Asthma is a chronic inflammatory disease of the airway that leads to airway obstruction via bronchoconstriction, edema, and mucus hypersecretion. The National Asthma Education and Prevention Program has outlined evidence-based guidelines to standardize asthma therapy and improve outcomes. The initial recommendation of choice for persistent asthmatic patients is an inhaled corticosteroid (ICS). Long-acting beta-2 agonists in combination with ICS, oral corticosteroids, leukotriene modifiers, and anti-IgE therapeutic options can be considered for patients with persistent or worsening symptoms. Many novel therapies are being developed, with an emphasis on anti-inflammatory mechanisms, gene expression, and cytokine modification.
Key points
- •
Inhaled SABAs are the preferred medication for intermittent asthma symptoms and acute reversal of bronchoconstriction.
- •
Persistent asthma symptoms are preferably managed with inhaled corticosteroids (ICSs) with or without adjunctive therapy consisting of LTRAs, zileuton, or theophylline.
- •
Particle size of inhalers plays a key role in lung deposition and hence effectiveness.
- •
Omalizumab, anti-IgE therapy injection, has been indicated as an adjunct for persistent allergic patients with asthma uncontrolled with ICS+LABA combination therapy with a low risk of anaphylaxis after injection.
- •
Many novel asthma therapies are being investigated that target gene expression, anti-inflammatory mechanisms, and steroid resistance.
Introduction
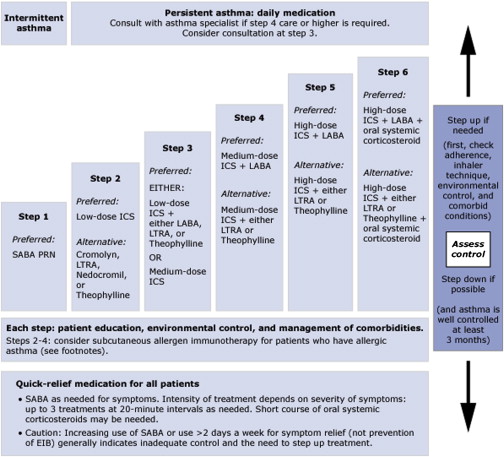
Asthma represents a chronic inflammatory process marked by bronchial hyperactivity, mucus hypersecretion, and airway edema that leads to airway obstruction. These changes in the airway initially are reversible, but with continued airway remodeling the extent of reversibility may vary, leading to more difficult management. The goals of asthma pharmacotherapy are to reverse the inflammatory state and airway obstruction. The National Asthma Education and Prevention Program (NAEPP) Expert Panel has devised evidence-based guidelines for asthma care, including recommendations for therapy based on asthma severity ( Fig. 1 ).
Introduction
Asthma represents a chronic inflammatory process marked by bronchial hyperactivity, mucus hypersecretion, and airway edema that leads to airway obstruction. These changes in the airway initially are reversible, but with continued airway remodeling the extent of reversibility may vary, leading to more difficult management. The goals of asthma pharmacotherapy are to reverse the inflammatory state and airway obstruction. The National Asthma Education and Prevention Program (NAEPP) Expert Panel has devised evidence-based guidelines for asthma care, including recommendations for therapy based on asthma severity ( Fig. 1 ).
Beta-2 agonists
Short-Acting Beta-2 Agonists
Short-acting beta-2 agonists (SABAs), such as albuterol and levalbuterol, are recommended for intermittent asthma symptoms and serve to immediately reverse bronchoconstriction via potent bronchodilation. The mechanism of action is via a selective interaction on beta-2 receptors of bronchial smooth muscle to achieve bronchodilation. SABAs are the preferred medication for acute asthma exacerbations as a rescue inhaler due to the quick onset of bronchodilation. Regular use of SABAs is not recommended because of the development of tachyphylaxis and increased hyper responsiveness.
Long-Acting Beta-2 Agonists
Long-acting beta-2 agonists (LABAs), salmeterol and formoterol, provide approximately 12 hours of bronchodilation. The mechanism by which LABAs provide long-acting effects has not been clearly delineated. Multiple mechanisms have been described in the development of once-daily ultra- LABA preparations, including partitioning of the drug into lipophilic compartments after inhalation forming small depots of the drug, the presence of small lipid rafts in airway smooth muscle, and the tight binding to beta-2 adrenoreceptor and formation of ternary complexes.
Since 2005, LABAs are no longer recommended as sole agents for the management of asthma. In 1993, Castle and colleagues, in a study using salmeterol, showed convincing evidence that mortality increased threefold in patients with asthma, which led to a study influenced by the Food and Drug Administration (FDA), the Salmeterol Multicentre Asthma Research Trial (SMART) study in 1996. The study was aborted due to increased exacerbations and mortality. Subsequent studies using formoterol in higher doses demonstrated increased exacerbations as well.
LABAs are currently recommended as a combination therapy with corticosteroids based on an FDA 2008 meta-analysis showing no significant safety risks. Per NAEPP guidelines, the use of LABAs + inhaled corticosteroids (ICSs) is indicated in persistent asthma uncontrolled with ICSs alone. Three preparations are available: budesonide/formoterol, mometasone/formoterol, and fluticasone/salmeterol.
A 2011 meta-analysis comparing fluticasone/salmeterol with budesonide/formoterol showed no significant difference between the 2 preparations as it relates to oral steroid requirements, hospital admissions, rescue inhaler use, and lung function. Another comparison study demonstrated that the odds of bronchodilation within 5 minutes was almost 4 times higher with fluticasone/formeterol over fluticasone/salmeterol, suggesting that this benefit may influence patient compliance with medication. In an effort to manage patients with asthma using the lowest effective dose of ICS/LABA, Hojo and colleagues proposed a step-down protocol to avoid asthma exacerbations. Patients were controlled on budesonide/formoterol at 640/18 μg (4 puffs/day) followed by step-down to 320/9 μg/day (2 puffs/day) when either the forced expired nitric oxide (FeNO) decreased to 28 or lower while the asthma control test (ACT) was 22 or higher or the ACT was 24 points or higher at 3 consecutive visits. After a 48-week study period, asthma control was stable based on SABA use and the number of acute exacerbations.
The selectivity of beta-2 agonists over alpha and beta-1 receptors results in fewer cardiac side effects, such as tachycardia and palpitations. Levalbuterol is an entamer of albuterol associated with even fewer cardiac side effects. Use of beta-2 agonists in diabetic patients is cautioned because of the risk of ketoacidosis related to induction of liver glycogenolysis via beta-adrenoreceptor. Other adverse reactions include hypokalemia, tremor, irritation, or anxiety after use.
Anticholinergics
Anticholinergic agents, primarily ipratroprium, also function as bronchodilators by inhibiting the vagal muscarinic receptors on smooth muscle. These agents can be effective especially in patients who do not tolerate SABAs. Tiotropium, a long-acting antimuscarinic, has been shown to be an effective bronchodilator in chronic obstructive pulmonary disease (COPD) and investigators have also shown tiotropium to be effective in asthma. Kerstjens and colleagues demonstrated in 2 randomized controlled trials that tiotropium improved asthma control in patients with poorly controlled asthma on ICSs and LABAs. Tiotropium was administered as 2 puffs of 2.5 μg via mist inhaler in addition to any previous asthma medications before the trial. After a 48-week trial period, the investigators observed an improvement in forced expiratory volume in 1 second (FEV1) in the first 24 weeks with an overall reduction in the risk of a severe exacerbation by 21% compared with placebo.
Corticosteroids
The mechanism of action of corticosteroids is complex, involving cellular and molecular mechanisms having direct and indirect influences on the airway. In general, corticosteroids have been shown to enhance the beta-adrenergic response that relieves muscle spasm, reverse edema by decreasing vascular permeability and the inhibition of leukotriene C4 (LTC4) and LTD4, decrease mucus by inhibiting macrophage release of secretagogue, and inhibit chemotaxis to reverse inflammatory response. The binding of glucocorticoid receptors triggers multiple genes involved in regulating airway inflammation ( Box 1 ).
Increased transcription
Annexin-1 (lipocortin-1, phospholipase A 2 inhibitor)
Beta-2 adrenoceptors
Clara cell protein (CC10, phospholipase A 2 inhibitor)
Glucocorticoid-induced leucine zipper protein
IL-1 receptor antagonist
IL-1 receptor 2 (decoy receptor)
Inhibitor of NF-κB (IκB-α)
IL-10
Mitogen-activated protein kinase phosphatase-1
Secretory leukoprotease inhibitor
Decreased transcription
Cytokines
IL-1, IL-2, IL-3, IL-4, IL-5, IL-6, IL-9, IL-11, IL-12, IL-13, IL-16, IL-17, IL-18, TNFα, GM-CSF, stem cell factor
Chemokines
IL-8, RANTES, MIP-1α, MCP-1, MCP-3, MCP-4, eotaxins
Adhesion molecules
E-selectin, ICAM-1, VCAM-1
Inflammatory enzymes
Cytoplasmic phospholipase A 2
Inducible cyclooxygenase (COX-2)
Inducible nitric oxide synthase
Inflammatory receptors
Bradykinin Beta-2 receptors
Tachykinin NK 1 -receptors, NK 2 -receptors
Peptides
Endothelin-1
Abbreviations: GM-CSF, granulocyte-macrophage colony stimulating factor; ICAM, intercellular adhesion molecule; IL, interleukin; MCP, monocyte chemoattractant protein; MIP, macrophage inflammatory protein; RANTES, released by normal activated T cells expressed and secreted; TNF, tumor necrosis factor; VCAM, vascular-endothelial cell adhesion molecule.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


