An antitussive agent should reduce the amount of coughing experienced by the patient sufficiently for the patient to appreciate an improvement in cough severity and regard the improvement as sufficient to outweigh any adverse effects or risks associated with the treatment. In recent years the development of objective cough counting devices and cough-specific quality of life tools have vastly improved our ability to appropriately assess the effectiveness of anti-tussive agents and hopefully will lead to the development of safe and effective treatments in the future. This article summarizes current knowledge of methodologies available for assessing cough therapies, the patient groups to study, and the design of clinical trials.
Cough consistently is reported to be the most common symptom for which patients seek medical advice and it has substantial impacts on quality of life for sufferers. As a consequence, cough represents a significant financial burden; for example, in the United Kingdom, over £100 million/year is spent on over-the-counter antitussives (of questionable efficacy), and the cost to the national economy is estimated at £1 billion annually due to absenteeism from work, reduced productivity, physician consultations, and prescription costs. Despite these facts, safe, effective, and acceptable antitussive agents are lacking. Although this may result partly from poor research investment in understanding of the mechanisms underlying cough and hence the identification of novel treatment targets, the lack of well-validated tools for the accurate measurement of cough in clinical trials also may have impeded progress.
The aim of any effective ant-tussive agent should be to reduce the amount of coughing experienced by the patient sufficiently for the patient to appreciate an improvement in cough severity, and regard the magnitude of the improvement as sufficient to outweigh any adverse effects or risks associated with the treatment. A recent focus group study provided some useful insights into how patients with chronic cough perceive the severity of this symptom. The study concluded that the three main dimensions of cough severity were: frequency of coughing, intensity or physical discomfort associated with coughing, and disruption caused by coughing ( Fig. 1 ).
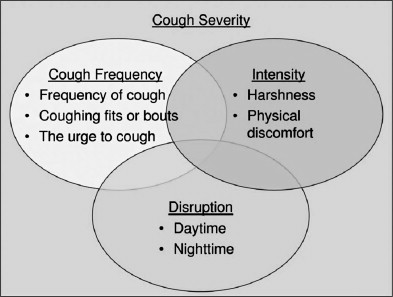
The most sensitive tools for capturing the efficacy of therapies for cough are likely to be those that are able to encapsulate these aspects of cough. In recent years, considerable progress has been made in the understanding of how best to measure cough, including the development of novel tools for the objective assessment of cough frequency and the assessment of the disruption and physical discomfort caused by coughing using cough-specific quality-of-life instruments. This article summarizes the current knowledge about methodologies for assessing cough therapies, the patient groups to study, and the design of clinical trials.
Subjective assessments of cough
In clinical practice and also in clinical trials, one of the quickest and easiest methods for documenting cough severity is to use either a numerical scoring system or visual analog scale.
Numerical Scoring Systems
Various numerical scoring systems have been used to assess the severity of cough and treatment responses. In their simplest forms, patients merely are asked to score their cough severity from 0 to 10 or on Likert scales separately describing increasing frequency or severity. For assessing cough in children, scales for the parents’ observations are needed in addition to those for the child. Other systems have used separate scales to describe coughing during the day and night, such as that used by Hsu and colleagues ( Table 1 ) . This scale uses descriptors of cough frequency for scores from 0 to 2 and then supplements these with description of disruption for scores from 3 to 5, which may be confusing for patients, as infrequent coughing may still be very disruptive.
| Score | Day | Night |
|---|---|---|
| 0 | No cough during the day | No cough during the night |
| 1 | Cough for one short period | Cough on waking only |
| 2 | Cough for more than two short periods | Wake once or early because of cough |
| 3 | Frequent coughing that did not interfere with usual daytime activities | Frequent waking because of cough |
| 4 | Frequent coughing that did interfere with usual daytime activities | Frequent cough most of the night |
| 5 | Distressing cough most of the day | Distressing cough most of the night |
Visual Analog Scales
Visual analog scales (VAS) have been used widely for assessingmany symptoms, but particularly pain. VAS for cough assessment consists of the usual 100 mm scale often marked at the extremes from “no cough” to “very severe” or “worst cough”. Some patient instruction may be required to ensure the scale is used correctly. The author has found cough VAS to correlate moderately with objective cough frequency ( Fig. 2 ) .
There are several limitations to subjective cough assessments that must be appreciated. First, the subject has to recall the severity of his or her cough over a period of time, for example scoring their cough severity on waking for the previous night or even estimating cough severity over periods of up to 2 weeks. Cough events are episodic, and some subjects may have difficulty remembering their symptoms, while others may be very vigilant and score more accurately. Recall bias also may prove a problem when subjects rate the change in cough symptoms over time. Global ratings of change scales are in common use, but rely on subjects comparing their current state to their recollection of a previous state. A recent study has demonstrated that such scale ratings are correlated strongly with the subject’s present state, rather than the change in state. The section on cough quality-of-life measures discusses this further. Other sources of variability in such measures include the influences of the patient’s mood, his or her expectations if an intervention is involved, and also the effect of physical complications of coughing. Patients who experience complications such as cough syncope and incontinence are likely to score cough highly on any scale even if the episodes of coughing are few.
Although the previously mentioned factors limit the accuracy of subjective scores when compared with more objective cough measures, they are nonetheless important in their own right, as they do accurately reflect a patient’s perception of the severity of his or her cough. It remains to be seen whether better targeting subjective assessments to address the different aspects of cough severity as suggested by Vernon and colleagues may make these measures more sensitive to change with interventions for cough.
Cough reflex sensitivity testing
The inhalation of irritant substances (capsaicin, citric acid, distilled water) in increasing concentrations can be used as a measure of the sensitivity of a subject’s cough reflex. Capsaicin is the most commonly used agent and has been shown to be safe, and it has good long- and short-term reproducibility. Additionally, studies have used these challenges to demonstrate the effect of several drugs on cough reflex sensitivity. Although in the past variability in challenge methodologies made study results difficult to compare, the recent European Respiratory Society (ERS) guidelines have aimed to standardize the equipment and challenge regimens used.
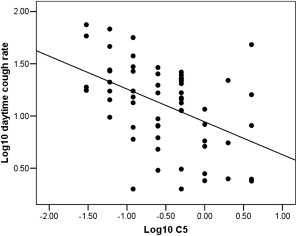
The sensitivity of the cough reflex is clearly mechanistically interesting in the study of cough. For example, cough thresholds are lower in females compared with males, and citric acid and capsaicin thresholds moderately correlate with one another and, therefore, probably represent subtly different aspects of the cough reflex. There is sizeable overlap in cough threshold measurements between healthy volunteers and chronic cough patients, however, perhaps suggesting that these measures largely represent the airway protective reflex common to both groups, rather than the hypersensitivity that leads to profound coughing in chronic cough. This may explain why it has been found that cough reflex sensitivity correlates weakly to moderately with spontaneous cough frequency in chronic cough ( Fig. 3 ), asthma, and chronic obstructive pulmonary disease (COPD) and is, therefore, a poor surrogate for cough counting.
Cough reflex sensitivity testing
The inhalation of irritant substances (capsaicin, citric acid, distilled water) in increasing concentrations can be used as a measure of the sensitivity of a subject’s cough reflex. Capsaicin is the most commonly used agent and has been shown to be safe, and it has good long- and short-term reproducibility. Additionally, studies have used these challenges to demonstrate the effect of several drugs on cough reflex sensitivity. Although in the past variability in challenge methodologies made study results difficult to compare, the recent European Respiratory Society (ERS) guidelines have aimed to standardize the equipment and challenge regimens used.
The sensitivity of the cough reflex is clearly mechanistically interesting in the study of cough. For example, cough thresholds are lower in females compared with males, and citric acid and capsaicin thresholds moderately correlate with one another and, therefore, probably represent subtly different aspects of the cough reflex. There is sizeable overlap in cough threshold measurements between healthy volunteers and chronic cough patients, however, perhaps suggesting that these measures largely represent the airway protective reflex common to both groups, rather than the hypersensitivity that leads to profound coughing in chronic cough. This may explain why it has been found that cough reflex sensitivity correlates weakly to moderately with spontaneous cough frequency in chronic cough ( Fig. 3 ), asthma, and chronic obstructive pulmonary disease (COPD) and is, therefore, a poor surrogate for cough counting.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


