Purpose
To investigate long-term changes in subfoveal choroidal thickness (SCT) after photodynamic therapy (PDT) and their relationship with chronic central serous chorioretinopathy (CSC) recurrence.
Design
Retrospective, observational, comparative case series.
Methods
Fifty-seven eyes with chronic CSC (52 patients, ≥2 years follow-up) treated with half-fluence or half-dose PDT were divided into 2 groups: those with incomplete CSC resolution or subretinal fluid (SRF) recurrence (SRF+) and those with complete SRF absorption without disease recurrence (SRF−). The SCT was measured using spectral-domain optical coherence tomography and relative SCT ratios (follow-up SCT: baseline SCT ratio) were compared between the 2 groups.
Results
Mean follow-up period was 33.9 ± 9.9 months (range: 24–62 months). Four of 57 eyes (7%) had persistent SRF after PDT and 12 of 53 eyes (22.6%) had initial SRF resolution with SRF recurrence. The SRF+ group had a slower reduction in SCT during the first month ( P < .001) and a higher relative SCT ratio than the SRF− group throughout follow-up ( P < .001). The relative SCT ratio at 1 month was highly predictive of CSC recurrence (area under the curve = 0.902, 95% confidence interval: 0.823–0.982). Using a relative SCT ratio cutoff of 93.1%, sensitivity of this measure was 93.8% and specificity was 78.1%.
Conclusions
Those with incomplete SRF absorption or SRF recurrence had a slower SCT decline at 1 month and a higher SCT ratio throughout follow-up compared to those without CSC recurrence. The SCT changes may reflect PDT efficacy and help predict long-term recurrence and early treatment outcomes.
Central serous chorioretinopathy (CSC) is a relatively common disorder and is characterized by serous detachment of the neurosensory retina with diffuse retinal pigment epithelium decompensation. Although the exact pathophysiology of CSC remains unknown, indocyanine green angiography (ICGA) images have revealed hyperpermeable choroidal vessels and enhanced-depth imaging optical coherence tomography (OCT) images have revealed a thickened choroid. Both of these findings suggest that the disease originates in the choroid. Moreover, recent topographic studies have shown a high level of correspondence between angiographic (primarily choroidal hyperfluorescence) and OCT (primarily a thickened choroid) abnormalities.
Although there is no standard therapy for CSC, photodynamic therapy (PDT) is gaining popularity as an effective treatment. This therapy induces vascular endothelial damage and thrombus formation, causing short-term choriocapillary occlusion and long-term choroidal vascular remodeling. These changes result in caliber normalization of dilated, congested choroidal vessels and are thought to be the mechanism by which PDT treats CSC. Various modifications to standard PDT were recently shown to be successful. These changes aimed to reduce potentially harmful effects of PDT and included reducing laser fluence and photosensitizer dose.
It is well known that choroidal thickness decreases after PDT in eyes with CSC. Maruko and associates compared choroidal thickness changes in eyes with CSC treated with either laser photocoagulation or half-dose PDT. They found that although subretinal fluid (SRF) resolved in both groups, choroidal thickness decreased in only the PDT group. Several subsequent studies have also shown a decrease in choroidal thickness after half-fluence PDT in eyes with CSC. However, even after PDT, angiographically abnormal areas present before treatment showed considerable choroidal thickening compared to other macular areas. This finding suggests that choroidal structural abnormalities, represented as choroidal thickening, is a possible cause of CSC recurrence. Another study compared treatment efficacy of half-dose PDT and one-third-dose PDT for chronic CSC. In contrast to eyes treated with half-dose PDT, choroidal thickness did not change in 4 of 6 eyes receiving one-third-dose PDT that had residual SRF. However, these studies only measured choroidal thickness within 3 months of PDT. Therefore, the long-term effects of PDT on choroidal thickness remain unknown, along with the relationship between choroidal thickness changes and disease recurrence. In this study, we investigated the long-term effects of half-fluence and half-dose PDT on subfoveal choroidal thickness in chronic CSC patients. The relationship between subfoveal choroidal thickness changes and disease recurrence was also examined.
Methods
We retrospectively reviewed the medical records of patients diagnosed with chronic CSC who underwent PDT at Seoul National University Bundang Hospital between October 1, 2009 and July 30, 2012. This study was reviewed and approved by the institutional review board (IRB) of Seoul National University Bundang Hospital (IRB No. B-1410-271-114, Seongnam, South Korea). Informed consent was obtained from every patient before PDT was administered. All study conduct adhered to the tenets of the Declaration of Helsinki.
Subjects
The CSC diagnosis was based on funduscopy, fluorescein angiography (FA), ICGA (Heidelberg Retina Angiography; Heidelberg Engineering, Heidelberg, Germany), and OCT (Spectralis OCT; Heidelberg Engineering) findings. Chronic CSC was defined as presence of recurrent symptoms or symptoms that had persisted for more than 3 months. Patients were included in data analyses if all of the following were true: (1) diagnosis of chronic CSC, (2) presence of SRF involving the fovea on OCT, and (3) at least 24 months of follow-up after PDT. Patients were excluded from analyses if any of the following were true: (1) history of previous PDT, (2) presence of other chorioretinal disorders (eg, choroidal neovascularization) that might affect visual acuity and/or the foveal structure, or (3) history of intraocular surgery (except uncomplicated cataract surgery).
Photodynamic Therapy
The half-fluence PDT treatment, which used a reduced laser fluence (25 J/cm 2 , 689 nm laser, 83 seconds treatment time) with a full verteporfin dose (6 mg/m 2 , Visudyne; Novartis AG, Basel, Switzerland), was performed in most cases examined. However, half-dose PDT, which used full fluence (50 J/cm 2 ) with a reduced verteporfin dose (3 mg/m 2 ), was also performed by a single physician (W.S.J.) between January 1, 2011 and July 30, 2012. The PDT spot size was defined as the diameter of the smallest circle covering the main hyperpermeable choroidal lesion, as identified on mid-phase ICGA, which resulted in SRF accumulation. If there were 2 distinct choroidal hyperpermeable lesions, both were measured and treated separately during the same PDT session. In these cases, overall PDT spot size was defined as the sum of the individual PDT spot sizes.
Optical Coherence Tomography Measurements
Central macular thickness (CMT) was defined as mean retinal thickness within the central 1-mm zone of the Early Treatment of Diabetic Retinopathy Study (ETDRS) grid. This value was automatically calculated by the OCT software used for evaluation. The subfoveal choroidal thickness was defined as the distance between the outer portion of the retinal pigment epithelium and the inner surface of the sclera directly beneath the foveal center. This parameter was manually measured on foveal-centered horizontal and vertical enhanced-depth imaging OCT images using the built-in caliper tool. Each image used for measurement was the average of 50–100 line scans and subfoveal choroidal thickness was taken as the average of horizontal and vertical scan measurements. Two observers (Y.K.K., N.K.R.) independently measured subfoveal choroidal thickness and the average of these 2 measurements was the final value used in analyses. To evaluate the interobserver reproducibility of subfoveal choroidal thickness measurement, the intraclass correlation coefficients (ICC [2, 1]) were calculated for subfoveal choroidal thickness. The fovea-to-PDT spot distance, defined as the distance between the PDT spot center and the foveal center, was also manually measured using the built-in caliper tool. The PDT spot location was also categorized as foveal (completely involving central 1-mm ETDRS grid circle), juxtafoveal (partially involving central 1-mm ETDRS grid circle), and extrafoveal (entirely outside of central 1-mm ETDRS grid circle).
Ophthalmic Examinations and Study Group Characteristics
Patients were examined 1 month after PDT and every 3–4 months thereafter. Snellen best-corrected visual acuity (BCVA) measurements were converted to the logarithm of the minimal angle of resolution (logMAR) scale for all analyses. Patients were divided into 2 study groups based on the presence or absence of SRF following PDT. Patients with residual SRF after PDT or those that had recurrence of PDT-resolved SRF during follow-up were placed into the SRF+ group. Patients that had complete SRF resolution following PDT without SRF recurrence during follow-up were placed into the SRF− group.
Data Analyses
Data are presented as mean ± standard deviation, where applicable. Serial changes in BCVA, CMT, and subfoveal choroidal thickness were compared between the 2 study groups using linear mixed modeling. In these models, study group and time were fixed effects and patient identification number was the categorical random effect. The rate of SRF absorption was compared between the 2 groups using log-rank tests. A multiple logistic regression analysis was performed using factors that were significantly associated with incomplete absorption or recurrence of SRF after PDT. We also performed receiver operating characteristic curve analysis using 1 month subfoveal choroidal thickness ratio and previous CSC treatment history for predicting incomplete absorption or recurrence of SRF after PDT. Statistical analyses were performed using statistical software (Stata version 13.0; Stata Corp, College Station, Texas, USA) and statistical significance was defined as P < .05.
Results
During the study period, a total of 120 eyes of 112 patients underwent PDT (half-fluence PDT: 89 eyes; half-dose PDT: 31 eyes) to treat chronic CSC. After excluding cases with no follow-up OCT images (6 eyes), follow-up loss, and short follow-up periods (<2 years, 57 eyes), 57 eyes of 52 patients were ultimately included in study analyses (half-fluence PDT: 39 eyes; half-dose PDT: 18 eyes). The mean follow-up period of these 57 eyes was 33.9 ± 9.9 months (range: 24–62 months). Treatment with PDT resulted in a significant improvement in BCVA and a significant reduction in CMT and subfoveal choroidal thickness over the 2-year follow-up period (all P < .001, linear mixed modeling). Interobserver reproducibility of the subfoveal choroidal thickness measurements was excellent, with ICC [2, 1] values between 0.941 and 0.995 for each follow-up visit. Fifty-three of 57 eyes (93%) had complete SRF absorption after the initial PDT session, while the remaining 4 eyes had persistent SRF. Twelve of 53 eyes (22.6%) that had initial SRF resolution had SRF recurrence during the follow-up period. Therefore, 16 eyes were placed in the SRF+ group and 41 eyes were placed in the SRF− group.
Subject Characteristics
Demographic and clinical characteristics were compared between SRF+ and SRF- groups ( Table 1 ). The SRF+ group, which had incomplete SRF absorption or SRF recurrence, had a higher rate of previous focal laser therapy or intravitreal anti–vascular endothelial growth factor (VEGF) injections than the SRF− group (44% vs 10%, P = .011). Age, sex, refractive error, disease chronicity, and PDT parameters were not significantly different between the 2 groups. None of the CSC cases occurred secondary to corticosteroid use ( Table 1 ).
| SRF+ Group (N = 16) | SRF− Group (N = 41) | P Value a | |
|---|---|---|---|
| Age, y | 49.8 ± 10.7 | 48.0 ± 7.0 | .873 |
| Male, n (%) | 13 (81) | 33 (80) | >.999 |
| Diabetes mellitus, n (%) | 1 (6) | 2 (5) | >.999 |
| Hypertension, n (%) | 2 (13) | 7 (17) | >.999 |
| Refractive error (SE, diopters) | −1.0 ± 2.5 | −0.5 ± 1.1 | .993 |
| Follow up period (mo) | 39.8 ± 12.9 | 31.4 ± 7.6 | .062 |
| Time span since first episode (mo) | 11.9 ± 10.8 | 26.8 ± 41.2 | .310 |
| Previous or concurrent use of corticosteroid, n (%) | 0 | 0 | >.999 |
| Previous CSC treatment, n (%) | .011 | ||
| None or oral medication b only | 9 (56) | 37 (90) | |
| Focal laser | 2 (13) | 1 (2) | |
| Anti-VEGF treatment | 5 (31) | 3 (7) | |
| PDT parameters | |||
| Distance from fovea to PDT spot center (μm) | 951 ± 929 | 675 ± 630 | .220 |
| PDT spot size (μm) | 2869 ± 934 | 2949 ± 790 | .451 |
| PDT spot location, n (%) | .173 | ||
| Foveal | 9 (56) | 32 (78) | |
| Juxtafoveal | 4 (25) | 6 (15) | |
| Extrafoveal | 3 (19) | 3 (7) | |
| Half-fluence:half-dose, n (%) | 13:3 (81:19) | 26:15 (63:37) | .193 |
| Visual outcome | |||
| Baseline BCVA (logMAR) | 0.63 ± 0.56 | 0.36 ± 0.32 | .076 |
| 2-year BCVA (logMAR) | 0.33 ± 0.46 | 0.14 ± 0.19 | .255 |
| 2-year visual gain (logMAR) | 0.31 ± 0.43 | 0.22 ± 0.24 | .830 |
| 2-year BCVA improved, n (%) c | 7 (44) | 12 (29) | .297 |
| 2-year BCVA stable, n (%) d | 16 (100) | 40 (98) | >.999 |
| Baseline OCT | |||
| Central macular thickness (μm) | 349.6 ± 81.9 | 409.0 ± 125.8 | .124 |
| Subfoveal choroidal thickness (μm) | 405.8 ± 86.3 | 417.8 ± 133.8 | .979 |
| PED, n (%) | 5 (31) | 15 (37) | .767 |
| Post-PDT 1-month OCT | |||
| Central macular thickness (μm) | 245.9 ± 54.7 | 229.2 ± 34.7 | .472 |
| % Central macular thickness | 73.0 ± 19.0 | 60.4 ± 17.3 | .019 |
| Subfoveal choroidal thickness (μm) | 397.5 ± 83.0 | 357.8 ± 119.1 | .131 |
| % Subfoveal choroidal thickness | 98.1 ± 4.5 | 85.6 ± 10.1 | <.001 |
| Post-PDT 2-year OCT | |||
| Central macular thickness (μm) | 250.5 ± 80.7 | 238.9 ± 32.5 | .440 |
| % Central macular thickness | 73.1 ± 17.6 | 62.6 ± 16.6 | .039 |
| Subfoveal choroidal thickness (μm) | 374.0 ± 85.7 | 338.4 ± 107.9 | .214 |
| % Subfoveal choroidal thickness | 92.2 ± 7.7 | 81.5 ± 11.9 | .001 |
| PED, n (%) | 3 (19) | 1 (2) | .129 |
a Mann-Whitney test used for continuous variables, χ 2 or Fisher exact test used for categorical variables.
c Increase in visual acuity ≥3 lines.
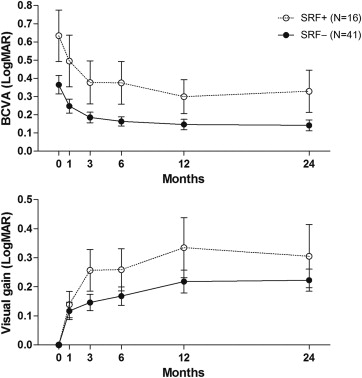
On average, the SRF+ group had a worse visual acuity during follow-up than the SRF− group (β-coefficient = 0.20, 95% confidence interval [CI]: 0.05–0.40, P = .012). However, there were no significant differences between groups in vision improvement (β-coefficient = 0.05, 95% CI: −0.057–0.004, P = .419, Figure 1 ).
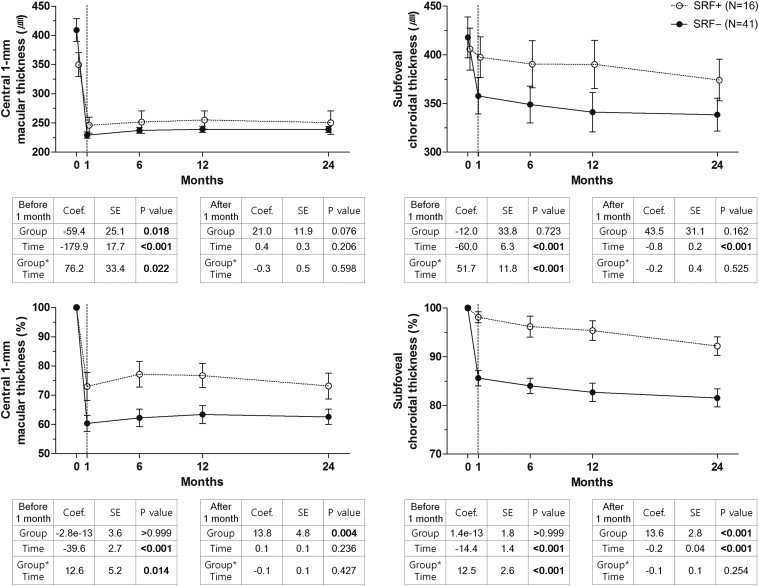
The CMT was significantly reduced 1 month after PDT ( P < .001), and this decrease persisted for at least 24 months ( P = .206, Figure 2 , Top left). There were differences between study groups in the rate of CMT reduction, as indicated by comparing CMT ratios (relative to baseline CMT) between groups at each follow-up visit. This revealed significant group and time interactions during the first month following treatment (β-coefficient = 12.6, 95% CI: 2.5–22.7, P = .014). After 1 month, the SRF+ group had a relatively higher CMT ratio than the SRF− group, which persisted throughout the follow-up period (β-coefficient = 13.8, 95% CI: 4.4–23.3, P = .004, Figure 2 , Bottom left). Similarly, significant differences between groups were observed in subfoveal choroidal thickness. There was a significant subfoveal choroidal thickness reduction in the first month following PDT ( P < .001) and, unlike CMT changes, a gradual subfoveal choroidal thickness reduction continued for the entire 2-year follow-up period (β-coefficient = −0.8, 95% CI: −1.1 to −0.4, P < .001, Figure 2 , Top right). The subfoveal choroidal thickness ratio (follow-up visit subfoveal choroidal thickness: baseline subfoveal choroidal thickness ratio) also showed a significant interaction in group and time during the first month (β-coefficient = 12.5, 95% CI: 7.4–17.6, P < .001), suggesting different subfoveal choroidal thickness reduction rates in the 2 study groups. Additionally, the SRF+ group maintained a higher subfoveal choroidal thickness ratio than the SRF− group throughout the follow-up period (β-coefficient = 13.6, 95% CI: 8.1–19.2, P < .001, Figure 2 , Bottom right). There were also significant differences between groups in the rate of SRF absorption. Interestingly, the SRF+ group had delayed SRF absorption compared with the SRF− group ( P = .012, log-rank test, Figure 3 ).
The clinical characteristics of patients with incomplete SRF absorption or SRF recurrence are summarized in Table 2 . Four patients had persistent SRF after initial PDT, with 2 of them having only mild SRF and photoreceptor ellipsoid zone disruption. Therefore, these patients chose not to undergo additional treatment. The other 2 patients underwent additional therapy (1 patient received intravitreal bevacizumab therapy, 1 patient underwent additional PDT), which resulted in SRF absorption in both patients. Twelve eyes had SRF recurrence during follow-up. Seven eyes had recurrence at the original leakage site, 4 eyes had recurrence at a new site, and 1 eye had recurrence at both the previous and a new site. Recurrence occurred an average of 21.4 ± 14.8 months (range: 2–58 months) after the initial PDT session. Three of 12 eyes (25%) had recurrence within 1 year and 9 of 12 eyes (75%) had recurrence within 2 years. Of the 12 patients that had SRF recurrence, 5 patients were not treated further, 5 patients underwent additional PDT, 1 patient underwent intravitreal bevacizumab injection, and 1 patient was lost to follow-up. The patient that was lost to follow-up had recurrence at 24 months and so was still included in analyses. The 11 patients followed after SRF recurrence all had a good clinical course, with a decrease in or a complete absorption of SRF after additional treatment ( Table 2 ).
| No. | Age | Sex | Symptom Duration (Months) | Previous Treatment | PDT Parameters | Early Outcomes | Recurrence or Persistent SRF | Visual Acuity | Follow-up Period Months) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Distance From Fovea (μm) | Spot Number | Spot Size (μm) | HF or HD | SRF Absorb | 1-Month CMT Ratio | 1-Month SCT Ratio | Time (Months) | Location | Treatment | Final Status | Initial | 2 Years | ||||||
| 1 | 54 | M | 26 | No | 270 | 1 | 2700 | HF | No | 65.2 | 89.5 | – | Same | Observation | Mild SRF | 20/125 | 20/100 | 34 |
| 2 | 49 | M | 3 | No | 250 | 1 | 2700 | HF | No | 77.6 | 98.8 | – | Same | IVB | SRF (−) | 20/200 | 20/200 | 50 |
| 3 | 47 | M | 40 | IVB | 2500 | 1 | 4000 | HD | No | 108.4 | 94.1 | – | Same | PDT | SRF (−) | 20/32 | 20/20 | 24 |
| 4 | 69 | M | 6 | IVB | 250 | 1 | 3000 | HF | No | 67.8 | 101.8 | – | Same | Observation | Mild SRF | CF at 1 m | 20/100 | 42 |
| 5 | 38 | M | 8 | No | 1300 | 1 | 2000 | HF | Yes | 90.0 | 93.1 | 34 | New | Observation | Mild SRF | 20/25 | 20/20 | 52 |
| 6 | 40 | M | 15 | No | 1070 | 1 | 2500 | HF | Yes | 73.0 | 93.1 | 58 | New | PDT | SRF (−) | 20/100 | 20/20 | 62 |
| 7 | 46 | M | 26 | No | 300 | 1 | 2400 | HD | Yes | 40.1 | 98.0 | 26 | Same | Observation | Mild SRF | 20/63 | 20/63 | 28 |
| 8 | 47 | M | 3 | No | 750 | 1 | 2000 | HD | Yes | 77.5 | 101.5 | 20 | Same & new | PDT | SRF (−) | 20/32 | 20/25 | 24 |
| 9 | 52 | M | 5 | No | 170 | 2 | 5000 | HF | Yes | 99.2 | 101.8 | 24 | New | Observation | SRF (−) | 20/32 | 20/25 | 34 |
| 10 | 51 | M | 4 | No | 3000 | 1 | 2800 | HF | Yes | 75.8 | 103.3 | 5 | Same | Observation | SRF (−) | 20/200 | 20/32 | 50 |
| 11 | 51 | M | 20 | No | 250 | 1 | 2800 | HF | Yes | 85.9 | 103.4 | 17 | Same | PDT | SRF (−) | 20/63 | 20/25 | 50 |
| 12 | 61 | F | 4 | Focal laser | 1800 | 1 | 2000 | HF | Yes | 46.3 | 93.5 | 7 | Same | PDT | SRF (−) | 20/50 | 20/25 | 31 |
| 13 | 74 | F | 4 | Focal laser | 1700 | 1 | 3500 | HF | Yes | 48.2 | 94.1 | 22 | Same | Observation | Mild PED | 20/63 | 20/32 | 50 |
| 14 | 39 | F | 5 | IVB | 150 | 1 | 2000 | HF | Yes | 63.5 | 100.4 | 24 | Same | Lost to FU | Lost to FU | 20/32 | 20/40 | 24 |
| 15 | 40 | M | 12 | IVB | 150 | 1 | 2000 | HF | Yes | 61.2 | 101.5 | 17 | Same | PDT | SRF (−) | 20/32 | 20/25 | 31 |
| 16 | 38 | M | 10 | IVB | 800 | 1 | 4500 | HF | Yes | 88.1 | 101.7 | 2 | New | IVB | SRF (−) | 20/100 | 20/50 | 54 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


