Purpose
To report the repeatability of a digital head-posture measuring system when used to record anomalous head postures in children.
Design
Prospective study and clinical laboratory investigation.
Methods
Using a digital head-posture measuring system, we measured 36 different anomalous head postures in 27 children with infantile nystagmus syndrome. Repeatability values and 95% limits of repeatability of measurements were generated for anomalous head postures.
Results
Among the 27 children, 3 had 2 head postures (right and left head turns) in 2 different directions; 6 had 2-dimensional head postures that were considered 2 different head postures; and 18 had a 1-dimensional head posture. There were 5 chin-up or chin-down postures, 23 head-turn postures, and 8 head-tilt postures in a total of 36 anomalous head postures. The repeatability value for all anomalous head postures was less than 10 degrees. Ninety-five percent limits of repeatability yielded ranges of less than 10 degrees for all anomalous head postures.
Conclusions
The digital head-posture measuring system is a valid and reliable device for measuring 3-dimensional head postures in children with nystagmus.
Anomalous head posture or ocular torticollis is a common clinical symptom in the pediatric population. It has been found that up to 62% of children with nystagmus have anomalous head postures. There is evidence that early corrective surgery for children with ocular torticollis improves visual function and may prevent musculoskeletal problems resulting from uncorrected ocular torticollis. Thus, an effective technique for accurate measurement of ocular torticollis in children is valuable to assist with evaluation and surgical planning. We have developed a digital head-posture measuring system and have shown it to be sufficiently accurate and to yield repeatable outputs from testing a manually positioned artificial head and cooperative adult subjects. This study examined the repeatability of measurements with the digital head posture system when used with children with ocular torticollis.
Methods
Patient Profile
Twenty-seven children with abnormal head posture and nystagmus participated in the investigation ( Table ). Our inclusion criteria involved an age range of patients of either sex from 6 months to 13 years. Patients who fell out of the desired age range were excluded from this study. The mean age for the children was 6.2 years (6 females and 21 males). The protocol and testing were approved by the Institutional Review Board of The University of Pittsburgh and conformed to the requirements of the United States Health Insurance Portability and Accountability Act. All procedures observed the Declaration of Helsinki, and informed consent was obtained from all subjects’ parent or legal guardians.
| Subject No. | Major Head Posture | Mean (degrees) |
|---|---|---|
| 1 | Chin up + left head tilt | 11.37 + −14.53 |
| 2 | Right head turn | 40.57 |
| 3 | Right/left head turn | 23.45/−34.02 |
| 4 | Right head turn | 20.64 |
| 5 | Left head tilt | −19.92 |
| 6 | Left head turn | −16.33 |
| 7 | Right head turn + right head tilt | 16.11 + 23.55 |
| 8 | Left head turn | −38.44 |
| 9 | Right/left head turn | 26.13/−22.77 |
| 10 | Left head turn | −45.90 |
| 11 | Right head turn | 24.25 |
| 12 | Right/left head turn | 11.41/−18.64 |
| 13 | Chin down + right head turn | −15.45 + 34.12 |
| 14 | Right head turn | 24.73 |
| 15 | Chin up + left head tilt | 14.04 + −22.12 |
| 16 | Left head turn | −23.89 |
| 17 | Chin down | −16.37 |
| 18 | Left head tilt | −15.07 |
| 19 | Left head turn | −23.87 |
| 20 | Left head tilt | −20.67 |
| 21 | Left head tilt | −12.58 |
| 22 | Chin down + right head turn | −19.68 + 19.71 |
| 23 | Left head turn + left head tilt | −28.02 + −13.32 |
| 24 | Left head turn | −34.60 |
| 25 | Left head turn | −17.05 |
| 26 | Left head turn | −25.13 |
| 27 | Left head turn | −16.23 |
Device
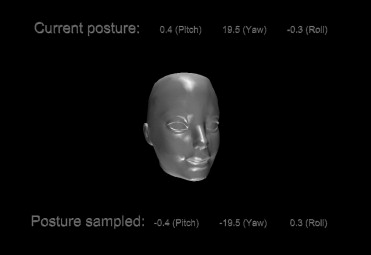
Detailed information regarding the digital head-posture measuring system has been reported and is available in a previously published article. Herein, we briefly describe the digital head-posture measuring system. The digital head-posture measuring system consists of a motion tracker mounted on an adjustable headset, a controller personal computer, and custom software for data recording and visualization. The adjustable headset was modified from prior studies. The plastic headset was replaced by 2 Velcro strips (Velcro Brand Fasteners, Clifton, New Jersey, USA), allowing for improved child comfort and ease of adjustment ( Figure 1 ). The motion tracker is commercially available and uses hybrid techniques, including a magnetometer, accelerometer, and gyroscope made by InterSense (Model 100-ITRAX-0002; InterSense Inc., Billerica, Massachusetts, USA). The software interface was written in C++. The digital head-posture measuring system continuously measures a patient’s head posture at a rate of 20 Hz and presents a real-time animation of a head movement on a liquid crystal display along with numerical readings in 3 dimensions ( Figure 2 ). It records and saves the data into a .txt file for off-line analysis. The saved data include the initial head position, ending head position, and the difference between the 2 positions (head posture in degrees). The manufacturer claims that the tracker works with a full 3600-degree range with angular accuracies of 0.25 degree for chin-up or chin-down and head-tilt measurements and of 0.50 degree for head-turn measurements.

Procedures
We use the terms head turn for rotation around the longitudinal axis (y-axis), chin up or chin down for rotation around the interaural axis (x-axis), and head tilt for rotation around the naso-occipital axis (z-axis) of the head throughout the article. Subjects were seated in an examination chair, and an image was displayed on a screen for the subjects to focus on. Images used were either a letter for older children or a cartoon character for younger children. The distance from the screen to the center of subjects’ head was approximately 1.5 m. As soon as a subject reached his or her null position and maintained a steady head posture, the digital head-posture measuring device was zeroed by pressing the space bar on the keyboard by a computer operator. The subject’s head then was moved manually by the investigator to actual 0 position (0 degrees for chin up or chin down, head turn, and head tilt) by a clinician using a head-rest frame behind the subjects as a reference. As soon as the true 0 position was reached, the enter button was pushed to freeze the instantaneous 3-dimensional angles for the subject’s abnormal head posture. The clinician did not obtain any instantaneous results. A total of 5 measurements were obtained for each head posture.
Data Analysis
Of the 5 measurements recorded for each head posture, the maximum and minimum values were removed, yielding 3 sets of 3-dimensional data. This was mainly because a large variation of head posture in children frequently was seen, and excluding the maximum and minimum values produced more reliable data for clinical application. The remaining data were analyzed to determine repeatability values, r , for every dimension. The equation for repeatability is shown below :
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


