Purpose
To report the clinical outcomes of repeat autologous cultivated limbal epithelial transplantation in patients with recurrence of limbal stem cell deficiency after a failed primary procedure.
Design
Retrospective case series.
Methods
This study included 50 patients, above 8 years of age, with clinically diagnosed unilateral limbal stem cell deficiency following ocular surface burns, treated between 2001 and 2010. Following failure of primary surgery all patients underwent a repeat limbal biopsy from the unaffected eye. The limbal cells were expanded ex vivo on a human amniotic membrane substrate for 10 to 14 days using a completely xeno-free explant culture technique. The resulting cultured epithelial monolayer and amniotic membrane were transplanted onto the patient’s affected eye. All patients underwent a comprehensive ophthalmic examination of both eyes at every follow-up visit. Postoperative corneal surface stability, change in visual acuity, and complications were objectively analyzed.
Results
At a mean follow-up of 2.3 ± 1.4 (median: 1.96, range: 1 to 7.5) years, 33 of the 50 recipient eyes (66%) maintained a completely epithelialized, avascular, and clinically stable corneal surface. A 2-line improvement in visual acuity was seen in 38 of the 50 recipient eyes (76%). None of the donor eyes developed any clinical features of ocular surface disease, conjunctival overgrowth of the donor site, or decrease in vision throughout the follow-up period.
Conclusions
Repeat autologous cultivated limbal epithelial transplantation successfully restores corneal epithelial stability and improves vision in eyes with recurrence of limbal stem cell deficiency, following failed primary surgery for ocular burns, without adversely affecting donor eyes.
The discovery of the corneal epithelial stem cells at the limbus led to a better understanding of the pathogenesis of ocular surface disease following inflammatory or traumatic limbal damage. This new knowledge also helped in developing a novel approach for treating eyes with limbal stem cell deficiency, which involved transplantation of a part of the limbus, containing viable stem cells, from a healthy eye onto the diseased eye. First described by Kenyon and Tseng, the surgical technique of limbal transplantation has since evolved from conjunctival-limbal grafting to ex vivo–cultivated limbal epithelial transplantation, introduced by Pellegrini and associates.
Over the course of the last decade, the cultivated technique of limbal transplantation has become increasingly popular, especially for the treatment of unilateral limbal stem cell deficiency. Requirement of only small amounts of donor tissue and hence a better safety profile for the donor eyes has made this technique the preferred method of limbal transplantation, wherever suitable laboratory facilities are available. However, despite the advances in cell-based therapy, treatment failures are not uncommon. In extensive literature reviews by Baylis and associates and Shortt and associates it was noted that on an average, one-third of all treated patients developed recurrence of limbal stem cell deficiency, usually within the first year.
In patients with failed primary surgery, a second limbal biopsy followed by ex vivo cultivation and transplantation can be considered. The only existing report on repeat autologous cultivated limbal transplantation is by Rama and associates, who regrafted 10 eyes once and 1 eye twice with an overall success rate of 81.8%. However, the impact of a second biopsy on the donor eye was not studied in that report. To fill this gap in the existing scientific literature, we report the clinical outcomes of repeat autologous cultivated limbal epithelial transplantation for the treatment of unilateral limbal stem cell deficiency following ocular surface burns.
Methods
Study Design and Subjects
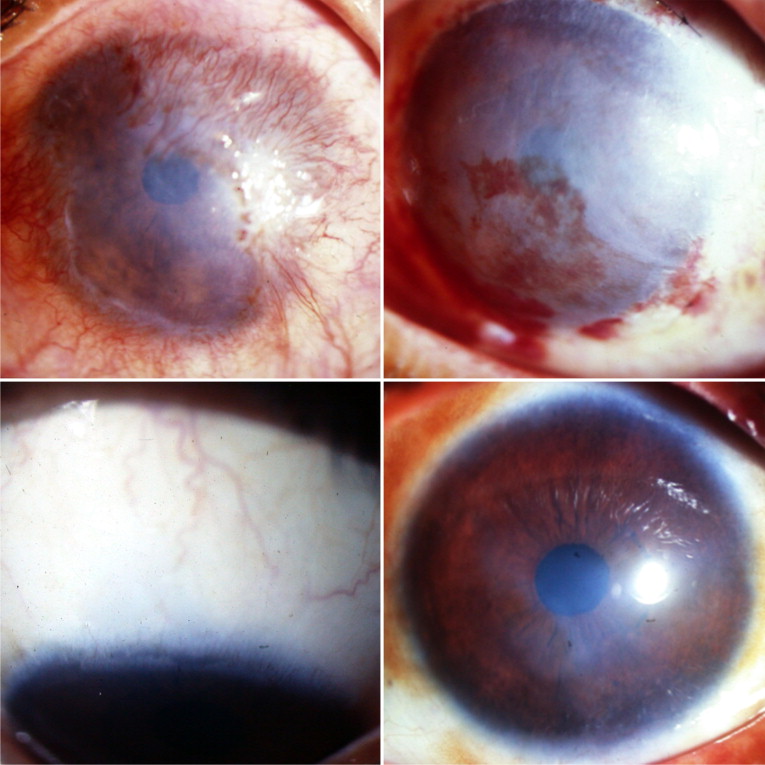
A retrospective chart review of all patients who underwent cultivated limbal epithelial transplantation for the treatment of limbal stem cell deficiency between April 1, 2001 and April 1, 2010 was carried out. Of the 200 patients who underwent primary autologous cultivated limbal epithelial transplantation for unilateral total limbal stem cell deficiency following ocular surface burns, those who developed recurrence of limbal stem cell deficiency and underwent a repeat procedure were included in this study. Total limbal stem cell deficiency was defined clinically as 360-degree absence of limbal palisades of Vogt, superficial corneal vascularization, diffuse fluorescein staining of the corneal surface with or without persistent epithelial defects, or conjunctivalization of the corneal surface ( Figure 1 ) .
The exclusion criteria were similar to the previous study, namely: 1) patients less than 8 years of age; 2) patients who had bilateral limbal stem cell deficiency or had allogeneic limbal transplantation; 3) patients who had limbal transplantation for partial limbal stem cell deficiency or limbal stem cell deficiency attributable to causes other than ocular surface burns; 4) patients with stable corneal epithelium but with <1 year of follow-up; 5) patients with total limbal stem cell deficiency but with dry eye disease (Schirmer test without anesthesia of <10 mm in 5 minutes); 6) patients with no visual potential as determined by clinical examination and electrophysiological testing (flash visual evoked potential and flash electroretinogram); and 7) patients with untreated concurrent ocular problems, such as entropion, trichiasis, lagophthalmos, glaucoma, and infection, were not considered for surgery.
Data Collection
The data retrieved from the medical records included age and sex of the patient, type and date of injury, details of prior ocular procedures, Snellen best spectacle-corrected visual acuity (BCVA) and intraocular pressure at presentation and at each follow-up visit, presence or absence of lid abnormalities, dry eye disease, symblepharon, degree of limbal involvement, intraoperative surgical details, postoperative complications, duration of follow-up, and status of ocular surface at each visit (slit-lamp findings including fluorescein staining).
Primary Outcome Measure
The primary outcome measure was the success of repeat limbal transplantation, defined clinically as a completely epithelialized, avascular, and clinically stable corneal surface. Failure or recurrence of limbal stem cell deficiency was defined as the occurrence of superficial corneal vascularization, persistent corneal epithelial defects, or conjunctivalization of the corneal surface. Survival time was calculated in months from the date of repeat limbal transplantation to the date of failure or the date of last follow-up depending on the clinical outcome.
Secondary Outcome Measures
The secondary outcome measures were: 1) the proportion of recipient eyes that had a 2-line improvement in BCVA at last follow-up or before undergoing keratoplasty as compared to baseline (before repeat surgery); 2) change in the BCVA in the donor eyes, before and after repeat limbal biopsy; and 3) intraoperative and postoperative complications of both repeat limbal biopsy and transplantation.
Technique of Limbal Biopsy
A repeat biopsy was taken from a healthy part of the limbus, which could be adjacent to but not inclusive of the area of previous biopsy; a 2 × 2-mm piece of conjunctival epithelium with 1 mm into clear corneal stromal tissue at the limbus was dissected; conjunctiva was excised just behind the pigmented line (palisades of Vogt); and the limbal tissue that contained epithelial cells and a part of the corneal stroma was obtained.
Technique of Limbal Culture
The tissue was transported to the laboratory in human corneal epithelium (HCE) medium. HCE is composed of modified Eagle’s medium/F12 medium (1:1) solution containing 10% (vol/vol) autologous serum (AS), 2 mM L-glutamine, 100 U/mL penicillin, 100 μg/mL streptomycin, 2.5 μg/mL amphotericin B, 10 ng/mL human recombinant epidermal growth factor, and 5 μg/mL human recombinant insulin. Under strict aseptic conditions, the donor limbal tissue was shredded into small pieces. Human amniotic membrane (hAM), prepared and preserved by our eye bank, was used as a carrier. A 3 × 4-cm hAM sheet was de-epithelialized using 0.25% recombinant trypsin and EDTA solution for 15 minutes. The shredded bits of limbal tissue were explanted over the center of de-epithelialized hAM with the basement membrane side up. A similar parallel culture was also prepared as a back-up. A submerged explant culture system without a feeder-cell layer was used. We used the HCE medium to nurture the culture. The culture was incubated at 37 C with 5% CO 2 and 95% air. The growth was monitored daily under an inverted phase contrast microscope and the medium was changed every other day. The culture was completed when a monolayer of the cells growing from the explants became confluent, typically in 10 to 14 days.
Technique of Limbal Transplantation
Any symblepharon that prevented adequate separation of the lids was released to permit the insertion of a wire speculum (no additional surgery to treat the symblepharon was performed). A peritomy was performed and the corneal fibrovascular pannus was excised. If excessive corneal thinning or perforation was noted at this stage a lamellar or penetrating keratoplasty was performed. The hAM and monolayer of cultivated limbal epithelial cells was spread over the cornea, epithelial side up. The graft was then secured to the peripheral cornea by interrupted, circumferential 10-0 nylon sutures and to the surrounding conjunctival edge by interrupted 8-0 polyglactin sutures. Alternately, using a sutureless technique, the graft was secured to the underlying ocular surface with fibrin glue (TISSEEL Kit; Baxter AG, Vienna, Austria) and the margins of the graft were tucked under the surrounding conjunctival edge. Bandage contact lenses were not applied at the end of surgery.
Postoperative Management
The postoperative regimen for limbal biopsy and transplantation was similar. All patients were treated with 1% prednisolone acetate eye drops 8 times a day tapered to once a day in 35 to 42 days and 0.3% ciprofloxacin hydrochloride eye drops 4 times a day for 1 week. The latter were continued, as needed, if an epithelial defect was present. No systemic antibiotics or steroids were administered to any patients. Patients were examined on postoperative days 1, 7, 42, and 90 and at an interval of 90 to 180 days thereafter, as customized by the clinical appearance of the transplant. Each examination included a complete history, visual acuity assessment with Snellen charts, intraocular pressure measurement, and detailed ocular examination of both eyes with slit-lamp biomicroscopy.
Statistical Analysis
MedCalc statistical software (version 11.4.3.0; Mariakerke, Belgium) was used for data analysis. The efficacy of transplantation was analyzed using Kaplan-Meier survival curves and survival probability/rate, reported as percentage (± standard error). A multivariate Cox proportional hazards model with stepwise elimination using Akaike information criterion (AIC) was designed (after checking the assumptions and interactions of the model) to test the association between graft failure and clinical variables. Change in BCVA before and after limbal biopsy and transplantation was analyzed using the Wilcoxon signed rank test for paired nonparametric data. A 2-tailed P value of less than .05 was considered statistically significant.
Results
Patient Demographics
This study included 50 of the 58 patients with failed primary autologous cultivated limbal epithelial transplantation performed for unilateral limbal stem cell deficiency following ocular burns. Eight patients declined the option of a second surgery. The mean age of the patients included in this study was 20.7 ± 11.4 (range 8 to 60) years and the male-to-female ratio was 7:3. The Table summarizes the baseline demographic features of all 50 cases and individual details are provided in the Supplemental Table (available at AJO.com ). Although 13 of the 50 fellow eyes (26%) had history of simultaneous injury, none had clinical features of ocular surface disease at presentation or just prior to repeat limbal biopsy. The mean follow-up was 2.3 ± 1.4 (median: 1.96, range: 1 to 7.5) years. All 50 patients had follow-up of 1 year; 25, 14, 10, 2, 2, and 1 patients had follow-up of 2, 3, 4, 5, 6, and 7 years respectively.
| Characteristic | n (%) |
|---|---|
| Laterality | |
| Right eye | 27 (54) |
| Left eye | 23 (46) |
| Etiology of ocular burn | |
| Alkali | 42 (84) |
| Acid | 6 (12) |
| Thermal | 1 (2) |
| Unknown chemical | 1 (2) |
| Ocular surgery prior to limbal transplantation | |
| Amniotic membrane graft | 34 (68) |
| Penetrating or lamellar keratoplasty | 15 (30) |
| Symblepharon release | 3 (6) |
| Entropion correction | 5 (10) |
| Tarsorrhaphy | 2 (4) |
| Tissue adhesive application | 5 (10) |
| Cataract extraction | 1 (2) |
| Best-corrected visual acuity before repeat limbal transplantation | |
| Better than 20/200 | 10 (10) |
| 20/200 or worse | 40 (80) |
| Lid abnormalities requiring correction before repeat limbal transplantation | |
| Upper lid entropion | 2 (4) |
| Lower lid entropion | 3 (6) |
| Trichiasis | 3 (6) |
| Incomplete lid closure | 2 (4) |
| Symblepharon present in at least 1 quadrant | 34 (68) |
| Duration between primary and repeat limbal transplantation | |
| 3 to 6 months | 20 (40) |
| More than 6 months to 1 year | 15 (30) |
| More than 1 year | 15 (30) |
| Type of surgery performed | |
| Repeat limbal transplantation | 42 (84) |
| Repeat limbal transplantation with lamellar or penetrating keratoplasty | 8 (16) |
Primary Outcome
At last follow-up visit, 33 of the 50 transplanted eyes (66%) maintained a completely epithelialized, avascular, and clinically stable corneal surface. The Kaplan-Meier survival rate at 1 year was 70% ± 6% and at 2 years and thereafter was 63.7% ± 7% ( Figure 2 ) . On multivariate analysis, eyes with symblepharon (hazard ratio: 6.7, 95% CI: 1.6 to 28, P = .0095) and eyes with simultaneous PK and limbal transplantation (hazard: 5.75, 95% CI: 1.3 to 24.6, P = .019) were found to be at greater risk of failure of repeat limbal transplantation; but there was no significant association seen with age, sex, etiology of injury, duration between injury and repeat surgery, duration between primary and repeat surgery, prior corneal transplantation, prior amniotic membrane grafting, presence of lid abnormalities, prior lid surgeries, and presenting vision.
Secondary Outcomes
Of the 50 recipient eyes, a 2-line improvement in final BCVA was seen in 38 (76%). At last follow-up visit or before undergoing keratoplasty, 22 eyes (44%) had BCVA of 20/60 or better, 18 (36%) had BCVA of 20/70 to 20/200, and 10 (20%) had BCVA worse than 20/200. Of the 10 eyes with BCVA of less than 20/200, 9 had poor vision attributable to recurrence of limbal stem cell deficiency and 1 eye had corneal scarring for which penetrating keratoplasty (PK) was done subsequently. Compared to baseline, there was a significant improvement in the median BCVA of recipient eyes at 1 week ( P < .0001), 6 weeks ( P < .0001), 3 months ( P < .0001), 6 months ( P < .0001), and 1 year ( P < .0001) post–repeat transplantation ( Figure 3 ) . In the donor eyes ( Figure 3 ), compared to baseline, there was no significant change in the BCVA at 1 week ( P = .11), 6 weeks ( P = .83), 3 months ( P = .37), 6 months ( P = .54), and 1 year post–repeat biopsy ( P = .49).
No intraoperative complications were noted during limbal biopsy; the only postoperative complication noted was subconjunctival hemorrhage adjacent to the donor site in 13 of the 50 cases (26%). Complete epithelialization of the donor site was seen in all cases by 14 days (or the day of limbal transplantation in the affected eye; Figure 4 ) . None of the donor eyes developed clinical features of limbal stem cell deficiency or conjunctival overgrowth at the site of repeat limbal biopsy.
No intraoperative complications occurred during repeat limbal transplantation. The most common post-transplantation complication was hemorrhage under the graft ( Figure 1 ), seen in 23 of 50 eyes (46%), which spontaneously resolved by 3 to 4 weeks. Recurrence of limbal stem cell deficiency occurred in 17 of the 50 transplanted eyes (34%). Fifteen cases (88.2%) recurred within 1 year, 13 (76.9%) within 9 months, and 10 (58.8%) within 6 months of repeat limbal transplantation. Seven of the 17 eyes (41.2%) developed persistent epithelial defects, among which 1 eye had a secondary corneal infection with Streptococcus pneumoniae and required an emergency therapeutic keratoplasty for corneal melting and perforation. Three eyes (4.5%) had recurrence of symblepharon that was encroaching onto the cornea. Corneal allografts failed in 4 of the 8 eyes that underwent simultaneous corneal and limbal transplantation.
Results
Patient Demographics
This study included 50 of the 58 patients with failed primary autologous cultivated limbal epithelial transplantation performed for unilateral limbal stem cell deficiency following ocular burns. Eight patients declined the option of a second surgery. The mean age of the patients included in this study was 20.7 ± 11.4 (range 8 to 60) years and the male-to-female ratio was 7:3. The Table summarizes the baseline demographic features of all 50 cases and individual details are provided in the Supplemental Table (available at AJO.com ). Although 13 of the 50 fellow eyes (26%) had history of simultaneous injury, none had clinical features of ocular surface disease at presentation or just prior to repeat limbal biopsy. The mean follow-up was 2.3 ± 1.4 (median: 1.96, range: 1 to 7.5) years. All 50 patients had follow-up of 1 year; 25, 14, 10, 2, 2, and 1 patients had follow-up of 2, 3, 4, 5, 6, and 7 years respectively.
| Characteristic | n (%) |
|---|---|
| Laterality | |
| Right eye | 27 (54) |
| Left eye | 23 (46) |
| Etiology of ocular burn | |
| Alkali | 42 (84) |
| Acid | 6 (12) |
| Thermal | 1 (2) |
| Unknown chemical | 1 (2) |
| Ocular surgery prior to limbal transplantation | |
| Amniotic membrane graft | 34 (68) |
| Penetrating or lamellar keratoplasty | 15 (30) |
| Symblepharon release | 3 (6) |
| Entropion correction | 5 (10) |
| Tarsorrhaphy | 2 (4) |
| Tissue adhesive application | 5 (10) |
| Cataract extraction | 1 (2) |
| Best-corrected visual acuity before repeat limbal transplantation | |
| Better than 20/200 | 10 (10) |
| 20/200 or worse | 40 (80) |
| Lid abnormalities requiring correction before repeat limbal transplantation | |
| Upper lid entropion | 2 (4) |
| Lower lid entropion | 3 (6) |
| Trichiasis | 3 (6) |
| Incomplete lid closure | 2 (4) |
| Symblepharon present in at least 1 quadrant | 34 (68) |
| Duration between primary and repeat limbal transplantation | |
| 3 to 6 months | 20 (40) |
| More than 6 months to 1 year | 15 (30) |
| More than 1 year | 15 (30) |
| Type of surgery performed | |
| Repeat limbal transplantation | 42 (84) |
| Repeat limbal transplantation with lamellar or penetrating keratoplasty | 8 (16) |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


