Chronic sinusitis affects millions of patients. Balloon technology is a tool that has enhanced the surgeon’s ability to treat patients suffering from chronic sinusitis. Three companies have developed products to dilate sinus ostia. An extensive literature review reveals that balloon catheters have an impressive safety profile and seem to be an effective tool for ostial dilatation. These tools are particularly effective in frontal recess dilatation and have great potential for office use under local anesthesia.
Close to 31 million Americans suffer from chronic rhinosinusitis. Endoscopic sinus surgery is currently the mainstay of treatment of patients who have failed medical management. The goals of surgery, traditionally, have been to remove inflamed tissue and bone to improve ventilation and drainage of the affected sinuses. Like all aspects of surgery, sinus surgery has evolved greatly since its inception.
Over the years, several notable pioneers have changed the way in which sinonasal disorders are treated. Near the turn of the nineteenth century, George Caldwell and Henri Luc individually described the canine fossa approach to the maxillary sinus. Nasal endoscopy was first used in 1901 by Hirshman, using a modified cystoscope. The development of the Hopkins rod telescope, patented in 1960, further revolutionized sinus surgery and enabled the otolaryngologist to navigate through the nasal cavity with unparalleled visualization. In 1978, Messerklinger published a collection of images detailing his surgical experience, which is considered a landmark in endoscopic sinus surgery. In the mid-1980s, Stammberger published a series of papers describing endoscopic sinus surgery techniques. Kennedy and colleagues brought these innovative techniques to the United States and coined the term “functional endoscopic sinus surgery.”
Image guidance systems, which were originally developed for neurosurgeons, have transitioned well into the operating room for sinus surgeons. The utility of this technology has allowed sinus surgeons to stretch the boundaries of endonasal procedures to include treatment of anterior skull base lesions. Although the use of image guidance originally met with some skepticism, many otolaryngologists have adopted this technology into their sinus surgery practice.
Balloon catheters have become available in endoscopic sinus surgery and are now a new tool to achieve the goals of sinus ostial dilatation. Balloon technology has been available for some time in other specialties, such as interventional cardiology, gastroenterology, endovascular surgery, and urology. In many instances, balloon technology has drastically changed treatment algorithms. An example of this paradigm shift is how angioplasty has now become an effective alternative to open cardiac surgery for selected patients with coronary artery disease.
Balloon catheter–based technology is a novel tool to access and dilate selected sinus ostia in patients with chronic rhinosinusitis, with the goal of preserving the mucosa and the surrounding structures. As with any new technology, there is always some degree of skepticism and doubt. In this article, the authors report on the available technology and discuss how these tools may be applied in sinus surgery. Safety and efficacy is analyzed through a review of published data.
Discussion
Three companies that manufacture balloon catheters have reported their use in endoscopic sinus surgery: Acclarent, Inc (Menlo Park, CA, USA), Quest Medical, Inc (Allen, TX, USA), and Entellus Medical, Inc (Maple Grove, MN, USA). Each company is described in the following sections, including relevant published literature. Some special considerations and potential points of controversy expand the descriptions.
Acclarent, Inc
Acclarent started their first investigation of balloon catheters in 2002. Since gaining approval to use these medical devices, approximately 3000 physicians have undergone training at various training facilities. More than 20,000 patients have been treated worldwide with balloon sinuplasty.
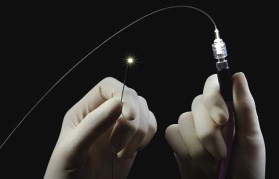
The technique involves a typical setup for endoscopic sinus surgery using a video tower and endoscopes. A guide catheter is positioned near the natural ostia of the sinus being treated. A wire is then passed through the guide catheter and is manipulated until it is confirmed to be located in the sinus cavity. The balloon catheter ( Fig. 1 ) is then passed over the guide wire through the guide sheath. Fig. 2 depicts the Acclarent Relieva system, with an endoscope and camera in a ghosted background. After conformation of the appropriate location, the balloon is then inflated and released. The balloon catheters are designed for multiple sinus use in a single patient. The surgery is often performed using fluoroscopic confirmation for wire and balloon placement, but recently a lighted guide wire called Luma ( Fig. 3 ) has been released. This lighted guide wire can provide a nonfluoroscopic option because direct sinus illumination can confirm location. The balloon catheter dilatation can be performed on the frontal, sphenoid, and maxillary sinus outflow tracts. If needed, a traditional endoscopic ethmoidectomy can be performed in addition to balloon ostial dilatation.


An initial feasibility study was performed by Bolger and Vaughan on human cadavers, with 100% success in dilating all of the 12 sinus ostia. Computed tomography (CT) scans were performed after the procedures, revealing microfractures of the sinus ostial regions without evidence of damage to the surrounding structure, such as the orbit or anterior skull base. This study was then followed by a pilot human study in 10 patients. Brown and Bolger dilated all planned ostia and observed ease with the frontal and sphenoid sinuses; the anesthesia time was also reduced. Some difficulty was reported while dilating the maxillary sinus and removing the lower portion of the uncinate in 5 of the 10 patients. The investigators did not report any adverse events or episodes of mucosal stripping.
The publication of the results of the CLEAR study (CLinical Evaluation to confirm sAfety and efficacy of sinuplasty in the paRanasal sinuses) has been instrumental in demonstrating clinical results of balloon sinuplasty. The study was published in 3 parts, starting with 24-week data, followed by 1-year data and then by 2-year data. The study, conducted at several institutions, comprised 115 patients. The study did not compare traditional sinus surgery with balloon sinuplasty, but evaluated hybrid procedures (balloon sinuplasty with traditional endoscopic sinus surgery, ie, ethmoidectomy) and balloon sinuplasty alone. No adverse events, including cerebral spinal fluid (CSF) leak, orbital injury, or nasal bleeding requiring nasal packing, were reported.
The CLEAR study measured sinus symptoms using Piccirillo’s validated SNOT-20 (Sino-Nasal Outcome Test) survey, which was given to the patients preoperatively and then postoperatively at 24 weeks, 1 year, and 2 years. All reports revealed a statistically significant improvement in the SNOT-20 scores. In the 2-year study, matched-pairs differences of the SNOT-20 scores were performed, and the investigators did not find any statistical difference between the scores at 24 weeks and 2 years. Similarly, there was no difference at 1 year compared with 2 years. This trend demonstrated that the patient’s symptoms did not worsen or improve further with time after 24 weeks. The greatest improvement in the SNOT-20 survey was a reduction in facial pain and pressure.
Another endpoint of the study was to compare preoperative and postoperative CT scans of the sinuses. The CT scans were scored using the Lund-Mackay scoring system. Patients undergoing the hybrid procedure had worse disease, and the Lund-Mackay scores were higher. When evaluating the mean for all patients in the study, the 1- and 2-year studies demonstrated improvement in Lund-Mackay scores. The difference between the scores at 1 and 2 years was not significant, indicating that there was neither further improvement nor worsening of the sinus disease as seen on CT scans. Regarding the subsets, patients who underwent the hybrid procedure had the most improvement in Lund-Mackay scores.
A clinical outcome of the study evaluated the ostial patency during postoperative nasal endoscopy. The overall observable patency rate was 80.5% and 85% at 24 weeks and 1 year, respectively. Patency was indeterminate in 17.9% (24 weeks) and 14% (1 year) of the patients. The overall nonpatency rate was low at 1.6% at 24 weeks and 1% at 1 year. The revision rate per sinus was 0.98%, 2%, and 3.6% at 24 weeks, 1 year, and 2 years, respectively. The revision rate per patient was 2.75% and 9.2% at 24 weeks and 2 years, respectively. A functional patency rate of 91.6% was reported when a clear sinus CT scan was observed, demonstrating a functionally patent sinus ostium.
The main criticism for the CLEAR study is the lack of randomization and the lack of a control arm. The best level of evidence as defined by the Oxford Centre for Evidence-Based Medicine is a randomized controlled clinical trial. This is not always possible, and much research in sinus surgery is level IV evidence (a case series without an internal control group). In addition, the investigators recognized that the improved outcomes may be influenced by a placebo effect and the natural history of the disease.
The PatiENT Registry provided results of a database of a retrospective review of 1036 patients who had 3276 sinuses treated. Although the study provides level IV evidence, it does reinforce a favorable device-safety profile. The database documented only 2 CSF leaks and 6 cases of minor bleeding that required cautery or packing. These 8 cases were performed in conjunction with standard functional endoscopic sinus surgery . The study did illustrate a practice trend of less debridements postoperatively in sinuplasty cases. A similar revision rate to the CLEAR study was reported in that 2.4% patients underwent revision surgery.
Although the CLEAR study did not report injuries to the skull base or the orbit, the MAUDE (Manufacturer and User Facility Device Experience) database reveals 5 incidents. Two reports involved penetration of the lamina papyracea, and one involved a skull base defect in a hybrid case resulting in a CSF leak. The remaining 2 cases reported balloon failure, in that the balloon broke away from the catheter.
Radiation exposure
Radiation exposure with the use of fluoroscopy can be a concern to the patient and the surgeon. Radiation to the eyes can cause damage to the proliferating cells in the epithelium, and the ultimate damage is cataract formation. The International Commission on Radiological Protection has stated that acute doses of 2 Gy, protracted occupational exposure of 4 Gy over less than 3 months, or 5.5 Gy over more than 3 months may cause cataract formation. It has also been reported that an average of 4.2 mGy per eye in balloon sinuplasty, which is much less than the cataract threshold. A CT scan of the sinuses in the axial plane has an average of 24.5 mGy to the lens, and in the coronal plane it is 35.2 mGy.
The surgeon is also exposed to radiation during balloon dilatation of the sinus ostia using Acclarent’s system. The fluoroscope used by a surgeon for balloon sinuplasty is in direct line of the fluoroscopy tube. In comparison, the hands of the interventional cardiologist is away from the actual field of the direct “beam” while working lower near the area of the femoral vein. Church studied the radiation exposure to a surgeon’s hands, neck, and eyes. Using the guidelines set by the US Code of Federal Regulations, he reported that a surgeon could perform more than 57,000 dilations per year before reaching an occupational limit for the hands, 20,000 dilations per year for the neck (thyroid), and 6000 dilations per year for the eyes. The direction of the fluoroscopic projection is an important factor. In the anteroposterior projection, the surgeon could perform 141 cases in a year before meeting the occupational limit for the hands.
Radiation exposure is an added risk to the patient and the surgeon. Ways to improve exposure include limiting the time of exposure by placing the fluoroscope on pulse as opposed to a continuous setting, projecting in a posteroanterior direction, shielding the patient’s eyes, and protecting the operating room staff with lead aprons and thyroid shields. The use of a thyroid shield would reduce the radiation dose by up to 95%. To address the radiation concern, a lighted guide wire (Luma) that can replace the need for fluoroscopy has been introduced. Direct sinus illumination by the guide wire can confirm proper location before balloon inflation.
Quest Medical, Inc
Quest Medical, Inc manufactures LacriCATH. Ophthalmologists have been using this technology to treat nasolacrimal duct obstruction since 1989. It was developed as an alternative to the open approach in treating nasolacrimal duct obstruction. The catheters have been described in an offlabel use for the treatment of sinus ostial obstruction. The catheters are unique in that they are balloons at the end of a malleable wire. This system does not require a guide wire and is available in a variety of diameters and lengths.
Citardi and Kanowitz first described the use of LacriCATH in the paranasal sinuses. A cadaveric study was performed without the use of fluoroscopy. It was reported that the catheter would fracture the free wall of the frontal recess, depending on the position of the agger nasi, and the fractured bone pieces could be retrieved. In the maxillary sinus, dilatation was successfully achieved in 3 of 6 maxillaries using a prebent 9-mm balloon designed for transnasal dacryocystorhinostomy. This study demonstrated the use of existing technology to perform the task of dilating sinus ostia without the use of fluoroscopy.
A second study was performed describing the use of the LacriCATH in the office setting for revision frontal sinus stenosis. Successful dilatation of 6 frontal sinus ostia was reported in the office setting without the use of fluoroscopy. This study reviewed 6 patients only but concluded that the technique was a feasible option for the office treatment of frontal sinus stenosis.
Entellus Medical, Inc
Some studies using balloon technology reported variable success in treating the maxillary sinus. Reports of trauma to adjacent structures and difficulty in identifying the natural ostium of the maxillary sinus were noted. Dilatation of the accessory ostium has also been reported. Citardi and Kanowitz reported successful dilatation of the maxillary ostium using LacriCATH in only 3 of 6 sinuses. Part of this challenge is because of the difficulty in identifying the natural ostium and the tendency of the balloon to drift posteriorly through either an accessory ostium or through a posterior fontanelle.
The Entellus Medical, Inc FinESS (Functional Infundibular Endoscopic Sinus surgery) system attempts to solve this problem by direct access into the maxillary sinus through a controlled canine fossa puncture with a small trocar. An access sheath is left in place after the trocar is removed. A canula is inserted through the access sheath, through which a small endoscope and a balloon catheter can be simultaneously placed. Direct visualization with a 0.5-mm flexible endoscope (Karl Storz, El Segundo, CA, USA) ( Fig. 4 ) into the maxillary sinus is performed for the identification of the natural maxillary ostium. A balloon catheter is then introduced under direct visualization through the natural ostium of the maxillary sinus and traversing the ethmoid infundibular space. The balloon is then inflated, widening the natural ostium and infundibulum and also deflecting the uncinate process medially. The maxillary sinus can then be irrigated as needed, through the canine fossa introducer. Fig. 5 depicts the basic setup for the Entellus FinESS system.




