Purpose
To describe the demographic features, clinical characteristics, and management in cases of childhood pterygium.
Design
Observational case series.
Methods
A retrospective review was done of 19 children (total 26 eyes) under the age of 16 years, consecutively presenting with pterygium and evaluated at a single tertiary care center between January 2000 and August 2011. The main outcome measures were clinical features, associated ocular or systemic diseases, approach towards its management, and histopathology of operated cases.
Results
Of the 19 patients, 10 were girls and 9 were boys. The mean age at presentation was 10.63 ± 3.48 years (range 2–15 years). Seven patients (37%) had bilateral involvement. None of the cases had familial history. The median refractive astigmatism was found to be −0.5 diopter cylinder. All the eyes had primary pterygium, except 1, which was recurrent. The majority of the eyes (85%) were managed conservatively. Four eyes (15%) required surgery, where pterygium excision with conjunctival-limbal autograft with fibrin glue application was done. The follow-up of surgical cases ranged from 5 to 38 months (median 6 months). One operated case recurred 1 year after surgery.
Conclusion
Development of pterygium is a possibility in younger age groups. No specific predisposing factors, either environmental or familial, were identified as contributing to childhood pterygium. The majority of the cases required conservative management.
We have known about pterygia, the wing-shaped fibrovascular growths on the corneal limbus, for thousands of years. While prevalence of pterygia is reported to be the highest among the elderly, development of new cases is greatest between the ages of 20 and 40. Although previous studies have indicated that genetic factors may contribute to the development of primary pterygium, scant literature is available describing its occurrence in the pediatric population. The existing literature on the latter topic is confined to a few isolated case reports and series that highlight the tendency of pterygium to occur in families. Specific data regarding the characteristics of pterygium in children and its management approach are lacking in literature. Herein, we report the information compiled from cases of pterygium in the age group below 16 years, presented at our tertiary care center over the last decade.
Methods
In this retrospective study, the medical records of 19 consecutive patients with pterygium, in the age group of below 16 years, were analyzed. All the patients were seen at L.V. Prasad Eye Institute, Hyderabad, India, between January 1, 2000 and August 31, 2011. This was out of a total figure of 329 049 children seen during the same period. This is equivalent to a hospital incidence of approximately 0.006% during the above-mentioned study period. The clinical diagnosis of pterygium was made when a radially oriented fibrovascular lesion growing over the limbus into the cornea was observed upon slit-lamp examination. Eyes that had a previous history of pterygium excision were also included in the study. Eyes with an atypical shape and invading tissue, symblepharon, and conjunctival scar tissue, such as seen in cases of xeroderma pigmentosum, and those with a history of ocular injuries were diagnosed as pseudopterygium and were not included in the study.
At presentation, a detailed history was obtained, including the patient’s demographic data, area (district) of residence, and medical and family history. For the purpose of evaluation, the residential area of the patients was categorized as either coastal or noncoastal. Referral reports from ophthalmologists and pediatricians were also evaluated. A comprehensive ocular examination was performed in all cases. All the children in the series were reasonably cooperative for examination in the clinic, and no case required examination under anesthesia. Particular care was taken to note any associated ocular or systemic pathology in all cases.
The possible indications for surgical management of pterygium were the presence of 1 or more factors, namely, proximity of pterygium to the visual axis, significant astigmatism, progression as documented by an ophthalmologist or reported by the parents, recurrence of pterygium, and surgery for cosmetic reasons. The technique of pterygium excision with conjunctival-limbal autograft with fibrin glue application (PTG Exc CLAG FG), which has been detailed elsewhere, was practiced in our series. All surgeries were performed under general anesthesia. The excised tissue was sent for histopathologic examination. The operated cases were managed with a tapering dose of prednisolone actetate 1% eye drops for 4 weeks and tobramycin sulfate 0.3% eye drops 4 times a day for 1 week. All surgical cases were followed up meticulously and all the conservatively managed cases were advised regarding appropriate regular follow-up.
Results
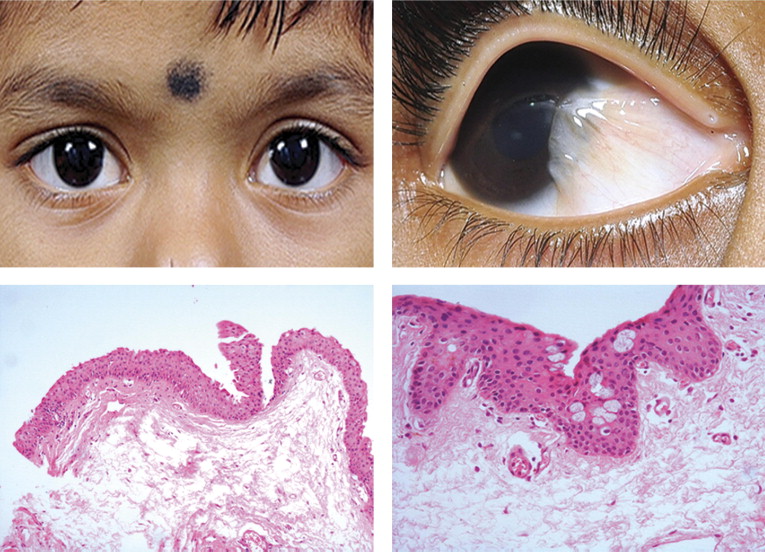
The demographic and clinical characteristics of our patients are depicted in Table 1 . The mean age at presentation was 10.63 ± 3.48 years (range 2–15 years). At presentation, 7 of 19 patients (37%) had bilateral involvement ( Figure , Top left). None of the cases in the series had a family history suggestive of pterygium or any systemic association. Two cases each were diagnosed with keratoconus and vernal keratoconjunctivitis, while 1 case each had posterior polar cataract and intermittent exotropia ( Table 1 ).
| Case No. | Age/Sex | Residential District (C/NC) | Presenting Complaint | Duration of Pterygium (mo) | BCVA (logMAR) | Spherical Equivalent | Refractive Astigmatism (D Cyl) | Pterygium Feature | Associated Ocular Disease | Pterygium Management | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OD | OS | OD | OS | OD | OS | ||||||||
| 1 | 15/F | Rangareddy (NC) | Fleshy growth | 12 | 0.1 | 0.1 | 1 | 0.5 | 0 | −1/120 | OU nasal pterygium | — | Obs |
| 2 | 15/F | Medak (NC) | OS UL swelling; DOV | 6 | 0 | 0.1 | 0.5 | 1.0 | 0 | −1/180 | OS inflammatory PTG | — | Topical steroids |
| 3 | 12/M | Rangareddy (NC) | DOV OU; fleshy growth | 4 | 0.4 | 0.3 | 0 | −2.25 | −8/180 | −1.5/175 | OU nasal PTG (OD>OS) | OU keratoconus, OU thin cornea | Optical correction; planned for pterygium surgery later |
| 4 | 10/M | Rangareddy (NC) | OU Itching, redness | 12 | 0.1 | 0.1 | 0.75 | 0.5 | −2/180 | 0 | OU nasal PTG | OU VKC, OD keratoconus | Obs; medical mgt |
| 5 | 12/M | Guntur (C) | DOV OU; fleshy growth | 6 | 0 | 0 | 1 | 0.75 | −1.0/180 | 0 | OD nasal PTG | — | Not willing for surgery; Obs |
| 6 | 10/M | Rangareddy (NC) | DOV OU | 12 | 0 | 0 | −1.25 | 1.75 | 0 | 0 | Early nasal PTG | — | Obs |
| 7 | 13/F | Guntur (C) | H/O OD PTG Exc in 2002; recurrence | 2 | 0 | 0 | 0.63 | −0.12 | −0.25/180 | −0.25/170 | OD nasal PTG | — | PTG Exc CLAG FG |
| 8 | 10/F | Rangareddy (NC) | Fleshy growth OS | 3 | 0 | 0 | 0 | 0 | 0 | 0 | OS nasal PTG | — | Obs |
| 9 | 4/M | Rangareddy (NC) | Fleshy growth OD | 24 | 0.1 | 0.1 | 0 | 0 | 0 | 0 | OD nasal PTG | — |
|
| 10 | 11/F | Nizamabad (NC) | H/O itching | 6 | 0 | 0 | 0 | −0.25 | 0 | −2.5/180 | OS nasal PTG | — | Obs |
| 11 | 11/F | Rangareddy (NC) | Fleshy growth, photophobia | 4 | 0.1 | 0 | −0.37 | 0 | −0.75/180 | 0 | OD temporal PTG | — | PTG Exc CLAG FG |
| 12 | 8/F | Nizamabad (NC) | Itching, redness | 1 | 0 | 0 | 0 | 0.37 | −0.75/180 | 0 | OD nasal PTG | VKC | Obs |
| 13 | 11/F | Rangareddy (NC) | Fleshy growth | 24 | 0.7 | 0.8 | +7.5 | +7.5 | −1/180 | −1/180 | OD nasal PTG | OU PPC; OU high hyperopia | Obs |
| 14 | 13/F | Guntur (C) | Fleshy growth | 4 | 0 | 0 | −0.75 | −0.75 | 0 | 0 | OU nasal PTG | — | Obs |
| 15 | 2/F | Prakasam (C) | White spot OU | 18 | 0.1 | 0.1 | 0.25 | 0.25 | 0 | 0 | OU nasal PTG | — | Obs |
| 16 | 15/M | Rangareddy (NC) | Fleshy growth | 2 | 0 | 0 | −0.75 | −0.75 | 0 | −0.5/70 | OU PTG | — | Obs |
| 17 | 10/M | Cuddapah (NC) | Fleshy growth | 4 | 0 | 0 | 0.25 | 0.5 | −0.5/90 | 0 | OD nasal PTG | — | Obs |
| 18 | 13/M | Rangareddy (NC) | Eye deviation, fleshy growth | 3 | 0 | 0 | 0 | 0 | 0 | 0 | OD nasal PTG | Exotropia | EOMS, PTG Exc CLAG FG |
| 19 | 7/M | Rangareddy (NC) | Fleshy growth | 3 | 0 | 0.1 | 0.25 | −0.25 | −0.5/20 | −0.5/20 | OS temp PTG | Obs | |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


