Purpose
To determine the frequency and clinical characteristics of chorioretinal folds emanating from the edge of a staphyloma in highly myopic patients.
Design
Observational case series.
Methods
Eight hundred and eighty-three eyes of 463 patients with an axial length ≥26.5 mm in at least 1 eye were studied. The fellow eyes of patients with unilateral high myopia were also included. Wide-field fundus images and fundus autofluorescence images were used to detect chorioretinal folds emanating from the staphyloma edge. In 100 patients, the eye shape was analyzed by 3-dimensional magnetic resonance imaging (3D MRI).
Results
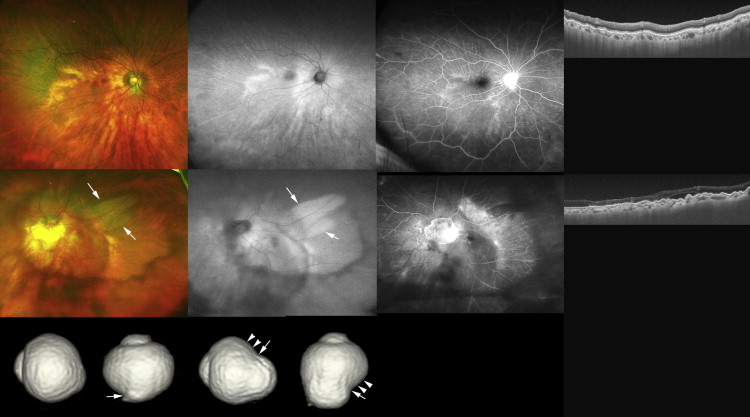
A posterior staphyloma was found in 459 of the 883 eyes (52.0%). Choroidal folds radiating from the staphyloma edge were found in 6 of the 459 eyes (1.3%) with a posterior staphyloma in wide-field autofluorescent images. The axial length varied greatly from 24.3 mm to 32.5 mm. Regardless of the axial length, all of the 6 eyes had a wide, macular type of staphyloma. Chorioretinal folds emanated from the upper or upper-temporal staphyloma edge. 3D MRI images showed the presence of a notch along the upper or temporal edge of the outpouching, and the eye curvature became flatter toward the steep edge of the outpouching.
Conclusions
Chorioretinal folds can emanate from the staphyloma edge in highly myopic patients even though the edge was away from the macula. Some directional force toward the steeper edge of the staphyloma might be related to the development of chorioretinal folds.
Chorioretinal folds have been reported to be present in various ocular and systemic conditions including hyperopia, choroidal neovascularization, and eyes with an orbital mass. Chorioretinal folds are also known to develop in eyes with tilted disc syndrome. In eyes with an inferior staphyloma due to the tilted disc syndrome, the upper edge of the staphyloma is located in the foveal region, and the chorioretinal folds run radially from the upper edge of the inferior staphylomas. However, it is not known whether chorioretinal folds are also observed in association with the different types of myopic staphylomas other than inferior staphylomas.
The High Myopia Clinic at Tokyo Medical and Dental University was established in 1974, and the number of registered patients exceeds 3600. Through our experience with these patients in the High Myopia Clinic, we have noted that some of the highly myopic eyes had chorioretinal folds emanating from the staphyloma edge even though the type of staphyloma was the wide, macular type and not the inferior type. In addition, the upper edge of the staphyloma was distant away from the fovea. These patients did not have any obvious lesions that could have caused the chorioretinal folds. A PubMed search on May 2015 with keywords “chorioretinal folds” extracted 58 publications of eyes with chorioretinal folds associated with various disorders. However, none of the publications included the eyes with pathologic myopia.
Chorioretinal lesions that develop within the staphyloma in highly myopic eyes are well known ; however, lesions developing away from the staphyloma have not been extensively investigated. Recently, wide-field fundus imaging has become available, and wide-field conventional fundus images and wide-field fundus autofluorescence (FAF) images can also be obtained. We recently reported the presence of radial tracts emanating from the upper edge of a staphyloma that ran upward against gravity in the wide-field FAF images.
The purpose of this study was to investigate the frequency and characteristics of these chorioretinal folds in patients with unilateral and bilateral high myopia with staphylomas. Eyes with the tilted disc syndrome were excluded. The pathogenesis of the chorioretinal folds was also investigated by analyzing the relationship between the patterns of chorioretinal folds and the eye shape obtained by 3-dimensional magnetic resonance imaging (3D MRI).
Methods
This was a retrospective, observational case series study. The procedures used conformed to the tenets of the Declaration of Helsinki, and the review of the medical records was approved by the Ethics Committee of Tokyo Medical and Dental University. The medical records of 463 consecutive patients who had been diagnosed with pathologic myopia, defined as an axial length ≥26.5 mm in at least 1 eye, and who had undergone fundus examination by the Optos Optomap Panoramic 200A system (Optos PLC, Dunfermline, United Kingdom) at the High Myopia Clinic of Tokyo Medical and Dental University between March 2, 2012 and July 12, 2013 were analyzed. Thus, the fellow eyes of patients with unilateral high myopia were also included. Patients with tilted disc syndrome and eyes whose staphyloma edge crossed the central fovea were excluded. Patients with other diseases that have been shown to be associated with chorioretinal folds (eg, thyroid eye disease, posterior scleritis, orbital tumors, hypotony, uveal effusion syndrome, age-related macular degeneration, and prior vitreoretinal surgery) were excluded. Patients with a history of autoimmune diseases or systemic malignancy were also excluded. A history of hypertension was not precisely documented for each patient.
Pseudo-color fundus images and FAF images were obtained by Optos for all of the patients. Choroidal folds had characteristic linear patterns in the FAF images, and the presence of choriodal folds was based on FAF images as determined by 2 of the authors independently (T.I. and K.S.). In all eyes with FAF findings suggestive of chorioretinal folds, their presence was confirmed by swept source optical coherence tomography (DRI-OCT-1; Topcon, Tokyo, Japan). One hundred and ten eyes also had fluorescein angiography (FA) with the Optos SLO instrument, and all patients had an axial length measurement with the IOL Master (Carl-Zeiss Meditec, Tubingen, Germany). One hundred eyes also had 3D MRI analyses of the shape of the eye including the type of staphylomas. The methods used to analyze the 3D MRI images have been presented in detail.
The presence of a posterior staphyloma was based on the presence of pigmentary abnormalities along the presumed staphyloma edge in the pseudo-color images as well as the FAF images obtained by the Optos system. We recently reported our findings on the comparisons of the Optos images and 3D MRI images of eyes with a staphyloma. This is relevant to this study because we found that the pigmentary abnormalities along the presumed edge of the staphyloma in the Optos images correlated very well with the presence and types of staphyloma detected by 3D MRI images.
Results
Nine hundred and twenty-six eyes of 463 patients were examined with wide-field fundus imaging. From the 926 eyes, 43 eyes of 43 patients were excluded: 4 eyes of 4 patients because the axial length data were unreliable because of bad fixation, 4 eyes of 4 patients because of phthisis bulbi, 29 eyes of 29 patients because their fundus images were not clear enough owing to dense cataracts, and 6 eyes of 6 patients because the eyes had tilted disc syndrome and the edge of inferior staphyloma crossed the fovea.
In the end, 883 eyes of 463 patients were studied. A posterior staphyloma was present in 459 of the 883 eyes (52.0%, 286 patients). The mean age of the 286 patients was 67.9 ± 9.8 years with a range of 27–89 years. The mean axial length of the 459 eyes was 30.2 ± 2.4 mm with a range of 23.5–40.0 mm. Interestingly, a staphyloma was found in 21 of the 54 non–highly myopic eyes (38.9%) of unilaterally highly myopic patients.
Choroidal folds radiating from the staphyloma edge were found in 6 of 459 eyes (1.3%) with a posterior staphyloma in wide-field FAF images, whereas they were not found in any of the eyes without a staphyloma. The characteristics of these 6 eyes are shown in the Table 1 . The axial length varied greatly from 24.3 mm to 32.5 mm. Regardless of the axial length, all 6 eyes had the wide, macular type of staphyloma according to the classification by Ohno-Matsui. The choroidal folds emanated from the temporal edge of the staphyloma in 2 eyes and from the upper to temporal edge in the other 4 eyes. In the 3D MRI images of the patients with unilateral high myopia, deformities of the globe were observed in both eyes ( Figures 1 and 2 ). The ocular wall peripheral to the superior or temporal edge of the outpouching was somewhat flatter than the lower wall of the globe in the image viewed nasally.
| Case | Age (y) | Sex | Side | Axial Length (mm) | Staphyloma | Type of Staphyloma a | Edge of Staphyloma From Which Choroidal Folds Emanate |
|---|---|---|---|---|---|---|---|
| 1 | 80 | F | R | 25.9 | + | Wide, macular | Upper to temporal |
| L | 29.3 | + | Wide, macular | Upper to temporal | |||
| 2 | 84 | F | R | 24.3 | + | Wide, macular | Temporal |
| 3 | 49 | F | R | 32.0 | + | Wide, macular | Upper to temporal |
| L | 32.5 | + | Wide, macular | Upper to temporal | |||
| 4 | 80 | F | R | 27.4 | + | Wide, macular | Temporal |
a Classification is based on pigmentary abnormalities along the presumed edge of the staphyloma (reference ).