Purpose
To investigate clinical characteristics of dry eye disease (DED) patients with a chronic pain syndrome.
Design
Cross-sectional study.
Methods
Four hundred twenty-five patients of a tertiary care DED patient cohort in the Netherlands were included. Chronic pain syndromes irritable bowel syndrome, chronic pelvic pain, and fibromyalgia were assessed by questionnaires. Outcome variables were the Ocular Surface Disease Index (OSDI) symptom questionnaire, tear osmolarity, Schirmer test, tear breakup time, conjunctival hyperemia, staining of the cornea and conjunctiva, and amount of mucus. Outcomes were cross-sectionally compared between DED patients with a chronic pain syndrome and those without.
Results
A total of 74 out of 425 DED patients (17%) had at least 1 chronic pain syndrome. The total symptom score was significantly higher in DED patients with a chronic pain syndrome than in those without (45.8 vs 33.8, P < .0005). Moreover, patients with a chronic pain syndrome scored higher on every single subscale of the 12-item OSDI symptom questionnaire. However, ocular signs were similar or even less severe in these patients. Similarly, in 64 DED patients from the population-based cohort TwinsUK, patients with a chronic pain syndrome (n = 24, 38%) had higher subscale and total (34.1 vs 14.4, P = .001) symptom scores.
Conclusion
In DED patients, chronic pain syndromes are common and are associated with increased severity of DED symptoms across all domains of the OSDI, even though objective ocular surface signs are no worse. In clinical practice, more awareness of chronic pain syndromes might help in understanding the discrepancy between signs and symptoms in DED.
Dry eye disease (DED) is a highly prevalent disorder and causes significant morbidity, with symptoms of pain, irritation, and interference with normal visual tasks. The poor correlation between symptoms and objective signs of the ocular surface disease hampers studies of DED and the management of patients with DED.
In a population-representative twin study, we recently reported that chronic pain syndromes are associated with DED. Consensus definitions are lacking, but chronic pain syndromes are often described as conditions with chronic pain of 1 or more body parts without obvious tissue-level pathology on adequate patient examination and absent abnormalities on routine investigation. Chronic pain syndromes include irritable bowel syndrome, chronic pelvic pain, and fibromyalgia (also known as chronic widespread pain syndrome). The exact mechanisms facilitating chronic pain syndromes have yet to be elucidated, but central sensitization and impaired descending pain modulation are generally believed to be underlying mechanisms causing widespread hypersensitivity to pain. We have shown not only that these disorders are associated with DED but also that they share underlying genetic factors with DED.
The purpose of this study is to investigate whether clinic-based DED patients with a chronic pain syndrome differ in ocular symptoms and signs from those without a chronic pain syndrome. In addition, we also investigated the differences in a population-based sample of DED patients.
Methods
Subjects
The GLOSSY (Groningen LOngitudinal Sicca StudY) cohort is a clinic-based cohort of dry eye patients from the tertiary dry eye clinic at the University Medical Center Groningen in the Netherlands. General and ophthalmic medical history, dry eye symptoms, dry eye test results using standardized methods, and dry eye therapies have been recorded longitudinally since September 2014, resulting in a clinical cohort with data on approximately 2000 patient visits a year. The University Medical Center Groningen is a national referral center for Sjögren disease and has a unique multidisciplinary approach to Sjögren disease, with regular examinations by rheumatologists, ophthalmologists, and oral surgeons. Consequently, approximately half of the patients visiting the tertiary dry eye clinic are Sjögren patients. All patients in the GLOSSY cohort have dry eye diagnosed by an ophthalmologist and/or were under the care of the multidisciplinary Sjögren disease service. The study was approved by the Institutional Review Board (IRB) of the University Medical Center Groningen and informed consent approval was not needed in this observational study. The research followed the tenets of the Declaration of Helsinki.
Assessment of Chronic Pain Syndromes
In the GLOSSY cohort the assignment of chronic pain syndromes was based on self-report by a questionnaire at baseline. Patients were asked the following question: “Have you ever been treated for or diagnosed by a physician as having …?” Fibromyalgia, chronic pelvic pain, and irritable bowel syndrome were among the list of many possible conditions patients were able to check, so the questionnaire did not appear to be specifically collecting chronic pain information.
Assessment of Dry Eye Outcomes
The study sample completed the Ocular Surface Disease Index (OSDI) at the beginning of their visit. The OSDI, developed by the Outcomes Research Group at Allergan Inc (Irvine, California, USA), is a 12-item questionnaire designed to provide a rapid assessment of the symptoms of ocular irritation consistent with dry eye disease and their impact on vision-related functioning. Presence of symptoms during the last week is rated per item on a 5-point scale (0-4) from “none of the time” to “all of the time.” The OSDI total score (ranging from 0 to 100) can be calculated with a formula using the sum score of all completed questions.
Dry eye tests were performed in both eyes in the following order: amount of conjunctival hyperemia, tear osmolarity, Schirmer value, visual acuity (Snellen), staining of the cornea with fluorescein, tear breakup time (TBUT), amount of mucus, and staining of the nasal and temporal conjunctiva with lissamine green. Conjunctival hyperemia was measured using the CCLRU grading system on a scale from 0 to 4 interpolated into increments of 0.5. Tear osmolarity was measured from the inferior lateral meniscus with a laboratory-on-a-chip by the TearLab Osmolarity System (TearLab Corporation; San Diego, California, USA) following standard protocols. An unanesthetized Schirmer-1 value after 5 minutes (mm/5 min) using sterile strips was measured in both eyes following standard protocols. Best-corrected visual acuity was measured in both eyes using a Snellen chart. For the statistical analysis the Snellen visual acuity was first transformed to a logMAR score. Staining of the cornea with fluorescein was performed using the Oxford Schema grading, ranging from grade 0 to 5, based on the number of punctate dots for the total exposed interpalpebral cornea. Staining of the conjunctiva with lissamine green was performed in a similar way using the Oxford Schema grading, scoring both the temporal and nasal zone and taking the sum of these scores per eye, ranging from 0 to 10. TBUT was measured by instilling a drop of fluorescein and counting the seconds after a blink before the tear film was broken up, following standard protocols. Each eye was measured 3 consecutive times and the average value per eye was used. The amount of mucus clumping per eye was scored as 0 (none), 1 (mild debris: mucus dots), 2 (moderate debris: mucus flocks), or 3 (mucus threads and filaments). Ophthalmologists that graded the dry eye were not aware of the study question and were not aware of the participants’ responses to questions about chronic pain syndromes.
Statistical Analysis
Data were cross-sectionally analyzed with the SPSS statistical package (version 22.0; SPSS, Inc, Armonk, NY). First, the demographics of the study sample was calculated. Second, outcome variables in patients with and without a chronic pain syndrome were calculated. The mean value of both eyes was taken for the analyses of all dry eye outcome variables. Since in both groups all symptoms and signs outcome variables turned out to have non-normal distributions, nonparametric Mann-Whitney U tests were used to test for a difference between groups. Additional similar analyses were performed looking at Sjögren and non-Sjögren DED patients separately. P < .05 was considered statistically significant in all analyses.
Population-Based Dry Eye Patients From the TwinsUK Cohort
In addition, to see whether results were similar in a population-based sample with less potential of ascertainment bias than a tertiary eye care clinic, we investigated DED patients from The TwinsUK Adult Twin Registry, held at King’s College, London, UK. This is a twin registry that has been ascertained from the general population through national media campaigns. Twins from this registry have been shown to be comparable to the age-matched general population singletons for a broad variety of medical and behavioral traits. A total of 606 female twin subjects that were included in a heritability study on DED were asked the following 2 questions in a questionnaire as proxy for having DED: “Have you ever been diagnosed (by a clinician) as having dry eye syndrome?” and “Do you currently use artificial tear eye drops or gel?” A strict definition of DED was applied to reduce the possibility of misclassification. If a participant answered “Yes” to both of these questions, she was assigned as having DED and subsequently included in this study. Local ethics committee (IRB) approval was obtained for the study, and twin volunteers gave informed consent but were unaware of the precise hypotheses being tested. The research followed the tenets of the Declaration of Helsinki. In this study sample classification of the different chronic pain syndromes was based on standard, validated criteria, per Vehof and associates. Three dry eye tests in the TwinsUK cohort were performed in both eyes in the following order: tear osmolarity, Schirmer value, and TBUT. The tests were all performed using standardized methods by the same trained research nurse. More information on how these tests were performed is provided by Vehof and associates.
Results
The first 425 consecutive DED patients from the GLOSSY cohort were included (85% female). Mean age (standard deviation [SD]) of the DED patients was 58.4 (15.7) years. Chronic pain syndromes were highly prevalent (17.4% [n = 74] having at least 1, 2.6% [n = 11] having more than 1), with irritable bowel syndrome (n = 40, 9.4%) and fibromyalgia (n = 38, 8.9%) most prevalent and chronic pelvic pain less prevalent (n = 7, 1.6%). Patients with a chronic pain syndrome did not have a different age than patients without a chronic pain syndrome (both groups 58.4 years, P = .98). Of patients with a chronic pain syndrome, 96% were female, compared to 83% of patients without a chronic pain syndrome ( P = .002, Fisher exact test).
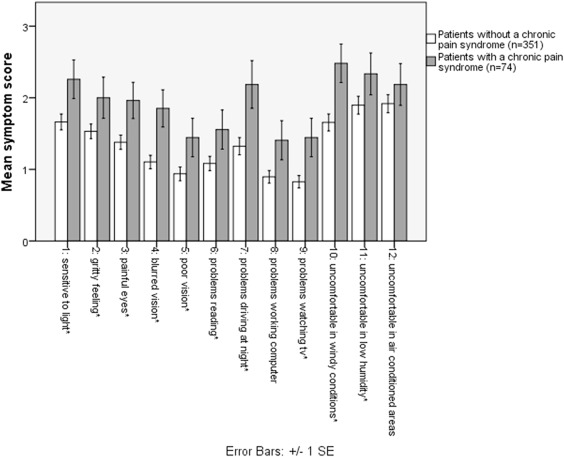
The OSDI total symptom score was significantly higher in chronic pain syndrome patients than in patients without a chronic pain syndrome (45.8 vs 33.8, P < .0005). Figure 1 shows the mean OSDI subscale scores separated in dry eye patients with and without a chronic pain syndrome. Interestingly, patients with a chronic pain syndrome scored higher on every single item of the 12-item OSDI symptom score, with 10 items being statistically significant. The higher symptom scores in DED patients with a chronic pain syndrome than in DED patients without a chronic pain syndrome were present in both Sjögren (n = 191, 12.0% having a chronic pain syndrome, OSDI total score 45.9 vs 34.2, P = .03) and non-Sjögren patients (n = 138, 13.8% having a chronic pain syndrome, OSDI total score 44.1. vs 33.9, P = .08).
The Table shows the measurements from the dry eye tests, again separated in DED patients with and without a chronic pain syndrome. Patients with a chronic pain syndrome scored as less severe on every dry eye test, although only corneal staining score and Schirmer score were statistically significantly different. In addition, there was a trend of less severe conjunctival staining and amount of mucus ( P < .10).
| Dry Eye Test | Patients With a Chronic Pain Syndrome (N = 74, 17%) | Patients Without a Chronic Pain Syndrome (N = 351, 83%) | Interpretation of Sign of Patients With vs Without a Chronic Pain Syndrome | P Value a for a Difference | ||
|---|---|---|---|---|---|---|
| Mean (SE) | Median Value | Mean (SE) | Median Value | |||
| Tear osmolarity (mOsm/mL) | 309.4 (1.9) | 308.0 | 311.6 (0.9) | 309.5 | Less severe | .45 |
| Conjunctival hyperemia (0-3) | 2.24 (0.08) | 2.5 | 2.35 (0.04) | 2.5 | Less severe | .14 |
| Schirmer value (mm) | n/a | 3.5 | n/a | 2.5 | Less severe | .048 |
| Visual acuity (Snellen) | 0.91 (0.03) | 0.95 | 0.87 (0.01) | 0.92 | Less severe | .23 |
| Corneal staining (0-5) | 1.01 (0.13) | 1.0 | 1.42 (0.07) | 1.5 | Less severe | .013 |
| Conjunctival staining (0-10) | 1.38 (0.22) | 1.0 | 2.14 (0.15) | 1.5 | Less severe | .06 |
| Tear breakup time (s) | 5.1 (0.4) | 5 | 4.7 (0.2) | 4 | Less severe | .35 |
| Mucus (0-3) | 0.51 (0.08) | 0.0 | 0.73 (0.05) | 0.5 | Less severe | .10 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


