Purpose
To describe the determinant clinical signs to diagnose diffuse unilateral subacute neuroretinitis (DUSN) and the main features related to identification of the live worm.
Design
Retrospective study performed at the Federal University of Rio Grande do Norte, Rio Grande do Norte, Brazil, between 2003 and 2008.
Methods
Patients with early- or late-stage diffuse unilateral subacute neuroretinitis were included. All patients underwent complete ophthalmologic examination and had a minimum of 6 months of follow-up.
Results
A total of 121 patients were included. Most patients were younger than 20 years (69.42%). Visual acuity was 20/400 or worse in 86 patients (71.7%). Nine patients (7.43%) presented in the early stage and 112 (92.57%) patients presented in the late stage. Subretinal tracks (91.7%), focal alterations of the retinal pigment epithelium (89.3%), small white spots (80.2%), and optic nerve atrophy (76.9%) were the most frequent clinical features. The subretinal worm was identified in 48 patients (39.66%), and laser treatment to destroy it was performed in all cases. The most common location of the nematode was the posterior pole (21 patients). It was observed that the younger the age, the higher the indices of larvae identification ( P = .022). Multifocal yellow-white lesions and vitritis were correlated with identification of the worm ( P = .001). Mean logarithm of the minimal angle of resolution visual acuity was 1.466 (20/600) and 1.281 (20/400) before and after laser treatment, respectively ( P < .005).
Conclusions
Identification of clinical signs and diagnosis of diffuse unilateral subacute neuroretinitis in its early stage, followed by prompt location and destruction of the worm by photocoagulation, may improve the vision of affected patients.
Diffuse unilateral subacute neuroretinitis (DUSN) is an infectious ocular disease caused by an unidentified motile nematode capable of infiltrating the subretinal space, causing inflammation and retinal degeneration that leads to profound vision loss. The disease can affect children and young adults without gender preference or systemic problems. It is usually unilateral and occasionally is bilateral.
The presence of a nematode-related eye disease was first described by Wilder when examining the enucleated eye of a child with retinoblastoma. Gass and Scelfo described the natural history of ocular nematode infections observed in otherwise healthy young patients from the southern United States and the Caribbean. Later, Gass and associates named the syndrome DUSN after studying 36 cases and confirming the presence of a nematode in 2 patients. Different sized parasites and several species of nematodes have been reported as etiologic agents of DUSN, including Ancylostoma caninum and Baylisascaris procyonis , but most reports do not present evidence regarding the specific agent.
Clinical findings in patients with DUSN can be divided into 2 stages. The early stage is characterized by mild to moderate vitritis, mild optic disc edema, and recurrent crops of evanescent, multifocal, yellow-white lesions at the level of the outer retina and choroid. The late phase is characterized by optic nerve atrophy, retinal vessel narrowing, and focal or diffuse retinal pigment epithelium (RPE) degeneration marked by profound visual loss. The worm can be identified at any stage of the disease.
Photocoagulation is the treatment of choice for DUSN because it is an effective means of destroying the worm. Locating the nematode is a difficult and frequently frustrating task. Oral treatment with albendazole may be an alternative for patients in whom the worm is not identified and in whom photocoagulation cannot be performed.
The purpose of this study was to evaluate a large series of patients with DUSN and to identify the main clinical signs to diagnose and find a live worm.
Methods
This was a retrospective study assessing the clinical charts of patients diagnosed with DUSN between January 2003 and January 2008 in the Ophthalmology Department, Federal University of Rio Grande do Norte, Rio Grande do Norte, Brazil.
Patients in the early and late stages of the disease were included. Classification into early- or late-stage disease was based on clinical presentation according to the original description by Gass and Scelfo. Early-stage patients were characterized by decreased visual acuity (VA), papilitis, multifocal yellow-white lesions, vitritis, and vasculitis. In the late stage, they were characterized by decreased VA, mild vitritis, diffuse and focal RPE damage, optic nerve atrophy, and retinal vessel narrowing. Five additional signs observed in another case series were included in the statistics of this series: the presence of small white spots (probable exudation residue), external retinal edema, altered retinal internal limiting membrane reflex, focal hyperplasia of the RPE (resulted from pigment migration), and evidence of white subretinal tracks, suggesting remnants of larval migration in the subretinal space. Cases in which the worm was identified were defined as confirmed DUSN, and eyes with the above-mentioned clinical features, but without identification of the worm, were classified as presumed DUSN. The only exclusion criterion was the presence of any other ocular disease.
All patients underwent complete ophthalmologic examination, including best-corrected VA using the Snellen chart, subsequently transformed into logarithm of the minimal angle of resolution (logMAR) VA, slit-lamp examination, tonometry, fundoscopy using a 3-mirror Goldman lens or 78-diopter lens, and retinography. Fluorescein angiography was performed only in a sample of patients. Those included in the study had a minimum of 6 months follow-up.
After diagnosis of DUSN, patients were examined repeatedly in an attempt to locate the worm. Those identified with or without a worm were included in the study. Patients in whom the subretinal worm was identified were treated with laser photocoagulation. The following data were recorded and entered into an electronic database (SPSS; SPSS, Inc, Chicago, Illinois, USA): age, sex, best-corrected VA (Snellen chart modified to logMAR units) before and after treatment, affected eye, presence and location of a subretinal worm, and clinical signs of each case.
The primary outcome was to describe the occurrence rate of each clinical sign related to diagnosis of DUSN. Identification of clinical signs related to worm location and visual outcome in the treated eyes were considered secondary outcomes.
Statistical analysis was performed using the paired Student t test, the Pearson chi-square test, the Fisher exact test, and logistic regression analysis. Nominal P values are provided and were not corrected for multiplicity.
Results
A total of 121 patients were included in the study. Table 1 presents patient age, VA at presentation, and mean time from onset of symptoms to diagnosis. Mean age was 16.3 years (range, 5 to 43 years). Most patients were younger than 20 years (69.42%). There was no difference in gender commitment with 58 (48%) men and 63 (52%) women. Of 121 patients identified, 9 (7.4%) were diagnosed in the early stage of the disease and 112 (92.6%) were diagnosed in the late stage of the disease.
| Age at presentation (y) | |
| 5 to 10 | 19 cases (15.7%) |
| 11 to 15 | 28 cases (23.14%) |
| 16 to 20 | 37 case (30.58%) |
| > 20 | 37 cases (30.58%) |
| Visual acuity at presentation | |
| ≥ 20/40 | 10 cases (8.2%) |
| 20/60 ≤ VA ≥ 20/200 | 25 cases (20.66%) |
| < 20/200 | 86 cases (71.07%) |
| Mean time from onset of symptoms to presentation (range) | |
| Overall (early- and late-stage disease) | 3.4 mos (3 d to 9.5 mos) |
| Early-stage disease | 2.6 wks (3 d to 8 wks) |
| Late-stage disease | 4.1 mos (12 wks to 9.5 mos) |
Table 2 lists the occurrence of clinical signs in all patients diagnosed with DUSN, stratified into the prevalence of each clinical feature in patients in the early and late stages of the disease. Overall, the most prevalent clinical signs were the presence of subretinal tracks (91.7%), focal alterations of the RPE (89.3%), small white spots (80.2%), and optic nerve atrophy (76.9%). These clinical features also were the most prevalent in late-stage DUSN. All 9 patients in the early stage had yellow-white retinal lesions, vitritis, retinal edema, and vasculitis at presentation. Papillitis was present in 6 patients (66.7%), and in 1 patient, a macular star developed. A subretinal living worm was identified in 100% of the patients exhibiting clinical signs compatible with early-stage DUSN.
| Early- plus Late-Stage DUSN (121 Cases) | Early-Stage DUSN (9 Cases) | Late-Stage DUSN (112 Cases) | |
|---|---|---|---|
| Subretinal tracks | 111 (91.7%) | 0 (0%) | 111 (99.1%) |
| Focal alterations of the RPE | 108 (89.3%) | 0 (0%) | 108 (96.4%) |
| Small white spots | 97 (80.2%) | 0 (0%) | 97 (86.6%) |
| Optic disc atrophy | 93 (76.9%) | 0 (0%) | 93 (83%) |
| Altered ILM reflex | 68 (56.5%) | 0 (0%) | 68 (60.7%) |
| Vitreitis | 67 (55.4%) | 9 (100%) | 58 (51.7%) |
| Narrowed retinal vessels | 64 (52.9%) | 0 (0%) | 64 (57.1%) |
| Retinal edema | 58 (47.9%) | 9 (100%) | 49 (43.7%) |
| Live worm | 48 (39.66%) | 9 (100%) | 39 (34.8%) |
| Focal hyperplasia of the RPE | 35 (28.9%) | 0 (0%) | 35 (31.2%) |
| Yellow-white lesions | 17 (14%) | 9 (100%) | 8 (7.1%) |
| Vasculitis | 11 (9.1%) | 9 (100%) | 2 (1.8%) |
| Papillitis | 6 (5%) | 6 (66.7%) | 0 (0%) |
| Macular star | 1 (0.8%) | 1 (1.1%) | 0 (0%) |
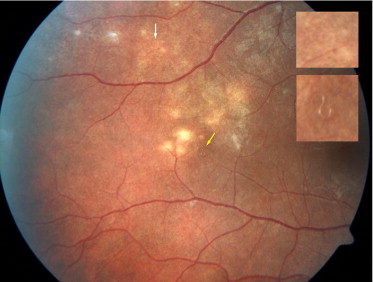
Figures 1 and 2 illustrate the most prevalent clinical signs of DUSN. Figure 1 shows the right eye of a 19-year-old woman with a 3-month history of VA loss. Multiple yellow-white retinal lesions can be observed temporal to the macula. A subretinal worm can be observed in the vicinity of these lesions (yellow arrow and bottom detail). A subretinal track also can be observed in the picture (white arrow and upper detail). Some degree of focal alteration of the RPE can be observed in the superior temporal region. Figure 2 shows different patients with classic clinical features of DUSN, such as optic nerve atrophy and retinal vessel narrowing (Top left), external retinal edema (Top right), focal hyperplasia of the RPE (Bottom left), and small white spots (Bottom right).

A subretinal motile live worm was identified in 48 patients (39.66%). The worm was identified in all early-stage patients and in 39 late-stage patients. The main worm location was the posterior pole (21 cases [43.75%]), followed by the temporal retina in 13 cases (27.08%), the nasal retina in 11 cases (22.91%), and the peripheral retina in 3 cases (6.25%).
All patients in whom the worm was identified were treated with photocoagulation to destroy it. Mean logMAR VA before and after laser treatment was 1.466 (Snellen equivalent, 20/600) and 1.281 (Snellen equivalent, 20/400), respectively. This improvement in VA was statistically significant ( P < .05).
Table 3 shows the occurrence rate of clinical signs in late-stage patients in whom the worm was identified (confirmed DUSN) compared with patients in whom it was not identified (presumed DUSN). With the exception of vitritis and the presence of yellow-white retinal lesions, the other clinical features had a similar occurrence rate in both groups. These results were statistically significant in relation to the presence of vitritis ( P = .001) and yellow-white retinal lesions ( P = .001) for identifying the subretinal worm.
| Worm Visualized | No Worm Visualized (73 Cases) | ||
|---|---|---|---|
| Early Stage (9 Cases) | Late Stage (39 Cases) | ||
| Subretinal tracks | 0 (0%) | 38 (97.4%) | 73 (100%) |
| Focal alterations of the RPE | 0 (0%) | 35 (89.7%) | 73 (100%) |
| Small white spots | 0 (0%) | 34 (87.17%) | 63 (86.3%) |
| Optic disc atrophy | 0 (0%) | 30 (76.9%) | 63 (86.3%) |
| Altered ILM reflex | 0 (0%) | 25 (64.1%) | 43 (58.9%) |
| Vitreitis | 9 (100%) | 30 (76.9%) | 28 (38.3%) |
| Narrowed retinal vessels | 0 (0%) | 21 (53.8%) | 43 (58.9%) |
| Retinal edema | 9 (100%) | 17 (43.6%) | 32 (43.8%) |
| Focal Hyperplasia of the RPE | 0 (0%) | 11 (28.2%) | 24 (32.8%) |
| Yellow-white lesions | 9 (100%) | 6 (15.38%) | 2 (2.7%) |
| Vasculitis | 9 (100%) | 2 (%) | 0 (0%) |
| Papillitis | 6 (66.7%) | 0 (0%) | 0 (0%) |
| Macular star | 1 (0.8%) | 1 (1.1%) | 0 (0%) |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


