Purpose
To examine choroidal thickness in nonarteritic anterior ischemic optic neuropathy (AION).
Design
Retrospective case control study.
Methods
In the eye clinic of the University Medical Center in Mannheim, Germany, we studied a group that consisted of patients with nonarteritic AION and a control group that consisted of individuals with normal fundus. Choroidal thickness was measured by the enhanced-depth imaging of spectral-domain optical coherence tomography. The main outcome measure was choroidal thickness.
Results
The study group consisted of 20 patients: 11 patients with acute nonarteritic AION and an unaffected contralateral eye and 9 patients with acute unilateral nonarteritic AION and previously nonarteritic AION in the contralateral eye. The control group consisted of 58 patients (58 eyes). In multivariate analysis, thinner subfoveal choroidal thickness was associated with the diagnosis of nonarteritic AION ( P = 0.001; regression coefficient B, −55.1), after adjusting for age ( P < 0.001) and refractive error ( P = 0.20). Similarly, unaffected eyes contralateral to eyes with acute nonarteritic AION as compared to control eyes showed thinner subfoveal choroidal thickness ( P = 0.037) after adjusting for age ( P = 0.001) and refractive error ( P = 0.06). In a reverse manner, nonarteritic AION was associated with thinner subfoveal choroidal thickness ( P = 0.007) after adjusting for age, optic disc diameter, gender, and refractive error.
Conclusions
Eyes affected by nonarteritic AION and unaffected contralateral eyes showed significantly thinner macular choroids than eyes of a control group after adjusting ocular and systemic parameters. A thin choroid may be added to the diagnostic features of nonarteritic AION. Future studies may examine the pathophysiologic meaning of the finding.
Since Spaide and colleagues reported on the visualization of the choroid by using the enhanced-depth imaging mode of spectral-domain optical coherence tomography, choroidal thickness has been measured in normal subjects and in patients with various diseases, such as polypoidal choroidal vasculopathy, central serous chorioretinopathy, chronic open-angle glaucoma, and chronic and acute angle-closure glaucoma.
None of the studies has addressed choroidal thickness in patients with nonarteritic anterior ischemic optic neuropathy (AION). Nonarteritic AION is a disease of the optic nerve head and is caused by a vascular insufficiency in the capillary bed of the optic disc. This capillary bed is fed by the large posterior choroidal arteries and the peripapillary arterial circle of Zinn-Haller surrounding the optic nerve head in the close vicinity of the choroidal vasculature. Because the choroidal vasculature and the vasculature of the optic nerve head are closely connected to each other, we conducted this study to measure the choroidal thickness at the posterior pole in patients with nonarteritic AION. Although the thickness of the whole choroid, including the choriocapillaris, the Sattler layer and the Haller layer, is clearly not a direct surrogate for choroidal blood flow, knowledge about whether nonarteritic AION is associated with an abnormally thick or thin choroid may help to better understand the pathogenesis and risk factors of nonarteritic AION.
Methods
The hospital-based retrospective observational study analyzed a study group of patients with nonarteritic AION and a control group of patients who attended the hospital for cataract surgery or reasons other than macular or retinal diseases. The ethics committee II of the Medical Faculty Mannheim of the University of Heidelberg approved the study according to the Declaration of Helsinki and all federal laws in Germany.
All study participants underwent a detailed ophthalmologic examination, including refractometry and measurement of best-corrected visual acuity, slit-lamp based examination of the anterior ocular segment, tonometry, and ophthalmoscopy. Subfoveal choroidal thickness (SFCT) was measured using spectral-domain optical coherence tomography (wavelength: 870 nm; Spectralis, Heidelberg Engineering, Heidelberg, Germany) with enhanced-depth imaging modality after pupil dilation. We obtained 9 horizontal optical coherent tomographic sections in a 15 × 30 rectangle centered on the fovea. The horizontal section running through the foveola was selected for further analysis. SFCT was defined as the vertical distance from the hyper-reflective line of the Bruch membrane to the hyper-reflective line of the inner surface of the sclera. The measurements were performed using the Heidelberg Eye Explorer software (v 5.3.3.0; Heidelberg Engineering). The images were taken by an experienced technician and were assessed by 3 experienced examiners (AKS, TMF, PS). The technician was unaware of the diagnosis, while the examiners were not masked when measuring choroidal thickness. Masking was difficult because the changes in the optic nerve head due to nonarteritic AION also led to changes in the macular region. The reproducibility of the technique had previously been examined and showed a relatively high repeatability (intraclass coefficient, 1.00; mean coefficient of variation, 0.85% ± 1.48%; Bland-Altman plot with 1.9% [61/3233] points outside the 95% limits of agreement). Using the infrared images of the optical coherent tomographic examination, we also measured the horizontal and vertical optic disc diameters.
Nonarteritic AION was characterized by an acute and painless loss of visual acuity and a sectoral visual field defect, often noted in the morning; a segmentally swollen and hyperemic optic disc, with the superior optic disc pole more often affected than the inferior pole; an erythrocyte sedimentation rate and serum concentration of the C-reactive protein within the age-adjusted normal ranges; an unremarkable finding of the superficial temporal artery by digital examination, by histologic examination after excision, or by sonography; and no other reason for an acute optic neuropathy. In the study group, optical coherence tomography was performed when patients had recently experienced the onset of nonarteritic AION, and it showed acute optic nerve head swelling. Several months prior to inclusion into the study, some patients in the study group had also suffered nonarteritic AION in the contralateral eye which, at the time of the examination, showed the typical sequelae of nonarteritic AION, such as segmental disc pallor and segmental loss of the retinal nerve fiber layer.
Statistical analysis was performed using a commercially available statistical software package (SPSS for Windows, v 21.0, IBM-SPSS, Chicago, Illinois, USA). For the patients in the study group, both eyes (affected eyes and unaffected eyes) were included in the study, whereas for the individuals in the control group, only the right eyes were included. As the first step in the statistical analysis, we calculated the mean values (presented as mean ± standard deviation) of the main parameters. As the second step, we compared the SFCT measurements in the affected eyes with the data obtained in the contralateral unaffected eyes of the patients in the study group. As the third step, we performed a univariate analyses of associations between SFCT and other ocular and systemic parameters, such as refractive error, age and gender. Previous large-scale studies had revealed such associations. As the fourth step, we conducted multivariate analyses with choroidal thickness as a dependent variable, and those parameters that were significantly associated with choroidal thickness in univariate analysis were used as independent variables. As the fifth step of the analyses, we performed binary regression analyses, univariate and multivariate, with the diagnosis of nonarteritic AION as the dependent variable and the other parameters, including choroidal thickness measurements, as independent variables. Odds ratios (ORs) and 95% confidence intervals (95% CIs) were presented. All P values were based on 2-sided tests and were considered statistically significant when the values were less than 0.05.
Results
The study group included 20 patients (16 men) with unilateral acute nonarteritic AION. The mean age was 66.9 ± 9.8 years (range, 42–80 years), and the mean refractive error was + 1.18 ± 1.93 diopters (range, −1.25 to +5.25 diopters). The study group was differentiated into 11 patients with first manifestations of nonarteritic AION and 9 patients who had attended the hospital with acute nonarteritic AION in the second eye when the first eye had experienced nonarteritic AION several months earlier. The control group included 58 patients (58 eyes) with no abnormality of the fundus. The mean age in the control group was 71.9 ± 11.7 years, and the mean refractive error was −0.20 ± 2.27 diopters. The study group and the control group differed significantly in refractive error ( P = 0.008), whereas age differences were not significant ( P = 0.07).
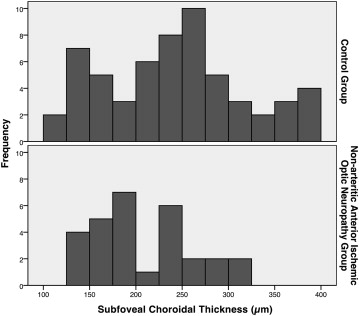
In the univariate analyses, the mean SFCT was marginally ( P = 0.05) thinner in the study group (207 ± 55 μm) than in the control group (248 ± 73 μm) ( Figure ).
In the first step of the statistical analyses, we compared choroidal thickness between the affected eyes and the contralateral unaffected eyes within the group of patients with unilateral nonarteritic AION and without histories of previous nonarteritic AION in the contralateral eye. The difference between the groups was not statistically significant (all P values >0.20) ( Table 1 ). A similar result was obtained for the subgroup of patients with acute unilateral nonarteritic AION and previous nonarteritic AION in the contralateral eyes (all P values >0.20).
| Parameter | Affected Eye | Contralateral Unaffected Eye | P Value a |
|---|---|---|---|
| Subfoveal | 205 ± 50 | 214 ± 48 | 0.70 |
| 1 mm to the fovea nasal | 183 ± 59 | 185 ± 63 | 0.91 |
| 2 mm to the fovea nasal | 147 ± 41 | 156 ± 46 | 0.64 |
| 2.5 mm to the fovea nasal | 127 ± 35 | 126 ± 36 | 0.94 |
| 1 mm to the fovea temporal | 190 ± 54 | 208 ± 55 | 0.34 |
| 2 mm to the fovea temporal | 172 ± 46 | 194 ± 60 | 0.66 |
| 2.5 mm to the fovea temporal | 165 ± 41 | 175 ± 55 | 0.88 |
a P value = statistical significance of the difference between the groups.
In the second step of the statistical analyses, we searched for associations between SFCT and other parameters in the control group. It was revealed that SFCT was significantly associated with younger age ( P = 0.001) and hyperopic refractive error ( P = 0.049), whereas gender ( P = 0.07), horizontal disc diameter ( P = 0.32) and vertical disc diameter ( P = 0.07) were not significantly associated with SFCT.
In the third step of the analyses, we performed a multivariate analysis with SFCT as a dependent variable and age, refractive error and diagnosis of nonarteritic AION as independent variables. It showed that thinner SFCT was significantly associated with the diagnosis of nonarteritic AION ( P = 0.001; standardized regression coefficient beta, −0.37; regression coefficient B, −55; 95% CI, −87, −23), after adjusting for age ( P < 0.001; beta, −0.43; regression coefficient B, −2.6; 95% CI, −3.9, −1.3); and refractive error ( P = 0.20; beta, 0.14; regression coefficient B, 4.4; 95% CI, −2.3, 11.2). If horizontal disc diameter or vertical disc diameter was added to the model as an independent variable, similar results were obtained, whereas horizontal disc diameter ( P = 0.56) or vertical disc diameter ( P = 0.72) was not significantly associated with SFCT. In addition, thinner choroidal thickness measurements obtained in the parafoveal region (1000 μm horizontal distance from the fovea) were associated with the diagnosis of nonarteritic AION in the same multivariate model ( Table 2 ).
| Parameter | P Value | Standardized Regression Coefficient Beta | Regression Coefficient B | 95% Confidence Interval |
|---|---|---|---|---|
| Subfoveal | 0.001 | −0.37 | −55.1 | −86.9, −23.3 |
| 1 mm to the fovea nasal | 0.002 | −0.35 | −49.0 | −79.1, −18.8 |
| 2 mm to the fovea nasal | 0.029 | −0.25 | −33.4 | −63.2, −3.6 |
| 2.5 mm to the fovea nasal | 0.055 | −0.22 | −28.2 | −57.0, −0.6 |
| 1 mm to the fovea temporal | 0.002 | −0.35 | −46.2 | −74.9, −17.6 |
| 2 mm to the fovea temporal | 0.000 | −0.43 | −49.7 | −73.8, −25.5 |
| 2.5 mm to the fovea temporal | 0.000 | −0.52 | −57.8 | −80.5, −35.0 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


