Purpose
To examine the relationship of choroidal thickness with axial length (AL) and myopia in young adult eyes in the ethnically diverse Correction of Myopia Evaluation Trial (COMET) cohort.
Design
Cross-sectional, multicenter study.
Methods
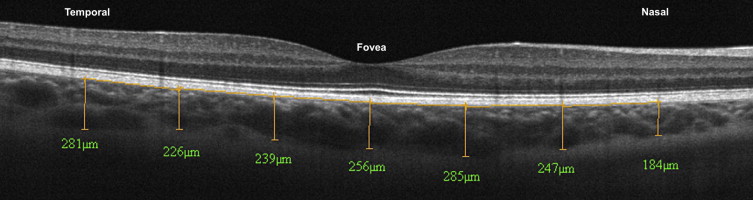
In addition to measures of myopia by cycloplegic autorefraction and AL by A-scan ultrasonography, participants underwent optical coherence tomography imaging of the choroid in both eyes at their last visit (14 years after baseline). Using digital calipers, 2 independent readers measured choroidal thickness in the right eye (left eye if poor quality; n = 37) at 7 locations: fovea and 750, 1500, and 2250 μm nasal (N) and temporal (T) to the fovea.
Results
Choroidal thickness measurements were available from 294 of 346 (85%) imaged participants (mean age: 24.3 ± 1.4 years; 44.9% male) with mean myopia of −5.3 ± 2.0 diopters and mean AL of 25.5 ± 1.0 mm. Overall, choroidal thickness varied by location ( P < .0001) and was thickest at the fovea (273.8 ± 70.9 μm) and thinnest nasally (N2250, 191.5 ± 69.3 μm). Multivariable analyses showed significantly thinner choroids in eyes with more myopia and longer AL at all locations except T2250 ( P ≤ .001) and presence of peripapillary crescent at all locations except T1500 and T2250 ( P ≤ .0001). Choroidal thickness varied by ethnicity at N2250 ( P < .0001), with Asians having the thinnest and African Americans the thickest choroids.
Conclusion
Choroids are thinner in longer, more myopic young adult eyes. The thinning was most prominent nasally and in eyes with a crescent. In the furthest nasal location, ethnicity was associated with choroidal thickness. The findings suggest that choroidal thickness should be evaluated, especially in the nasal regions where myopic degenerations are most commonly seen clinically.
The choroid, primarily a vascular structure, has several important functions in the eye, including delivery of blood and nutrients to the outer retina, thermoregulation of the retina, and secretion of growth factors (for a recent review see ). If the choroid is compromised, a loss of blood flow and oxygen to the retina can occur and ultimately lead to a variety of visually debilitating ocular diseases. In myopia, axial elongation of the eye can lead to choroidal degeneration and/or breaks in the Bruch membrane, clinically evident as lacquer cracks, chorioretinal atrophy, Fuchs spot, or myopic choroidal neovascularization. Further, the prevalence of myopia in the United States has increased in recent years to 40% of the population aged 12–54 years and is particularly high in Asian populations, where it reached levels as high as 95.5% in a population of Chinese university students. Given such ocular comorbidities and increasing prevalence in both the United States and Asia, a more complete characterization of the choroid in young adult myopic eyes is warranted.
The choroid has also been implicated in the modulation of eye growth in animals, owing to its rapid thinning in response to hyperopic defocus (image plane behind the retina), which, in coordination with increasing vitreous chamber depth, moves the retina toward the image plane. Similarly, in human eyes the choroid thins rapidly in response to hyperopic defocus imposed by a negative-powered lens or sustained accommodation. These responses occur within hours after the imposition of stimuli that, over sustained periods, produce axial elongation and, eventually, myopia. Given its unique position between the retina and sclera, the choroid may be a source of scleral growth regulators in response to such local visual stimuli, making it potentially important in emmetropization and axial elongation.
The advent of high-resolution spectral-domain optical coherence tomography (SD OCT) allows for the evaluation of choroidal thickness in vivo, which may provide important information about the possible role of the choroid in human myopia and the increased susceptibility of the myopic eye to ocular disease. In fact, human studies have found that thinner choroids are associated with higher amounts of myopia in adults and children. Only a few studies have investigated the association of choroidal thickness and axial length and report thinner choroids in longer eyes. Read and associates showed that the choroid of myopic children is thinner than that of nonmyopic subjects and suggested that the magnitude of this difference is greater than would be expected simply from axial elongation. However, many OCT studies have looked at choroidal thickness only centrally at the fovea, in older participants, and/or in non–ethnically diverse populations, and/or did not investigate the relationship of choroidal thickness with both refractive error and axial length or the presence of peripapillary crescent, typically an indicator of higher amounts of myopia. Therefore, a better understanding of the factors associated with choroidal thickness in young myopic eyes is needed.
The purpose of this study is to determine whether choroidal thickness at several locations surrounding the fovea is related to ethnicity, sex, presence of peripapillary crescent, axial length, and amount of myopia in a large cohort of myopic young adults, from the Correction of Myopia Evaluation Trial (COMET), in which over one quarter have high myopia (worse than −6.0 diopters [D]).
Subjects and Methods
The COMET study design and main treatment outcomes have been described previously. Briefly, the randomized multicenter clinical trial ( clinicaltrials.gov identifier at each of the clinical centers: NCT00000113 ) evaluated 2 lens treatments, single vision and progressive addition lenses, in a large, multiethnic group who were aged 6 to < 12 years with low to moderate myopia when they enrolled, and reported a statistically but not clinically significant treatment effect of 0.20 D after 3 years. COMET has continued as a longitudinal observational study of factors associated with myopia progression and stabilization. In the current analyses, data are combined for the 2 lens treatment groups. During the final study visit, the standard study protocol, including measurements of axial length and cycloplegic refractive error, was followed as described below and previously. In addition to these procedures, OCT imaging of the choroid was performed, as described below.
Participants
A total of 346 young myopic adults, aged 20.4–27.5 (mean: 24.2 ± 1.4) years old at their final study visit 14 years after baseline, had OCT imaging of the choroid performed at their respective clinical centers (optometry schools/colleges in Birmingham, Alabama; Boston, Massachusetts; Houston, Texas; and Philadelphia, Pennsylvania). The study protocols were HIPAA compliant and conformed to the Declaration of Helsinki and the institutional review boards at each participating center approved the research protocols. At study enrollment, informed consent was obtained from parents and assent from their children, after a written and verbal explanation of the clinical procedures. Participants were re-consented as adults at age 18 years and for additional measurements, described below.
Standard Study Procedures
As part of the COMET study protocol, refractive error and axial length were measured in all participants at each annual visit. Study optometrists who were certified on all procedures performed all measurements. Refractive error was measured 30 minutes after administration of a second drop of a cycloplegic agent (2 drops of 1% tropicamide, separated by 4–6 minutes), using an autorefractor (ARK-700A; Nidek, Gamagori, Japan). Five consecutive reliable measurements were taken in each eye and the mean cycloplegic refractive error, in terms of spherical equivalent, was calculated for each eye.
Axial length was measured by ultrasonography (A-2500; Sonomed, Lake Success, New York, USA) after a drop of anesthetic (1% proparacaine) was placed in each eye. Five consecutive measurements were taken, either using the slit-lamp (preferred technique) or handheld technique, in each eye. A standard deviation less than or equal to 0.10 mm between measurements was maintained for each eye. Mean axial length was then calculated for each eye from these measurements.
Optical Coherence Tomography Imaging
The SD OCT device (RTVue, Model RT-100; Optovue, Inc Fremont, California, USA) used in this study can capture 26 000 A-scans per second with a depth resolution of 5 μm using a scanning laser diode at a wavelength of 840 ± 10 nm. In COMET, OCT imaging was initially performed beginning in the 11th study year by the study optometrist in each participant’s right eye followed by the left eye, with natural pupils, unless the pupil size was smaller than 3 mm under dim illumination (n = 5). For these few participants, OCT imaging was performed with dilated pupils after all other ocular measurements were taken. No optical correction was used when images were taken. To improve image quality, all participants received 1 drop of an artificial tear with mild viscosity in each eye prior to imaging. In addition, fixation and blinks were monitored during all scans.
After imaging, the en face and cross-sectional scanning laser ophthalmoscopy images of the optic nerve (3D disc baseline registration scan) from all participants were evaluated by a trained study optometrist (E.H. or W.M.T.) for the presence or absence of a peripapillary crescent. A crescent, a common clinical observation in myopic patients, is defined as a retraction of the Bruch membrane complex from the optic nerve head margin. A crescent was graded as “present” if 2 conditions were met: (1) the crescent was observable beyond the previously verified disc margin in any location around the nerve on the en face image and (2) a corresponding increase in signal intensity from the underlying sclera in the crescent area on the cross-sectional image was observed.
At the final visit (14th study year), to investigate choroidal thickness, a 6-mm line scan (average of ≥25 B-scans), centered on the fovea, was taken in each eye. All scans were individually inspected at the time of measurement to ensure good image quality (signal strength index >50, with no breaks or shearing in the images) and were retaken, if necessary. The “auto-all focus” feature of the RTVue was used during all image acquisitions in an attempt to minimize any retinal magnification effects that might have occurred owing to differences in participants’ axial lengths. This feature automatically estimates the participant’s refraction, in diopters, and accordingly adjusts the system’s configuration to minimize magnification errors. In addition, a previous report using the same instrument and pilot testing of our data (n = 33) showed that no correction was necessary for possible magnification effects associated with increased axial length.
Measurement of Choroidal Thickness
Two masked independent readers at the IDEA Reading Center manually measured choroidal thickness (using the chorioscleral border) in the right eye (left eye if poor right eye quality [n = 37]). Choroidal thickness was measured with digital calipers available with RTVue software (version 6.10.100.22) at 7 locations: fovea and 750, 1500, and 2250 μm nasal (N) and temporal (T) to the fovea ( Figure 1 ). If at any 1 location the chorioscleral border was not visible to the grader, the remaining locations were still graded, if possible. For each location, the average of the 2 readers’ measurements was used, or the consensus value, if necessary. Consensus grading occurred if the 2 readers’ choroidal thickness differed by either 15% or 30 μm. This method of manual choroidal thickness measurement using digital calipers has been shown to be highly repeatable.
Statistical Analysis
All statistical analyses were performed using SAS version 9.3 (SAS Institute, Cary, North Carolina, USA). Participant demographic characteristics including sex and self-reported ethnicity, as well as ocular components, were each evaluated for associations with choroidal thickness measurements in all 7 locations using t tests (sex, axial length [median split], presence/absence of high myopia [worse than −6.0 D], presence/absence of crescent) and ANOVA tests (ethnicity). Pearson correlation coefficients were used to evaluate the relationship between choroidal thickness and axial length/spherical equivalent refraction as a continuous variable at each location. To account for the correlations among all the regions within the same participant, linear mixed models were then used to assess the effects of potential risk factors when the choroidal thicknesses of all regions were included as the outcome in the same model. Covariates under consideration for inclusion in the linear mixed models included sex, ethnicity, axial length (continuous), presence/absence of crescent, and spherical equivalent refraction. Owing to the collinearity between axial length and refraction, they were included separately in 2 different models. To achieve the most parsimonious model, final models were selected to include only the statistically significant factors (ethnicity, axial length or spherical equivalent refraction, presence/absence of crescent; P value < .05) and adjusted for multiple comparisons using Bonferroni correction. The adjusted parameter estimates and their standard errors from the models are presented along with the corresponding P values. Visual acuity and participant age were not evaluated for associations with choroidal thickness, given the narrow ranges in the cohort.
Results
Overall Results
Analyses were based on the 294 of 346 scans (85%) (3 were excluded owing to refractive surgery/missing data, 49 were not gradable at any location) that were gradable at at least 1 location in 1 eye. The mean (±standard deviation [SD]) refractive error of the participants with usable data was −5.3 (±2.0) D and the mean axial length was 25.5 (±1.0) mm. As shown in Table 1 , significant differences were found between the gradable and not gradable group by ethnicity, refractive error, and axial length, with the not gradable group generally having a higher percentage of African Americans ( P < .01), less myopia (mean difference = 0.8 D, P = .01), and shorter eyes (mean difference = 0.4 mm, P = .01). The percentage of scans needing adjudication in at least 1 location based on the previously defined criteria was 29% with the majority of adjudications occurring in the outer retinal locations. After adjudication, the interclass coefficients of choroidal thickness measurements between graders were >0.98 in all measured retinal locations (range = 0.98–0.99).
| Participant Characteristics | Scan Gradable (N = 294) | Scan Not Gradable (N = 49) | P Value |
|---|---|---|---|
| N (%) | N (%) | ||
| Sex | .59 a | ||
| Male | 132 (86.8) | 20 (13.2) | |
| Female | 162 (84.8) | 29 (15.2) | |
| Ethnicity | <.01 a | ||
| Asian | 29 (100) | 0 (0.0) | |
| Hispanic | 41 (93.2) | 3 (6.8) | |
| Mixed/other | 15 (83.3) | 3 (16.7) | |
| White | 142 (92.8) | 11 (7.2) | |
| African American | 67 (67.7) | 32 (32.2) | |
| Age (y) | .65 b | ||
| Mean (SD) | 24.3 (1.4) | 24.2 (1.4) | |
| Median (min, max) | 24.3 (20.7, 27.5) | 24.2 (20.4, 26.9) | |
| Refractive error (D) | .01 b | ||
| Mean (SD) | −5.3 (2.0) | −4.5 (1.9) | |
| Median (min, max) | −4.9 (−13.1, −0.9) | −4.1 (−9.4, −0.9) | |
| Axial length (mm) | .01 b | ||
| Mean (SD) | 25.5 (1.0) | 25.1 (0.9) | |
| Median (min, max) | 25.5 (22.0, 28.1) | 25.0 (23.3, 27.6) |
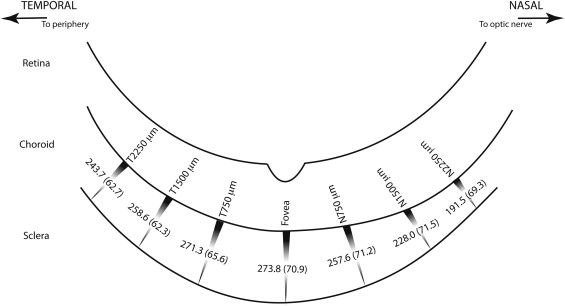
Overall, choroidal thickness varied across the 7 locations ( P < .0001) and was thickest at the fovea (mean ± SD: 273.8 ± 70.9 μm) and thinnest at N2250 (191.5 ± 69.3 μm), as demonstrated by the choroidal thickness profile diagram in Figure 2 . These data show significant nasal-temporal asymmetries in choroidal thickness in these young myopic eyes. On average, the nasal choroid thinned more rapidly than the temporal choroid at locations peripheral to the fovea. The difference between the choroidal thickness at the fovea and N2250 was 62.3 μm, which is about twice the difference in choroidal thickness between the fovea and T2250, a difference of 30.1 μm. The largest nasal-temporal difference in choroidal thickness was between N2250 (191.5 μm) and T750 (271.3 μm) (mean difference = 79.3 μm, P < .0001).
Ethnicity and Sex
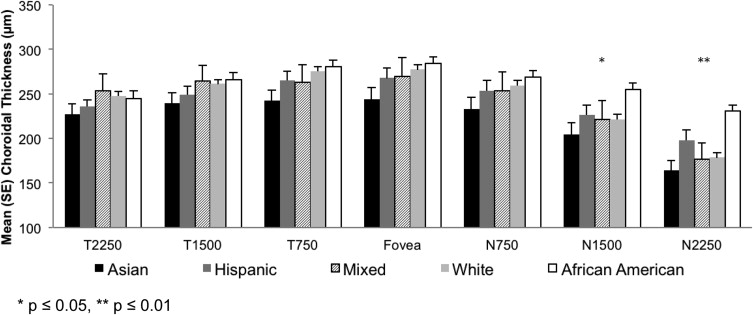
Overall, African Americans had the thickest choroids and Asians had the thinnest at all locations. However, ethnicity was only significantly associated with choroidal thickness in the furthest nasal locations (N1500, P ≤ .05 and N2250, P ≤ .01, Figure 3 ). In these locations, compared to African Americans, Asians had significantly thinner choroids (mean ± standard error at N1500 = 50.1 ± 15.7 μm thinner, P < .01; at N2250 = 66.4 ± 14.7 μm thinner, P < .01). In addition, compared to African Americans, whites had significantly thinner choroids at N1500 (33.0 ± 10.5 μm thinner, P ≤ .01) and at N2250 Hispanics and whites had significantly thinner choroids (∼32–51 μm thinner, P ≤ .01). There were no sex differences in choroidal thickness at any of the 7 measured locations (range of mean difference between male and female subjects: −5 to 5 μm, P ≥ .47 at each location).
Axial Length and Presence of High Myopia
Longer eyes, based on a median split of participants’ axial length (25.5 mm), had significantly thinner choroids at all retinal locations ( P ≤ .01 at all locations except P < .05 at T2250, Figure 4 ). Likewise, those participants with high myopia worse than −6.0 D (n = 86, mean ± SD = −7.8 ± 1.4 D) had significantly thinner choroids at all retinal locations ( P ≤ .01, Figure 4 ), in comparison to those participants with lower amounts of myopia (n = 208, mean ± SD = −4.2 ± 1.1 D). The mean differences in choroidal thickness were similar in longer vs shorter eyes (range: 19–36 μm thinner) and high vs low myopia (22–40 μm thinner). These differences were generally more pronounced in the nasal vs temporal locations, as shown in Figure 4 .

Presence of Crescent
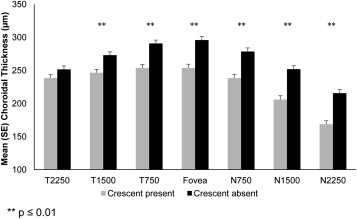
As mentioned earlier, each participant was evaluated for the presence or absence of crescent. The mean axial length and amount of myopia of participants who did have a crescent were longer/worse (25.7 mm/−5.7 D) than those who did not have a crescent (25.2 mm/−4.8 D). Therefore, participants with a crescent had significantly longer eyes (0.5 mm longer) and were more myopic by 0.9 D ( P < .0001 for both). The presence of a peripapillary crescent was also highly associated with thinner choroids. Specifically, eyes with a crescent had significantly thinner choroids compared to eyes without a crescent at all retinal locations measured (27–45 μm thinner, P < .0003), except the T2250 location, as shown in Figure 5 . Similar to the differences seen in choroidal thickness with and presence of high myopia, the largest differences between presence and absence of crescent were noted in the nasal locations.
Multivariable Analysis
A multivariable analysis (linear mixed model using axial length, presence or absence of crescent, and ethnicity as covariates) of the possible factors associated with choroidal thickness showed that longer axial length was significantly associated with thinner choroids ( P ≤ .001) at all except the furthest temporal location (T2250). In general, choroids were approximately 10–16 μm thinner per 1 mm increase in axial length, with the greatest slope occurring at the N1500 location (16.4 ± 4.0 μm thinner/1 mm increase, P < .0001). Similarly, the presence of crescent was significantly associated with thinner choroids ( P ≤ .0001) at all except the furthest temporal locations (T1500, T2250) ( Table 2 ). In this model, choroids were estimated to be 8–35 μm thinner in eyes with than without a crescent. When myopia was used instead of axial length as a covariate (data not shown), the findings were similar, with more myopia associated with thinner choroids ( P ≤ .004) at all locations.
| Location | Axial Length (mm) | Crescent | |||
|---|---|---|---|---|---|
| Model Estimate, μm (SE) | P Value b | Presence | Model Estimate, μm (SE) | P Value b | |
| T2250 (n = 291) | −9.7 (3.8) | .01 | Yes | −8.0 (7.7) | .30 |
| No | Reference | – | |||
| T1500 (n = 291) | −12.0 (3.7) | .001 ∗ | Yes | −19.7 (7.5) | .01 |
| No | Reference | – | |||
| T750 (n = 292) | −13.3 (3.8) | .0005 ∗ | Yes | −29.9 (7.7) | .0001 ∗ |
| No | Reference | – | |||
| Fovea (n = 294) | −14.3 (4.1) | .0005 ∗ | Yes | −34.7 (8.3) | <.0001 ∗ |
| No | Reference | – | |||
| N750 (n = 292) | −14.8 (4.1) | .0004 ∗ | Yes | −33.3 (8.4) | .0001 ∗ |
| No | Reference | – | |||
| N1500 (n = 292) | −16.4 (4.0) | <.0001 ∗ | Yes | −35.0 (8.2) | <.0001 ∗ |
| No | Reference | – | |||
| N2250 (n = 292) | −14.9 (3.8) | <.0001 ∗ | Yes | −33.7 (7.7) | <.0001 ∗ |
| No | Reference | – | |||
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


