Key points
- •
Effect, directly or indirectly, is on neural processing of auditory stimuli.
- ○
Physiologic measures are needed to accurately characterize patients with auditory neuropathy spectrum disorder (ANSD).
- ○
Clinical behavioral responses vary greatly and are not useful diagnostic measures.
- ○
- •
Patients with ANSD have greater difficulty listening in noise than those with other types of hearing disorders.
- ○
Separating detection ability from discrimination ability is critical in considering various management approaches.
- ○
- •
Without clear auditory input, visual information is needed for auditory communication and speech/language development.
- •
Many patients benefit from cochlear implants; fewer benefit from hearing aids.
- •
Patients should be followed closely, as changes in auditory function may occur over time.
| ABR | Auditory brainstem response |
| AN | Auditory neuropathy |
| AN/AD | Auditory neuropathy/auditory dys-synchrony |
| ANSD | Auditory neuropathy spectrum disorder |
| APD | Auditory processing disorder |
| CM | Cochlear microphonic |
| EVA | Enlarged vestibular aqueduct |
| FM | Frequency modulation |
| HMSN | Hereditary motor sensory neuropathy |
| IHC | Inner hair cells |
| MEMR | Middle-ear muscle reflex |
| MOCR | Medial olivocochlear reflex |
| NICU | Neonatal intensive care unit |
| OAE | Otoacoustic emission |
| OHC | Outer hair cells |
| OTOF | Otoferlin |
| SNHL | Sensorineural hearing loss |
Auditory neuropathy (AN), auditory neuropathy/dys-synchrony (AN/AD), and, more recently, auditory neuropathy spectrum disorder (ANSD) are variable terms used to describe an auditory disorder seen in patients ranging in age from infants to adults. With knowledge of the inherent problems presented by each term, ANSD is used here with the understanding that no one term is completely definitive or descriptive.
Overview of characteristics
ANSD is characterized by evidence of intact outer hair cell (OHC) function, shown by the presence of otoacoustic emissions (OAEs) and/or cochlear microphonics (CMs), accompanied by poor eighth nerve–brainstem responses, demonstrated by absent or highly abnormal auditory brainstem responses (ABRs). Further evidence of effects on neural function is demonstrated by absent or elevated middle-ear muscle reflexes (MEMRs) and abnormal medial olivocochlear reflexes (MOCRs). Although understanding of speech in noise is poorer than that observed in sensorineural hearing loss (SNHL), word recognition in quiet is highly variable, and thresholds for pure tones range from normal to profound losses. Most ANSD patients show bilateral characteristics, although function may be asymmetric between ears, and patients with unilateral ANSD have been documented.
Despite fairly similar findings on auditory physiologic measures, patients vary considerably in functional communication abilities. Clinical presentation typically includes difficulty listening in noise, may include fluctuating hearing ability, and, in the case of infants and children, most often involves delays in speech and language development. Patients with ANSD typically demonstrate poor temporal resolution and may have neural deficits in other systems.
Overview of characteristics
ANSD is characterized by evidence of intact outer hair cell (OHC) function, shown by the presence of otoacoustic emissions (OAEs) and/or cochlear microphonics (CMs), accompanied by poor eighth nerve–brainstem responses, demonstrated by absent or highly abnormal auditory brainstem responses (ABRs). Further evidence of effects on neural function is demonstrated by absent or elevated middle-ear muscle reflexes (MEMRs) and abnormal medial olivocochlear reflexes (MOCRs). Although understanding of speech in noise is poorer than that observed in sensorineural hearing loss (SNHL), word recognition in quiet is highly variable, and thresholds for pure tones range from normal to profound losses. Most ANSD patients show bilateral characteristics, although function may be asymmetric between ears, and patients with unilateral ANSD have been documented.
Despite fairly similar findings on auditory physiologic measures, patients vary considerably in functional communication abilities. Clinical presentation typically includes difficulty listening in noise, may include fluctuating hearing ability, and, in the case of infants and children, most often involves delays in speech and language development. Patients with ANSD typically demonstrate poor temporal resolution and may have neural deficits in other systems.
Incidence
ANSD occurs in about 10% of individuals who have a dys-synchronous ABR, or an ABR consistent with an estimate of severe or profound hearing loss. This estimate is based on data from several sources that include screening of more than 1000 children enrolled in schools for the d/Deaf in North America, a similar smaller-scale study in Hong Kong, a hospital-based study of children in Australia, and a multicenter newborn screening study in the United States. A higher incidence of 17.3% and 15.4%, respectively, was reported among children identified with hearing loss following newborn hearing screening. In the neonatal intensive care unit (NICU), rates of ANSD physiologic characteristics ranged from 24% to 40% of infants who failed ABR testing in one or both ears.
Clinical findings
Physiologic measures that assess cochlear active processes related to OHC and mechanical activity and peripheral neural function of the eighth nerve and brainstem pathways most accurately describe patients with ANSD. Cochlear processes are evidenced by the presence of OAEs and CMs. Clinical tests specifically sensitive to auditory nerve dysfunction are the ABR, MEMRs, and the MOCR. Of these measures, OAEs and ABR together form the most sensitive combination. A summary of physiologic and behavioral audiologic test results in patients with ANSD is shown in Table 1 .
| Test | Outcome |
|---|---|
| Otoacoustic emissions | Typically present |
| Middle-ear muscle reflexes | Typically absent |
| Cochlear microphonic | Present (inverts with stimulus polarity reversal) |
| Auditory brainstem response | Absent or severely abnormal |
| Pure-tone thresholds | Normal to severe/profound hearing loss |
| Word recognition in quiet | Variable; slightly reduced to greatly reduced |
| Word recognition in noise | Generally poor |
| Medial olivocochlear reflex | Typically absent |
Hair Cell Responses: Otoacoustic Emissions and Cochlear Microphonics
OAEs provide a measure of cochlear active processes related to OHC function and cochlear mechanics. The presence of ANSD is typically established based on presence of these responses when peripheral neural responses are absent or significantly reduced. In the absence of middle-ear disorders, OAEs are typically present in patients with ANSD. Because OAEs are low-amplitude acoustic signals, even small middle-ear changes can be sufficient to reduce OAE amplitude or prevent the OAE from being recorded. The effect of even minor middle-ear problems and the high incidence of otitis media in infants and children can confound identification of ANSD.
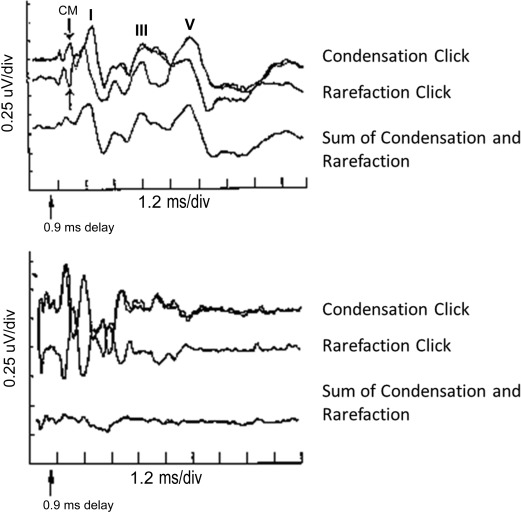
Cochlear function can also be evaluated using the CM. Because the CM is an electrical response, it does not depend on reverse transmission through the middle ear system. A key factor in distinguishing CM from neural responses is the reversal of the electrical response with presentation of condensation versus rarefaction stimuli. The CM will invert with stimulus polarity reversal, whereas neural responses to clicks typically do not completely invert ( Fig. 1 ).
Neural Responses: Auditory Brainstem Response
ABRs are most often absent in patients with ANSD, although some patients demonstrate small evidence of neural synchrony for high-level stimuli. In the germinal article defining AN, Starr and colleagues reported absent ABRs in 9 of 10 patients and an abnormal ABR characterized by Wave V responses only to high-intensity stimuli in 1 patient. A subsequent review of ABR data for 186 patients with ANSD indicated that approximately 75% of patients had absent ABRs while 25% showed abnormal responses characterized by the presence of low-amplitude Wave V only at high stimulus levels (75–90 dB nHL).
The absence or abnormality of all components of the ABR including Wave I suggests that the distal portion of the eighth nerve is affected, either directly or indirectly, in ANSD. This characteristic distinguishes patients with ANSD from those with space-occupying lesions affecting the eighth nerve where ABR Wave I is present. Imaging studies (MRI, computed tomography) are characteristically normal in patients with ANSD. Neural changes in ABR are attributed to demyelinating and axonal neuropathies.
Neural Responses: Efferent Acoustic Reflexes
Both ipsilaterally and contralaterally elicited MEMRs are most often absent in these patients, although a small percentage (about 10%) of patients may display MEMRs at elevated levels or in combination with absent responses. The MOCR assesses changes in OAEs when the olivocochlear neural pathway, terminating at the cochlear OHCs, is activated. Although patients with ANSD typically demonstrate the presence of OAEs, they consistently show no or minimal suppression of transient OAEs for binaural, ipsilateral, and contralateral suppressor stimuli. Abnormalities in both reflexes seem to be related to poor afferent auditory input, based on both the ability to elicit nonacoustic reflexes and studies in patients with unilateral ANSD.
Behavioral Findings: Pure-Tone Thresholds and Speech Recognition
Pure-tone thresholds and speech recognition, particularly in quiet, are the least informative measures in the evaluation of ANSD. Pure-tone thresholds range from normal sensitivity to severe or profound hearing loss. Some patients show rising or unusual configurations with possible asymmetry between ears. When OAEs are present and pure-tone thresholds are poorer than expected for the presence of OAEs, this combination may provide a clue to the presence of ANSD or another type of neural disorder that warrants further investigation.
Speech recognition in ANSD patients is typically poorer than expected based on pure-tone thresholds, but performance varies widely across individuals. Some patients with ANSD demonstrate word-recognition ability in quiet in ranges similar to those with SNHL, whereas word-recognition ability in noise is clearly below that expected in SNHL. Of 68 patients aged 4 years and older in whom word recognition was measurable using standardized tests, more than half had no word-recognition ability, even in quiet. Of the remaining patients, 30 had word-recognition scores greater than 0% in quiet and only 5 patients had measurable word recognition in noise. This widely varying ability presents a particular challenge in both understanding ANSD and planning appropriate management.
Underlying mechanisms
The set of clinical test results observed in patients with ANSD can occur as a result of absence or disruption of inner hair cell (IHC) activity, disorders of the auditory nerve, or abnormalities at the synapses of the IHCs and auditory nerve. IHC abnormalities could result from a lack of development, traumatic insult, or a loss over time. Selective IHC loss was observed in several premature newborns who failed ABR testing. Hypoxia and toxic insults specific to IHCs are other possible explanations. Direct effects on auditory nerve activity have been implicated in patients with concomitant peripheral neuropathies such as Charcot-Marie-Tooth disease, Friedreich ataxia, Mohr-Tranebjaerg syndrome who also display characteristics of ANSD. Study of underlying mechanisms is enhanced through efforts to distinguish presynaptic versus postsynaptic responses using electrocochleography.
Links between ANSD and genetic mutations are well documented with evidence of recessive, dominant, and mitochondrial inheritance patterns, and occurrence in syndromic and nonsyndromic hearing loss (see Ref. for review). An example is the OTOF gene that encodes otoferlin, whose mutations are associated with nonsyndromic recessive ANSD. Otoferlin plays a role in neurotransmitter release at the synapse between the IHCs and the auditory nerve.
In some patients with ANSD, fluctuations in auditory function have been linked to fluctuations in body temperature (as little as 1°C) and an apparent temperature-sensitive form of ANSD. Several reports implicate OTOF gene mutations and other mechanisms, possibly autoimmune disorders, whereby auditory function varies with changes in body temperature. ANSD is also reported in infants with potential risk factors that include hypoxia and hyperbilirubinemia.
Differential diagnosis
Although the test protocols necessary to diagnose ANSD are now well established, dysfunction of the IHCs and their synapses can lead to a hearing disorder that is difficult to distinguish clinically from an auditory nerve disorder. Identifying concomitant peripheral neuropathies or radiologic abnormalities is helpful in distinguishing among various conditions.
Association with Other Neurologic Abnormalities
Several neurologic problems are identified in patients with ANSD, including hereditary motor sensory neuropathy (HMSN), Charcot-Marie-Tooth disease, Friedreich ataxia, Mohr-Tranebjaerg syndrome, gait ataxia, loss of deep tendon reflexes, or motor system disturbances. The motor neural system may be affected without accompanying sensory problems involving the auditory system. When the auditory system is affected, characteristics such as absent or highly abnormal ABRs with preserved OAEs provide evidence consistent with ANSD. Broad variation in auditory characteristics such as speech understanding exists, likely related to underlying genetic characteristics in addition to the stage in the progression of the disorder.
Cochlear Nerve Deficiency
Absent or hypoplastic auditory nerves are not uncommon, and these conditions resemble ANSD when OHC responses are present. Audiologic management in these patients is problematic because a cochlear implant cannot work when the nerve is absent, and might not work well when the cochlear nerve is hypoplastic.
Enlarged Vestibular Aqueduct
Patients with an enlarged vestibular aqueduct (EVA) present with a wide variety of audiometric thresholds and physiologic results, and may demonstrate clinical characteristics consistent with ANSD. EVA is associated with SNHL, onset from birth to adolescence, progression, fluctuation, the possibility of other congenital ear anomalies, and contributing factors such as head trauma. Not all cases of EVA will show clinical test results consistent with ANSD.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


