Purpose
To determine the effectiveness of autologous transplantation of the internal limiting membrane (ILM) for refractory macular holes.
Design
Prospective, interventional case series.
Patient and Methods
Ten eyes of 10 consecutive patients who underwent autologous transplantation of the ILM for the treatment of refractory macular holes were studied. The primary diseases in these patients were large idiopathic macular holes that had existed for more than 1 year (4 eyes), a traumatic macular hole (1 eye), myopic foveoschisis (2 eyes), foveoschisis resulting from pit-macular syndrome (2 eyes), and proliferative diabetic retinopathy (1 eye). Apart from the 5 eyes with idiopathic or traumatic macular holes, macular holes developed in the other 5 eyes after initial vitrectomies with ILM removal. In all eyes, regular macular hole surgery failed to achieve closure. The main outcome measures used in this study were macular hole closure and best-corrected visual acuity (BCVA).
Results
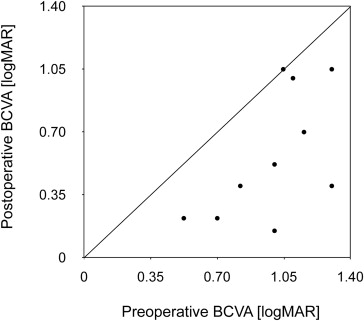
Macular holes were closed successfully in 9 eyes (90%) after autologous transplantation of the ILM. The postoperative BCVAs were significantly better than the preoperative BCVAs ( P = .007, paired t test). Postoperative BCVAs improved by more than 0.2 logarithm of the minimal angle of resolution units in 8 eyes (80%) and were unchanged in 2 eyes (20%).
Conclusions
Although this is a pilot study, the results suggest that autologous transplantation of the ILM may contribute to improved anatomic and visual outcomes in the treatment of refractory macular holes and may warrant further investigation.
Internal limiting membrane (ILM) peeling has become an important element in the surgical treatment of a variety of retinal disorders, including macular holes, epiretinal membranes, vitreomacular traction, retinoschisis, and macular edema. ILM peeling is thought to provide good anatomic and functional results in these diseases by releasing the tractional forces on the macula completely and reducing the risk of postoperative epiretinal membrane formation. However, removal of the ILM recently was suggested to be ineffective for refractory macular holes and to be detrimental in macular diseases such as foveoschisis by causing the development of secondary macular holes.
To address this problem, Michalewska and associates reported the efficacy of a modified surgical procedure, called the inverted ILM flap technique , for large macular holes. Kuriyama and associates also reported the efficacy of this procedure for myopic macular holes. To avoid the postoperative development of macular holes in myopic foveoschisis, Ho and associates and Shimada and associates reported an ILM peeling technique that left the epifoveal ILM in situ. Although these procedures can be an option for an initial vitrectomy, to avoid the failure of macular hole closure or the development of secondary macular holes, they cannot be applied to eyes with idiopathic macular holes, in which the initial vitrectomies with ILM peeling fail to achieve closure, or to eyes with secondary macular holes, in which the ILM already has been removed in previous vitrectomies.
To try to solve this problem, we developed a new surgical technique, called autologous transplantation of the ILM , that transplants a flap of the ILM to the inside of the macular hole. This study was carried out to evaluate the functional and anatomic efficacy of autologous transplantation of the ILM for the treatment of refractory macular holes.
Methods
Patients and Study Design
This study was a prospective, interventional case series. All investigations adhered to the tenets of the Declaration of Helsinki. Each patient was informed about the risks and benefits of the surgery and their written, informed consent was obtained. The study was approved by the Institutional Review Boards of Okayama University Graduate School of Medicine, Dentistry and Pharmaceutical Sciences and Kagawa University Faculty of Medicine.
Ten eyes of 10 consecutive patients who had refractory macular holes and who underwent pars plana vitrectomy with autologous transplantation of the ILM between May 1, 2012, and June 30, 2013, were enrolled in the study. The inclusion criteria were as follows: (1) clinical presentation with macular hole after the initial vitrectomy with ILM removal; (2) treatment with 25-gauge, 3-port pars plana vitrectomy with autologous transplantation of the ILM and 10% sulfur hexafluoride gas tamponade; and (3) a follow-up period of more than 3 months since the last vitrectomy. The primary diseases in these patients were large idiopathic macular holes with diameters of more than 400 μm that had existed for more than 1 year (4 eyes), a traumatic macular hole (1 eye), myopic foveoschisis (2 eyes), foveoschisis resulting from pit-macular syndrome (2 eyes), and proliferative diabetic retinopathy (1 eye). Apart from the 5 eyes with idiopathic or traumatic macular holes, macular holes developed in the remaining 5 eyes after initial vitrectomies. In all 10 eyes, the initial regular macular hole surgery with ILM removal or enlargement of the ILM-peeled area failed to close the macular holes. We measured the size of the macular holes parallel to the retinal pigment epithelium at the nearest point of retinal apposition. Macular hole closure was defined as the absence of a neurosensory defect over the fovea.
All patients underwent comprehensive ophthalmologic examinations, including measurement of best-corrected visual acuity (BCVA) with refraction using the 5-m Landolt C acuity chart and indirect and contact lens slit-lamp biomicroscopy. Spectral-domain optical coherence tomography (SD OCT) examinations were performed before and after surgery and at follow-up in all eyes using commercially available instruments (Cirrus [Carl Zeiss Meditec, Inc., Dublin, California, USA] or Spectralis [Heidelberg Engineering GmbH, Heidelberg, Germany]).
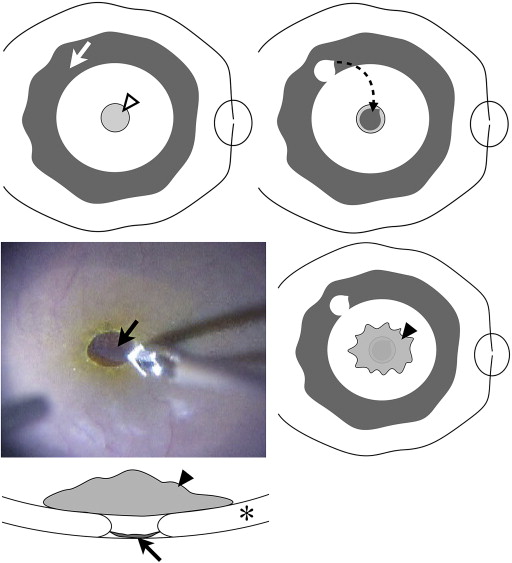
Surgical Techniques
All patients underwent 25-gauge, transconjunctival, sutureless microincision vitrectomy. All surgeries were performed by the same surgeon (F.S.). The residual ILM first was stained with 0.25 mg/mL brilliant blue G solution (Coomassie BBG 250; Sigma-Aldrich, St. Louis, Missouri, USA) to identify the area where the ILM had been peeled off in previous surgery ( Figure 1 ). We then peeled off a small piece of the ILM to create a free flap, so that its diameter was almost the same in diameter as the macular hole to be repaired. To avoid losing sight of the free flap of ILM, we turned off the infusion line and placed the free flap inside the macular hole. We then placed a low molecular weight viscoelastic material (Opegan; Santen Pharmaceutical Co, Ltd, Osaka, Japan) over the free flap of ILM to stabilize it, and this was left in the eye. Immediately after reopening the infusion line, we performed fluid–air exchange, keeping the extrusion needle away from the macula. At the end of the operation, the air was replaced with 10% sulfur hexafluoride gas. Patients were asked to remain face down for 3 days after surgery ( Supplemental Video available at AJO.com ).
Data Analysis
BCVA was recorded as decimal values and converted to the logarithm of the minimal angle of resolution units for statistical analysis. All visual acuity results are presented in logarithm of the minimal angle of resolution units. To evaluate the surgical outcomes, the preoperative and postoperative BCVA were compared using the paired t test. A P value of less than .05 was considered significant. All statistical analyses were performed using SPSS for Windows version 17.0 (SPSS, Inc., Chicago, Illinois, USA). Data are presented as mean ± standard deviation.
Results
The characteristics of the 10 patients who were enrolled in this study are shown in the Table . The mean age of the 6 female and 4 male patients was 60.6 ± 19.5 years (range, 17 to 83 years). The mean follow-up period was 12 ± 5 months (range, 3 to 18 months). The mean diameter of the macular holes before autologous transplantation of the ILM was 509.3 ± 137.8 μm (range, 281 to 789 μm). The lens status of the eyes was unchanged after autologous transplantation of the ILM. Intraocular lenses had been inserted in 8 eyes (80%), and the other 2 eyes (20%) were phakic.
| Patient No. | Age (y) | Sex | Follow-up (m) | Primary Disease | Initial Size of Macular Hole (μm) | Size of Macular Hole after Initial Surgical Repair (μm) | Macular Hole Status (after Internal Limiting Membrane Transplantation) | Visual Acuity | Lens Status | |
|---|---|---|---|---|---|---|---|---|---|---|
| Before Surgery | Final | |||||||||
| 1 | 51 | Male | 18 | Myopic foveoschisis | — | 450 | Closed | 1.30 | 0.40 | Pseudophakic |
| 2 | 65 | Female | 16 | Myopic foveoschisis | — | 479 | Closed | 1.15 | 0.70 | Pseudophakic |
| 3 | 78 | Female | 16 | Foveoschisis resulting from pit-macular syndrome | — | 430 | Closed | 1.30 | 1.05 | Pseudophakic |
| 4 | 83 | Female | 15 | Large macular hole | 789 | — | Open | 1.10 | 1.00 | Pseudophakic |
| 5 | 65 | Female | 15 | Large macular hole | 592 | — | Closed | 1.00 | 0.15 | Pseudophakic |
| 6 | 66 | Female | 12 | Large macular hole | 516 | — | Closed | 0.52 | 0.22 | Pseudophakic |
| 7 | 72 | Male | 11 | Large macular hole | 474 | — | Closed | 0.70 | 0.22 | Pseudophakic |
| 8 | 68 | Male | 9 | Proliferative diabetic retinopathy | — | 640 | Closed | 1.05 | 1.05 | Pseudophakic |
| 9 | 17 | Male | 5 | Traumatic macular hole | 442 | — | Closed | 0.82 | 0.40 | Phakic |
| 10 | 41 | Female | 3 | Foveoschisis resulting from pit-macular syndrome | — | 281 | Closed | 1.00 | 0.52 | Phakic |
Macular hole closure was achieved after autologous trans- plantation of the ILM in 9 eyes (90%). In only 1 eye (10%; Patient 4), in which a large macular hole had existed for more than 3 years, was the procedure unsuccessful. In the 9 eyes (90%) in which the macular holes closed after autologous transplantation of the ILM, the transplanted ILM flaps were visible as highly reflective areas on SD OCT within 7 days of autologous transplantation of the ILM. These highly reflective areas disappeared within 3 months. The mean BCVA was 0.99 ± 0.25 (range, 0.52 to 1.30) before surgery and 0.57 ± 0.36 (range, 0.15 to 1.05) at the final visit. This showed a significant difference in BCVA before and after autologous transplantation of the ILM ( P = .007). The postoperative BCVA improved by more than 0.2 logMAR in 8 eyes (80%), but was unchanged in 2 eyes (20%; Figure 2 ). No complications occurred during surgery or after surgery in any cases.
Figures 3 and 4 show the clinical results for 2 patients who underwent autologous transplantation of the ILM for large macular holes. SD OCT images show the macular hole closure achieved after autologous transplantation of the ILM. Figure 5 shows similar results for the patient who sought treatment with a traumatic macular hole, choroidal rupture, and subretinal fibrosis. Similarly, the initial regular macular hole surgery, in which the ILM was removed, did not result in any success. However, after we performed autologous transplantation of the ILM at the second surgery, the macular hole was closed successfully, resulting in an improvement in visual acuity. The clinical results of autologous transplantation of the ILM for 1 of the 2 patients with foveoschisis resulting from pit-macular syndrome are shown in Figure 6 . Again, the SD OCT images show a successful outcome after autologous transplantation of the ILM.



