Meniere disease is one of the most fascinating and most vexing of all clinical conditions encountered by the otolaryngologist. Operationally speaking, a Meniere ear is a fragile ear. In fact, Meniere disease can and should be redefined as a degenerating inner ear that has impairment of one or more homeostatic systems, resulting in instability of hearing and balance function. This updated definition is a valuable guide to the clinical epidemiology and presentation of Meniere disease and to understanding the effects of conservative treatments. In the absence of a definitive test for Meniere disease, the greatest challenge for the clinician may be differentiating this condition from migraine. Ultimately, Meniere vertigo attacks are controllable in more than 99% of cases, but hearing loss and other auditory symptoms tend to be unresponsive to treatment.
Meniere’s disease is one of the most fascinating and most vexing of all clinical conditions encountered by the otolaryngologist. Despite having captivated the interest of clinicians and researchers for a century and a half and thousands of papers having been written about it, the causes, pathophysiology, and treatments of Meniere’s disease are not completely understood. Nonetheless, there is merit in occasionally taking inventory of the many findings and developments in inner ear research to update our thinking about this disorder of hearing and balance.
Toward a modern definition of Meniere’s disease
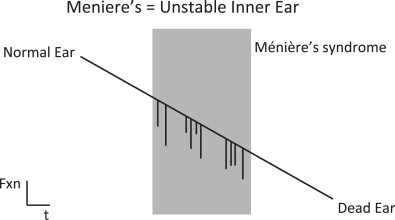
The nomenclature of Meniere’s “disease” versus Meniere’s “syndrome” in the otolaryngology literature is confusing enough and is not revisited here. Meniere’s disease is a “phenotype”; that is, it is a clinical presentation of unstable hearing and balance that may arise from many different insults to the inner ear. There is compelling evidence that it can arise from genetic factors, inflammatory and immunologic dysfunction, infection, trauma, and vasculopathy. Disturbances of barometric pressure, osmotic pressure, hydrostatic pressure, and perfusion pressure have all been incriminated at one time or another as factors in Meniere’s disease. A normal ear has a host of homeostatic systems. These systems regulate the production, maintenance, and recycling of endolymph and perilymph. They regulate efferent and afferent nerve signaling, efferent and afferent blood flow, intercellular signaling, ion cycling, mitochondrial energy metabolism, and other processes. Under normal circumstances, these homeostatic systems are so robust that inner ear functions of hearing and balance are impervious to changes in the rest of the body or the external environment. In Meniere’s disease one or more of these systems is dysfunctional. As a consequence of impaired homeostasis, hearing and balance functions become vulnerable to myriad internal and external factors, such as stress, sleep deprivation, dietary indiscretion, hormonal change, allergies, and barometric pressure change. Operationally speaking, a Meniere’s ear is a fragile ear. In fact, Meniere’s disease can and should be redefined as a degenerating inner ear that has impairment of one of more homeostatic systems resulting in instability of hearing and balance function ( Fig. 1 ).
Application of the modern definition of Meniere’s disease—diagnosis
There are 2 reasons to assign a patient’s condition a specific diagnosis: (1) to guide treatment and (2) to prognosticate. The American Academy of Otolaryngology–Head and Neck Surgery (AAO-HNS) Hearing and Equilibrium Subcommittee has published guidelines for the classification and reporting of Meniere’s disease treatment outcomes. These guidelines specify character, frequency, and duration of vertigo attacks necessary to achieve a diagnosis of Meniere’s disease. These guidelines have been updated periodically, with the last update in 1995. Although adoption of standardized diagnostic and reporting criteria are essential in research studies, one can afford to be somewhat less dogmatic in routine clinical practice. The 2 critical features of the Meniere’s phenotype that enable diagnosis are (1) instability and (2) involvement of both hearing and balance. Patients with isolated hearing instability or isolated vestibular symptoms do not meet Meniere’s diagnostic criteria. The old nomenclature of “cochlear Meniere’s” and “vestibular Meniere’s” was abandoned with the 1985 update of AAO-HNS criteria because there is insufficient evidence that these entities share essential pathophysiology with Meniere’s disease and because many such patients never meet Meniere’s criteria for involvement of auditory and vestibular systems.
Patients with Meniere’s disease exhibit huge variability in symptoms, within and between patients. Symptoms may occur in clusters or sporadically. Patients may have a great deal of hearing fluctuation or rapid loss but relatively infrequent vertigo (“auditory dominant” pattern), frequent and severe vertigo attacks but only mild hearing loss or infrequent fluctuations (“vestibular dominant” pattern), or auditory and vestibular symptoms that occur together or with relatively equal frequency and severity (“mixed” pattern). Although these patterns seem evident clinically, they have never been characterized epidemiologically. It is not known if there are 3 distinct pattern classes or a continuum. Nor is it known if patients remain “true to class” over time or if they transition from one class to another. If there are class transitions, it is not known if all patients pass through the classes in the same order. It is also not known if these different pattern classes indicate specific underlying pathophysiologic mechanisms or causes. The current best practice is to consider patients with combined auditory and vestibular instability to be patients with Meniere’s disease and treat them accordingly.
Application of the modern definition of Meniere’s disease—diagnosis
There are 2 reasons to assign a patient’s condition a specific diagnosis: (1) to guide treatment and (2) to prognosticate. The American Academy of Otolaryngology–Head and Neck Surgery (AAO-HNS) Hearing and Equilibrium Subcommittee has published guidelines for the classification and reporting of Meniere’s disease treatment outcomes. These guidelines specify character, frequency, and duration of vertigo attacks necessary to achieve a diagnosis of Meniere’s disease. These guidelines have been updated periodically, with the last update in 1995. Although adoption of standardized diagnostic and reporting criteria are essential in research studies, one can afford to be somewhat less dogmatic in routine clinical practice. The 2 critical features of the Meniere’s phenotype that enable diagnosis are (1) instability and (2) involvement of both hearing and balance. Patients with isolated hearing instability or isolated vestibular symptoms do not meet Meniere’s diagnostic criteria. The old nomenclature of “cochlear Meniere’s” and “vestibular Meniere’s” was abandoned with the 1985 update of AAO-HNS criteria because there is insufficient evidence that these entities share essential pathophysiology with Meniere’s disease and because many such patients never meet Meniere’s criteria for involvement of auditory and vestibular systems.
Patients with Meniere’s disease exhibit huge variability in symptoms, within and between patients. Symptoms may occur in clusters or sporadically. Patients may have a great deal of hearing fluctuation or rapid loss but relatively infrequent vertigo (“auditory dominant” pattern), frequent and severe vertigo attacks but only mild hearing loss or infrequent fluctuations (“vestibular dominant” pattern), or auditory and vestibular symptoms that occur together or with relatively equal frequency and severity (“mixed” pattern). Although these patterns seem evident clinically, they have never been characterized epidemiologically. It is not known if there are 3 distinct pattern classes or a continuum. Nor is it known if patients remain “true to class” over time or if they transition from one class to another. If there are class transitions, it is not known if all patients pass through the classes in the same order. It is also not known if these different pattern classes indicate specific underlying pathophysiologic mechanisms or causes. The current best practice is to consider patients with combined auditory and vestibular instability to be patients with Meniere’s disease and treat them accordingly.
Application of the modern definition of Meniere’s disease—treatment
Traditionally, Meniere’s disease has been treated with dietary restriction of sodium, caffeine, and alcohol; with diuretics; and with invasive procedures. Since Hallpike and Cairns and Yamakawa first reported endolymphatic hydrops in postmortem examination of temporal bones of patients with Meniere’s disease, there was a presumption that endolymphatic hydrops caused the fluctuating progressive hearing loss and vertigo attacks of Meniere’s disease. Recommendation to restrict sodium intake was originally conceived as a way of reducing “fluid retention” in the inner ear. Although this notion might seem simplistic and improbable, the fact is that many patients with Meniere’s disease are sensitive to sodium intake and do better on a restricted diet. Likewise, diuretics were first proposed to reduce endolymph volume. It is impossible to imagine that someone on a diuretic is urinating endolymph, but many patients with Meniere’s disease seem to improve on diuretic therapy. The modern definition of Meniere’s disease offers an explanation. A normal ear has homeostatic mechanisms that keep the fluid and electrolyte status of the inner ear tightly controlled and stable. A Meniere’s ear has lost this regulatory control. Diet and diuretic therapy place the responsibility for regulatory control in the patient’s hands and are means of pampering the fragile ear. A fragile ear may be intolerant of variations in sodium levels. If so, it is likely that a low sodium level is not actually the important feature of treatment. A constant sodium level is the critical feature. By evening out sodium intake across the day, patients reduce the risk of spikes that trigger symptoms. Although a very low sodium diet will achieve even distribution through the day, an even distribution can also be maintained on a “no added salt” (NAS) diet of 2000 to 3000 mg sodium per day. A target of 500 to 1000 mg of sodium per meal is relatively easy to achieve. Patient compliance is much better on the NAS diet than on a more severe restriction. There is an additional benefit of the more modest sodium restriction. If a patient is used to an extremely low sodium diet, a single handful of potato chips may double their day’s sodium intake, a spike that could easily trigger an attack. Alternatively, if the patient is equilibrated on the NAS diet of 1000 mg/meal, that same handful of chips may be only a 25% to 30% increase rather than 100% increase in daily sodium. The spike is relatively smaller and thus less likely to trigger symptoms.
Perspiring and subsequent fluid replacement is another potential source of inner ear stress that could trigger Meniere’s attacks. Maintenance of a stable fluid and electrolyte status is a primary objective in this updated approach to Meniere’s management. Therefore, in our clinic we stress that when patients with Meniere’s disease perspire, it is important that they actively replace their fluid loss with a sports drink or other electrolyte solution. The patients are perspiring saltwater, which must be replaced with something comparable. Patients are advised to sip the replacement solution frequently as they perspire, rather than dehydrating for an hour and then replacing with a single large bolus of fluid. For a 75-kg man perspiring freely, replacement rate is approximately 1 L/h. Sodium intake during fluid replacement while perspiring is not counted in the day’s total because it is canceled out by the loss through perspiration.
Caffeine and alcohol cause large fluid shifts through physiologic fluid compartments. Limiting their use to no more than a single “dose” per day is another way to keep the inner ear stable and avoid triggering an attack. Diuretics affect ion pumps and ionic gradients in the ear as well as in the kidney. It is likely that diuretic therapy in Meniere’s disease works via its influence on inner fluid and electrolyte processing and not by dehydrating the inner ear through inducing urination of endolymph. The guiding principle in all the conservative medical treatments with dietary restrictions, fluid replacement, and diuretics is to reduce stress on the inner ear’s fluid and electrolyte status so that it can retain a sufficient degree of stability.
Many of the other triggers for Meniere’s attacks, such as stress, hormonal change, barometric pressure change, sleep deprivation, and allergy attacks, can all be seen as challenges to the homeostasis of the fragile Meniere’s ear. Thus, patients with Meniere’s disease seem to do best if they have a regular daily routine, with meals at the same time each day, plenty of sleep, and some regular exercise. Patients with Meniere’s disease also do better if they have good general health and if they work with their primary care physician and other doctors to manage any other health issues. Common general health issues whose management often benefits the patient with Meniere’s disease include sleep disorders, allergies, thyroid dysfunction, diabetes, and perimenstrual or peripmenopausal hormonal fluctuations.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


