Purpose
To quantify the predictive strength of anterior chamber area (ACA), anterior chamber volume (ACV), anterior chamber width (ACW), lens vault (LV), iris thickness (IT), and iris area (IArea) for 2 angle width parameters, trabecular–iris space area (TISA750) and angle opening distance (AOD750) at 750 μm from the scleral spur, in different ethnicities.
Design
Prospective, cross-sectional study.
Methods
Anterior segment optical coherence tomography images for 166 white, 90 African, 75 Hispanic, and 132 Chinese subjects were analyzed. First, ACA, ACV, ACW, LV, IT, and IArea were compared among ethnic groups. Second, associations of TISA750 and AOD750 with ACA, ACV, ACW, LV, IT, and IArea were investigated within each ethnic group using multivariable linear regression models, standardized regression coefficients (β), and coefficients of determination (R 2 ).
Results
Significant ethnic differences were observed in ACA, ACV, ACW, LV, IT, and IArea (all P < .05). ACA, ACV, and LV were significant predictors of TISA750 and AOD750 in all ethnic groups (all P < .001). ACW and IT were significant predictors of AOD750 in white and African subjects (all P < .05). ACW and IT were significant predictors of TISA750 in white subjects (all P < .05). IArea was a significant predictor of AOD750 in Chinese ( P < .05). ACA, ACV, and LV had the highest predictive strength for both TISA750 and AOD750 in all ethnic groups based on β and R 2 .
Conclusions
Despite ethnic differences in ACA, ACV, ACW, LV, IT, and IArea, the same 3 anterior segment parameters (ACA, ACV, and LV) were the strongest predictors of angle width (TISA750 and AOD750) in all 4 ethnic groups.
Primary angle closure glaucoma (PACG) is one of the leading causes of irreversible blindness worldwide. Although this condition is most commonly described among those of Asian descent, it can occur in all races. A review of the literature published between the years 1966 and 2006 indicated reproducible evidence of ethnic variations in the prevalence of PACG. Evaluation of the anterior chamber angle width is considered the key factor in diagnosis, since this anatomic parameter primarily determines the risk for PACG development. One method of quantifying angle width is by using diagnostic imaging modalities such as anterior segment optical coherence tomography (AS OCT). Analysis of AS OCT images with customized software, the Zhongshan Angle Assessment Program (Zhongshan Ophthalmic Centre, Guangzhou, China), allows objective and reproducible quantification of anterior segment biometric parameters.
Two parameters that closely reflect angle width are trabecular–iris space area and angle opening distance. Foo and associates showed in Chinese subjects that angle width is largely dependent on variations in anterior chamber area, anterior chamber volume, anterior chamber width, lens vault, iris thickness measured at 750 μm from the scleral spur, and iris area. Using a predictive mathematical model composed of these 6 anterior segment biometric parameters, their study explained 81.4% of the variability in trabecular–iris space area at 750 μm from the scleral spur and 85.5% of the variability in angle opening distance at 750 μm from the scleral spur.
However, their findings in an ethnic Chinese population may not necessarily apply to other ethnic groups. Quantifying the predictive ability of anterior segment biometric parameters associated with anterior chamber angle width in various ethnic groups can provide insight into mechanisms of angle closure in different ethnicities. The purpose of the present study was to objectively compare the predictive strength of anterior chamber area, anterior chamber volume, anterior chamber width, lens vault, iris thickness measured at 750 μm from the scleral spur, and iris area for anterior chamber angle width among white, African, Hispanic, and Chinese populations.
Methods
Approval for this prospective, cross-sectional, single-center, multiethnic, clinic-based study was obtained from the University of California, San Francisco (UCSF) Committee on Human Research. The study was carried out in accordance with the tenets of the Declaration of Helsinki and written consent was obtained from all patients. The study population was composed of 4 different ethnic cohorts (white, African, Hispanic, and Chinese) consecutively recruited from the UCSF general ophthalmology and glaucoma clinics between March 1, 2008 and September 28, 2010. Ethnicities were self-designated by the patients.
Inclusion criteria for subject enrollment included: (1) adult patients (age >18 years); (2) patients who consented to undergo standardized ophthalmic examination and AS OCT imaging; (3) absence of corneal abnormalities that may obscure the view of anterior segment structures; (4) absence of prior laser or incisional eye surgery; (5) absence of previous ocular trauma; and (6) self-reported white, African, Hispanic, and Chinese ancestry in both parents (the term “white” for the purposes of this study included only European-derived whites). Exclusion criteria for enrollment included the following: (1) aphakic or pseudophakic eyes; (2) inability to complete the standardized ophthalmic examination and AS OCT imaging; and (3) poor AS OCT imaging quality (evaluated on the basis of corneal reflection, continuity of anterior segment structures, motion artifacts, and indeterminate scleral spurs).
All enrolled subjects received intraocular pressure measurement by Goldmann applanation tonometry (model AT900; Haag-Streit AG, Koeniz, Switzerland), central corneal thickness measurement by ultrasound pachymetry (Model DGH-550 Pachette 2; DGH Technology Inc, Exton, Pennsylvania, USA), manual refraction, and gonioscopy with a Zeiss-style 4-mirror lens (Model OPDSG; Ocular Instruments, Inc, Bellevue, Washington, USA). A single trained ophthalmologist (Shan C. Lin) performed gonioscopy at 16 × magnification with slit-lamp biomicroscopy in a darkroom setting. The study population was further categorized into narrow-angle and open-angle groups. The Shaffer gonioscopic classification was used to determine the anterior chamber angle grading in all 4 quadrants: an angle between the iris and the trabecular meshwork surface of 35–45 degrees was classified as grade 4, between 20 and 35 degrees was classified as grade 3, between 10 and 20 degrees was classified as grade 2, and less than 10 degrees was classified as grade 1. Grade 0 was assigned if angle structures were not observed. For this study, eyes with narrow angles were defined as those with Shaffer grades of 2 or less in 3 or more quadrants, whereas eyes with open angles were defined as those with Shaffer grades of 3–4 in 3 or more quadrants. This definition of narrow angle has previously been used by other studies. Both the narrow-angle and open-angle groups included nonglaucomatous and glaucomatous subjects.
Anterior Segment Optical Coherence Tomography
All qualified study subjects received imaging in the dark with AS OCT (Visante OCT; Carl Zeiss Meditec, Inc, Dublin, California, USA), a noncontact optical coherence tomographic system using 1310-nm-wavelength light to capture high-resolution cross-sectional images of the anterior segment of the eye. AS OCT imaging was performed under standardized dark conditions with illuminations below 1 lux as measured by EasyView Digital Light Meter (Model EA30; Extech Instruments, Inc, Waltham, Massachusetts, USA). Patients were allowed 5 minutes for dark adaptation before image acquisition. Each AS OCT scan captured both the temporal and nasal quadrants (nasal-temporal 0–180 degrees) in a single image while the patient looked straight ahead. An experienced operator, masked to the standardized ophthalmic examination findings, performed all the AS OCT scans. Three to 5 images were acquired for the 1 randomly selected eye of each subject and the image with the best quality was selected for analysis using the Zhongshan Angle Assessment Program. Image quality was evaluated on the basis of a steady central fixation as judged by a clear corneal reflection, good visibility of the scleral spurs, the presence of continuity in anterior segment structures, and the absence of motion artifacts.
The Zhongshan Angle Assessment Program contained algorithms that automatically defined the borders and curvatures of anterior segment structures after the scleral spurs were localized manually on the AS OCT images. Measurements for both the nasal and temporal angles were simultaneously produced, but only the nasal angles were analyzed in this study. This procedure has previously been used in our other studies. The following parameters were derived from the Zhongshan Angle Assessment Program: trabecular–iris space area at 750 μm from the scleral spur, angle opening distance at 750 μm from the scleral spur, anterior chamber area, anterior chamber volume, anterior chamber width, lens vault, iris thickness measured at 750 μm from the scleral spur, iris area, and pupil diameter.
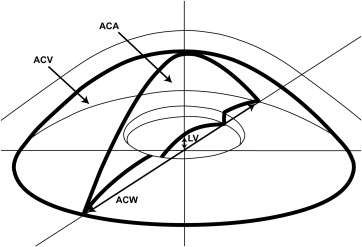
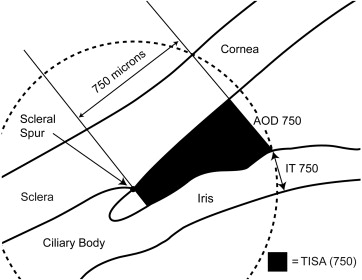
The above listed AS OCT parameters were defined previously in other studies. Trabecular–iris space area at 750 μm from the scleral spur was defined as the trapezoidal area with the following boundaries: anteriorly, a perpendicular line between the inner corneoscleral wall and the iris surface at 750 μm anterior to the scleral spur; posteriorly, a line perpendicular to the inner corneoscleral wall extending from the scleral spur to the iris surface; superiorly, the inner corneoscleral wall; and inferiorly, the iris surface. Angle opening distance at 750 μm from the scleral spur was defined as the length of the line extending from the anterior iris to the corneal endothelium, perpendicular to the line drawn along the trabecular meshwork at 750 μm anterior to the scleral spur. Anterior chamber area was defined as the cross-sectional area of the anterior chamber bounded by the corneal endothelium anteriorly, and the anterior surface of the iris and the anterior surface of the lens (within the pupil) posteriorly. Anterior chamber volume was calculated by rotating the anterior chamber area 360 degrees around a vertical axis through the mid-point of the anterior chamber area. Anterior chamber width was defined as the horizontal scleral spur-to-spur distance. Lens vault was defined as the perpendicular distance between the anterior pole of the crystalline lens and the horizontal line joining the 2 scleral spurs. An illustration of anterior chamber area, anterior chamber volume, anterior chamber width, and lens vault is provided in Figure 1 . For iris thickness, a circle centered at the scleral spur was drawn with a radius of 750 μm, and the point of intersection between the circle and the anterior surface of the iris was identified. The shortest distance from this point to the posterior surface of the iris was calculated as iris thickness measured at 750 μm from the scleral spur. An illustration of trabecular–iris space area at 750 μm from the scleral spur, angle opening distance at 750 μm from the scleral spur, and iris thickness measured at 750 μm from the scleral spur is provided in Figure 2 . Iris area was calculated as the cumulative cross-sectional area of the full length of the iris. Pupil diameter was calculated by measuring the distance between the pupil edges on the cross-sectional images.
Statistical Analysis
For analysis, 1 eye was selected for each subject. The default protocol was to use images from the right eye for analysis. However, the left eye’s data were used when the right eye did not meet the inclusion criteria. For each ethnic group, mean and standard deviation were calculated for all variables. Comparisons were made between ethnic groups for subjects with only narrow angles, only open angles, and both narrow and open angles. A P value <.05 was considered statistically significant. Continuous data were analyzed using 1-way analysis of variance with Tukey post hoc test for between–ethnic group comparisons. Continuous data were analyzed using independent Student t tests for within–ethnic group comparisons. Categorical data were analyzed with Pearson χ 2 test. Multivariable linear regression models were used to investigate the association of trabecular–iris space area at 750 μm from the scleral spur and angle opening distance at 750 μm from the scleral spur with anterior chamber area, anterior chamber volume, anterior chamber width, lens vault, iris thickness measured at 750 μm from the scleral spur, and iris area, while controlling for age, sex, pupil diameter, and spherical equivalent. Both standardized regression coefficients (β) and coefficients of determination (R 2 ) were calculated from the multivariable linear regression models. To determine the effects of glaucoma on the association of trabecular–iris space area at 750 μm from the scleral spur and angle opening distance at 750 μm from the scleral spur with anterior chamber area, anterior chamber volume, anterior chamber width, lens vault, iris thickness measured at 750 μm from the scleral spur, and iris area, the same multivariable linear regression models were applied to only nonglaucomatous subjects. Spherical equivalent was derived from the refraction using the following formula: sphere plus half of the cylinder. All statistical analyses were performed with JMP statistical software (Ver. 10.0; SAS Institute, Cary, North Carolina, USA). AS OCT images were analyzed with Zhongshan Angle Assessment Program. Scleral spurs were localized by a single observer (B.C.) while masked to the patient’s ophthalmic examination results. To evaluate intraobserver reproducibility, 25 images were randomly selected and anterior segment parameters were remeasured by the same observer (B.C.) on 2 separate occasions. The intraobserver reproducibility was assessed with an intraclass correlation coefficient.
Results
This study enrolled a total of 474 white, African, Hispanic, and Chinese patients who met the inclusion criteria and were willing to participate. Among them, 11 patients were excluded due to poor AS OCT imaging quality (evaluated on the basis of corneal reflection, continuity of anterior segment structures, motion artifacts, and indeterminate scleral spurs). The narrow-angle subjects included 61 whites, 41 Chinese, 28 Africans, and 36 Hispanics. The open-angle subjects included 105 whites, 91 Chinese, 62 Africans, and 39 Hispanics. Among the 463 included patients, 398 subjects did not have a diagnosis of glaucoma and 65 subjects had a diagnosis of glaucoma. Table 1 summarizes the comparisons of anterior chamber area, anterior chamber volume, anterior chamber width, lens vault, iris thickness measured at 750 μm from the scleral spur, iris area, age, sex, pupil diameter, and spherical equivalent between ethnic groups.
| Ethnicity | P Value | ||||
|---|---|---|---|---|---|
| White | Chinese | African | Hispanic | ||
| No. patients (total) | 166 | 132 | 90 | 75 | .069 a |
| Narrow | 61 | 41 | 28 | 36 | |
| Open | 105 | 91 | 62 | 39 | |
| Age (total) (y) | 66.3 ± 13.0 | 64.6 ± 16.2 | 62.7 ± 13.0 | 67.1 ± 13.2 | .146 b |
| Narrow (y) | 68.3 ± 12.6 | 70.4 ± 14.9 | 64.9 ± 9.8 | 66.7 ± 13.0 | .339 b |
| Open (y) | 65.1 ± 13.1 | 62.0 ± 16.1 | 61.7 ± 14.1 | 67.4 ± 13.6 | .108 b |
| Sex (total) (% female) | 53.61% | 57.58% | 64.44% | 65.33% | .218 a |
| Narrow (% female) | 63.93% | 70.73% | 78.57% | 83.33% | |
| Open (% female) | 47.62% | 51.65% | 58.06% | 48.72% | |
| SE (total) (diopters) | −0.4 ± 2.9 | −2.0 ± 4.0 | −0.1 ± 2.1 | 0.0 ± 3.0 | <.0001 b |
| Narrow (diopters) | 1.0 ± 2.2 | 0.8 ± 3.3 | −0.2 ± 1.6 | 0.9 ± 1.9 | .208 b |
| Open (diopters) | −1.3 ± 3.0 | −3.1 ± 3.7 | −0.1 ± 2.4 | −1.0 ± 3.6 | <.0001 b |
| PD (total) (mm) | 3.9 ± 1.3 | 4.1 ± 1.3 | 3.9 ± 1.0 | 4.0 ± 0.9 | .421 b |
| Narrow (mm) | 3.7 ± 1.4 | 3.5 ± 1.5 | 3.8 ± 1.0 | 4.2 ± 0.7 | .164 b |
| Open (mm) | 4.0 ± 1.3 | 4.4 ± 1.1 | 4.0 ± 0.9 | 3.9 ± 1.1 | .064 b |
| ACA (total) (mm 2 ) | 21.1 ± 4.1 | 20.4 ± 4.3 | 21.2 ± 4.1 | 19.3 ± 3.7 | .009 b |
| Narrow (mm 2 ) | 18.3 ± 2.9 | 17.1 ± 2.3 | 18.2 ± 2.4 | 17.0 ± 2.2 | .032 b |
| Open (mm 2 ) | 22.7 ± 3.9 | 21.9 ± 4.1 | 22.6 ± 4.0 | 21.4 ± 3.5 | .279 b |
| ACV (total) (mm 3 ) | 147.2 ± 36.9 | 137.4 ± 35.6 | 146.0 ± 35.3 | 129.7 ± 32.0 | .001 b |
| Narrow (mm 3 ) | 123.0 ± 25.5 | 110.6 ± 19.2 | 120.2 ± 20.4 | 110.8 ± 18.9 | .010 b |
| Open (mm 3 ) | 161.3 ± 35.3 | 149.4 ± 34.8 | 157.6 ± 34.5 | 147.1 ± 31.9 | .044 b |
| ACW (total) (mm) | 12.0 ± 0.5 | 11.7 ± 0.4 | 11.9 ± 0.4 | 11.7 ± 0.5 | <.0001 b |
| Narrow (mm) | 12.0 ± 0.5 | 11.5 ± 0.4 | 11.8 ± 0.4 | 11.7 ± 0.4 | <.0001 b |
| Open (mm) | 12.1 ± 0.5 | 11.7 ± 0.4 | 12.0 ± 0.4 | 11.8 ± 0.5 | <.0001 b |
| LV (total) (mm) | 0.54 ± 0.31 | 0.41 ± 0.35 | 0.36 ± 0.30 | 0.50 ± 0.31 | <.0001 b |
| Narrow (mm) | 0.76 ± 0.23 | 0.68 ± 0.22 | 0.63 ± 0.21 | 0.69 ± 0.21 | .043 b |
| Open (mm) | 0.41 ± 0.28 | 0.29 ± 0.33 | 0.24 ± 0.26 | 0.33 ± 0.28 | .002 b |
| IT750 (total) (mm) | 0.43 ± 0.08 | 0.47 ± 0.08 | 0.46 ± 0.09 | 0.46 ± 0.08 | .008 b |
| Narrow (mm) | 0.43 ± 0.07 | 0.48 ± 0.10 | 0.49 ± 0.09 | 0.47 ± 0.09 | .015 b |
| Open (mm) | 0.43 ± 0.08 | 0.46 ± 0.07 | 0.44 ± 0.09 | 0.44 ± 0.06 | .017 b |
| IArea (total) (mm 2 ) | 1.53 ± 0.24 | 1.59 ± 0.23 | 1.66 ± 0.26 | 1.61 ± 0.29 | <.0001 b |
| Narrow (mm 2 ) | 1.58 ± 0.25 | 1.64 ± 0.25 | 1.71 ± 0.18 | 1.61 ± 0.26 | .114 b |
| Open (mm 2 ) | 1.50 ± 0.23 | 1.57 ± 0.23 | 1.64 ± 0.28 | 1.61 ± 0.32 | .003 b |
| CCT (total) (μm) | 559 ± 33 | 552 ± 43 | 538 ± 36 | 555 ± 37 | <.0001 b |
| Narrow (μm) | 562 ± 33 | 555 ± 52 | 540 ± 36 | 556 ± 30 | .106 b |
| Open (μm) | 557 ± 34 | 551 ± 38 | 537 ± 38 | 554 ± 36 | .008 b |
| IOP (total) (mm Hg) | 16.3 ± 3.7 | 16.1 ± 3.0 | 16.7 ± 3.7 | 17.2 ± 4.7 | .222 b |
| Narrow (mm Hg) | 16.4 ± 3.7 | 16.5 ± 3.7 | 17.2 ± 3.1 | 17.5 ± 5.6 | .529 b |
| Open (mm Hg) | 16.2 ± 3.8 | 16.0 ± 2.7 | 16.5 ± 4.0 | 17.3 ± 3.4 | .367 b |
b P values by 1-way analysis of variance with Tukey post hoc test.
In the narrow-angle group, white, Chinese, African, and Hispanic subjects significantly differed in anterior chamber area, anterior chamber volume, anterior chamber width, lens vault, and iris thickness measured at 750 μm from the scleral spur (all P < .05). In the open-angle group, white, Chinese, African, and Hispanic subjects significantly differed in anterior chamber volume, anterior chamber width, lens vault, iris thickness measured at 750 μm from the scleral spur, and iris area (all P < .05). Merging both narrow-angle and open-angle groups together showed significant difference in anterior chamber area, anterior chamber volume, anterior chamber width, lens vault, iris thickness measured at 750 μm from the scleral spur, and iris area among white, Chinese, African, and Hispanic subjects (all P < .05).
Table 2 lists the comparisons of anterior chamber area, anterior chamber volume, anterior chamber width, lens vault, iris thickness measured at 750 μm from the scleral spur, iris area, age, sex, pupil diameter, and spherical equivalent between narrow-angle and open-angle subjects within each ethnic group. For the white group, significant differences were observed in anterior chamber area, anterior chamber volume, and lens vault between narrow-angle and open-angle subjects (all P < .05). For the Chinese group, significant differences were observed in pupil diameter, anterior chamber area, anterior chamber volume, anterior chamber width, and lens vault between narrow-angle and open-angle subjects (all P < .05). For the African group, significant differences were observed in anterior chamber area, anterior chamber volume, anterior chamber width, lens vault, and iris thickness measured at 750 μm from the scleral spur between narrow-angle and open-angle subjects (all P < .05). For the Hispanic group, significant differences were observed in anterior chamber area, anterior chamber volume, lens vault, and iris thickness measured at 750 μm from the scleral spur between narrow-angle and open-angle subjects (all P < .05).
| Ethnicity | Narrow Angle | Open Angle | P Value | |
|---|---|---|---|---|
| No. patients | White | 61 | 105 | |
| Chinese | 41 | 91 | ||
| African | 28 | 62 | ||
| Hispanic | 36 | 39 | ||
| Age (y) | White | 68.3 ± 12.6 | 65.1 ± 13.1 | .128 b |
| Chinese | 70.4 ± 14.9 | 62.0 ± 16.1 | .004 b | |
| African | 64.9 ± 9.8 | 61.7 ± 14.1 | .216 b | |
| Hispanic | 66.7 ± 13.0 | 67.4 ± 13.6 | .822 b | |
| Sex (% female) | White | 63.93% | 47.62% | .042 a |
| Chinese | 70.73% | 51.65% | .040 a | |
| African | 78.57% | 58.06% | .059 a | |
| Hispanic | 83.33% | 48.72% | .001 a | |
| SE (diopters) | White | 1.0 ± 2.2 | −1.3 ± 3.0 | <.0001 b |
| Chinese | 0.8 ± 3.3 | −3.1 ± 3.7 | <.0001 b | |
| African | −0.2 ± 1.6 | −0.1 ± 2.4 | .951 b | |
| Hispanic | 0.9 ± 1.9 | −1.0 ± 3.6 | .013 b | |
| PD (mm) | White | 3.7 ± 1.4 | 4.0 ± 1.3 | .096 b |
| Chinese | 3.5 ± 1.5 | 4.4 ± 1.1 | .002 b | |
| African | 3.8 ± 1.0 | 4.0 ± 0.9 | .240 b | |
| Hispanic | 4.2 ± 0.7 | 3.9 ± 1.1 | .201 b | |
| ACA (mm 2 ) | White | 18.3 ± 2.9 | 22.7 ± 3.9 | <.0001 b |
| Chinese | 17.1 ± 2.3 | 21.9 ± 4.1 | <.0001 b | |
| African | 18.2 ± 2.4 | 22.6 ± 4.0 | <.0001 b | |
| Hispanic | 17.0 ± 2.2 | 21.4 ± 3.5 | <.0001 b | |
| ACV (mm 3 ) | White | 123.0 ± 25.5 | 161.3 ± 35.3 | <.0001 b |
| Chinese | 110.6 ± 19.2 | 149.4 ± 34.8 | <.0001 b | |
| African | 120.2 ± 20.4 | 157.6 ± 34.5 | <.0001 b | |
| Hispanic | 110.8 ± 18.9 | 147.1 ± 31.9 | <.0001 b | |
| ACW (mm) | White | 12.0 ± 0.5 | 12.1 ± 0.5 | .166 b |
| Chinese | 11.5 ± 0.4 | 11.7 ± 0.4 | .011 b | |
| African | 11.8 ± 0.4 | 12.0 ± 0.4 | .020 b | |
| Hispanic | 11.7 ± 0.4 | 11.8 ± 0.5 | .657 b | |
| LV (mm) | White | 0.76 ± 0.23 | 0.41 ± 0.28 | <.0001 b |
| Chinese | 0.68 ± 0.22 | 0.29 ± 0.33 | <.0001 b | |
| African | 0.63 ± 0.21 | 0.24 ± 0.26 | <.0001 b | |
| Hispanic | 0.69 ± 0.21 | 0.33 ± 0.28 | <.0001 b | |
| IT750 (mm) | White | 0.43 ± 0.07 | 0.43 ± 0.08 | .532 b |
| Chinese | 0.48 ± 0.10 | 0.46 ± 0.07 | .372 b | |
| African | 0.49 ± 0.09 | 0.44 ± 0.09 | .022 b | |
| Hispanic | 0.47 ± 0.09 | 0.44 ± 0.06 | .075 b | |
| IArea (mm 2 ) | White | 1.58 ± 0.25 | 1.50 ± 0.23 | .051 b |
| Chinese | 1.64 ± 0.25 | 1.57 ± 0.23 | .137 b | |
| African | 1.71 ± 0.18 | 1.64 ± 0.28 | .148 b | |
| Hispanic | 1.61 ± 0.26 | 1.61 ± 0.32 | .999 b | |
| CCT (μm) | White | 562 ± 33 | 557 ± 34 | .318 b |
| Chinese | 555 ± 52 | 551 ± 38 | .678 b | |
| African | 540 ± 36 | 537 ± 38 | .696 b | |
| Hispanic | 556 ± 30 | 554 ± 36 | .760 b | |
| IOP (mm Hg) | White | 16.4 ± 3.7 | 16.2 ± 3.8 | .753 b |
| Chinese | 16.5 ± 3.7 | 16.0 ± 2.7 | .392 b | |
| African | 17.2 ± 3.1 | 16.5 ± 4.0 | .421 b | |
| Hispanic | 17.5 ± 5.6 | 17.3 ± 3.4 | .840 b |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


