of ILM above, torn away from retina, with fibrin-hemorrhage debris below. Often a portion of the perimacular ridge can be seen clinically, surrounding hemorrhage at the macula ( Figure 3 , Top left). On gross and microscopic examination, retinal ridges have a canopy of detached ILM over the ridge with hemorrhage and fibrin below ( Figure 3 , Top middle and Bottom).
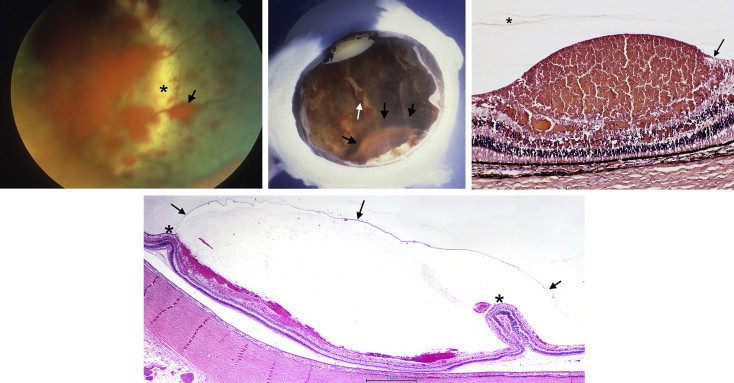
A cherry hemorrhage is an isolated, single, circular, elevated bleed, typically in the equatorial retina, that is observable by gross examination ( Figure 4 , Top left). Smaller cherry hemorrhages are focal hemorrhagic detachments of the ILM without an obvious break ( Figure 3 , Top right). Larger ones, microscopically, show a retinal ridge with torn ILM canopy surrounding blood and fibrin beneath ( Figure 4 , Top right and Bottom left). Ultrastructurally, the basement membrane of the ILM is composed of attached vitreous fibrils on one side and Müller cell remnants on the other ( Figure 4 , Bottom right). Every eye with a cherry hemorrhage had at least 1 documented ILM tear elsewhere in that eye.