Purpose
To assess the effect of laser in situ keratomileusis (LASIK) on near visual function in presbyopic patients.
Design
Retrospective cohort study.
Methods
Fifty-three eyes of 40 patients 45 years of age and older who had undergone LASIK for high myopia (−6 diopters [D] and over) were included. The minimal add powers for obtaining the best-corrected near visual acuity (add powers) were measured preoperatively and 3 months postoperatively, and the correlations with the powers corrected by LASIK, corneal higher-order aberrations (HOAs), ocular HOAs, and patient ages were evaluated using univariate analysis. Factors correlated with the changes in add powers were evaluated further by multivariate analysis.
Results
The mean ± standard deviation patient age was 50.0 ± 4.1 years; the power corrected by LASIK was −7.56 ± 1.06 D. The mean add power was 1.80 ± 0.60 D preoperatively, which increased significantly ( P < .001) to 2.18 ± 0.69 D postoperatively. Significant correlations with the increased add powers were detected with age ( P = .01) and the power corrected by LASIK ( P = .04) but not with corneal and ocular HOAs ( P > .05). Multivariate analysis showed that only age was correlated significantly ( P = .01). The percentage of eyes with increased add powers of 0.5 D or more was 60.4%, which was significantly ( P = .02) higher in younger patients.
Conclusions
This study verified the apparent progression of presbyopia after LASIK and the importance of obtaining informed consent from patients, especially those with early presbyopia.
Laser in situ keratomileusis (LASIK) is one of the most common elective ophthalmic surgical procedures performed worldwide ; by 2009, more than 16 million procedures had been performed worldwide. More than 95% of patients have been satisfied with the surgical results, with most patients achieving at least 20/40 uncorrected distance visual acuity and the majority achieving 20/20 uncorrected distance visual acuity. Thus, LASIK provides patients with spectacle independence. However, patients over 45 years still need reading glasses after surgery.
The changes in corneal higher-order aberrations (HOAs) after corneal refractive surgery are believed to cause corneal multifocality and may delay the symptoms of presbyopia by extending the depth of field compared to normal presbyopic patients. However, theoretically the ocular accommodation required to bring near objects into focus must increase after myopic corneal refractive surgery compared with spectacle correction owing to changes in the vertex distance, especially in highly myopic patients, if they used spectacles preoperatively. This increase in accommodation for near vision is not a major concern in young patients. However, it may raise concerns about asthenopia or apparent progression of presbyopia resulting in the need for reading glasses that degrades the quality of life for the patients aged 45 years and over.
The purpose of the current study was to assess the effect of LASIK on near visual function in presbyopic patients by evaluating the changes in the minimal additional power needed to attain the best-corrected near visual acuity (VA).
Methods
This retrospective study included patients who underwent LASIK and completed more than 3 months of follow-up. The study followed the tenets of the Declaration of Helsinki, and the Institutional Review Board for Human Studies of Keio University School of Medicine approved the study. All patients provided informed consent before the examinations and surgery.
Patients
Fifty-three eyes of 40 patients (22 women, 18 men) who underwent LASIK at Minamiaoyama Eye Clinic were included in this study. The mean patient age was 50.0 ± 4.1 years (range, 45–59 years). The inclusion criteria were patient age of 45 years and older, a LASIK correction of −6.0 diopters (D) and over, 20/20 or better postoperative best-corrected VA, and a deviation of the postoperative manifest refraction as spherical equivalent not exceeding ± 0.25 D. We selected the minimal myopic correction of −6.0 D, which covered a sufficient number of patients to study with as large a corrected power as possible. All patients underwent complete preoperative and postoperative assessments and had no pathology or intraoperative or postoperative complications.
Surgeries
All surgeries were performed at the Minamiaoyama Eye Clinic from July 9, 2005 to July 21, 2012. The central corneal thicknesses were measured at the corneal apex preoperatively using the AL-2000 pachymeter (Tomey, Aichi, Japan). The corneal flaps were created using a MK-2000L microkeratome (Nidek Co Ltd, Aichi, Japan) or the Intralase FS60 or Intralase iFS femtosecond laser (Abbott Medical Optics Inc, Santa Ana, California, USA). Laser ablation was performed with a 4.5-mm optical zone and 7.0-mm transition zone with multipoint ablation using the EC-5000 (Nidek Co Ltd) excimer laser with a standard algorithm.
Preoperative and Postoperative Refraction and Visual Acuity
The uncorrected and corrected distance VAs (UDVA and CDVA) and corrected near VA (CNVA) were measured preoperatively and 3 months postoperatively. The distance VA was measured using the SC-2000 visual measurement system. (Nidek Co Ltd). The near VA was measured using a decimal VA chart (Nitten Co Ltd, Aichi, Japan) at 40 cm. The minimal additional power needed to achieve the CNVA was determined as the difference between the dioptric powers of the corrected lens for CDVA and for CNVA (add power).
Wavefront Analysis
Corneal and ocular HOAs and refractive data were recorded preoperatively and 3 months postoperatively using ARK 10000 (Nidek Co, Ltd), which is based on automatic retinoscopy and provides integrated corneal topography and wavefront measurement in one device. Corneal HOAs originate from the anterior cornea. All wavefront aberrations were calculated and plotted with respect to the corneal vertex. The corneal topography was measured using Placido disk technology, and the ocular wavefront was measured using the principle of skiascopic phase difference.
The coefficients of the Zernike polynomials were determined up to the sixth order for the 4-mm optical zones from the wavefront data. The root mean squares (RMSs) of the total HOAs (THOA) from the third- to sixth-order Zernike coefficients were calculated. The RMSs of the third- and fifth-order coefficients were used to represent coma-like aberrations (S3 + S5) and the RMSs of the fourth- and sixth-order coefficients were used to denote spherical-like aberrations (S4 + S6).
Literature Search
We conducted a PubMed literature search that covered the period up to November 2013 using the keywords “presbyopia,” “LASIK,” “refractive surgery,” and “accommodation” to search for similar studies.
Statistical Analysis
The preoperative and postoperative values were compared using the paired t test. For statistical analysis of the correlation between factors, Pearson correlation analysis was performed, and stepwise multiple linear regression analysis was performed subsequently. The linear association between age and the rate of significant postoperative increases in add power was evaluated using the Cochran-Armitage trend test that calculated the exact P value.
Statistical analyses were performed using SPSS version 20 for Windows software (IBM Corp, Armonk, New York, USA). The Cochran-Armitage trend test was calculated using SAS version 9.2 (SAS Institute, Cary, North Carolina, USA). The values are expressed as the means ± standard deviations; a probability of less than 5% ( P < .05) was considered statistically significant.
Results
Visual and Refractive Data and Surgical Outcomes
Table 1 shows the preoperative and postoperative refraction and VAs. The add power to achieve the CNVA significantly increased by 0.38 ± 0.60 D ( P < .001) postoperatively.
| Parameters | Mean ± SD (Range) | P Value | |
|---|---|---|---|
| Preoperative | Postoperative | ||
| Subjective refraction (SE) (D) | −7.72 ± 1.05 (−10.88 to −6.00) | 0.00 ± 0.03 (−0.13 to 0.13) | <.001 a |
| Power corrected by LASIK (D) | −7.56 ± 1.06 (−10.75 to −6.00) | ||
| UDVA (logMAR) | 1.34 ± 0.18 | −0.11 ± 0.08 | <.001 a |
| Snellen equivalent | 20/383 | 20/14 | |
| CDVA (logMAR) | −0.10 ± 0.06 | −0.14 ± 0.06 | .75 |
| Snellen equivalent | 20/15 | 20/14 | |
| CNVA (logMAR) | 0.00 ± 0.01 | 0.00 ± 0.02 | .32 |
| Snellen equivalent | 20/20 | 20/20 | |
| Add power b (D) | 1.80 ± 0.60 | 2.18 ± 0.69 | <.001 a |
a Significant correlation ( P < .05).
Wavefront Analysis
Table 2 shows the changes in the wavefront analysis for a 4-mm pupil. The corneal aberrations and ocular coma-like aberration increased significantly postoperatively.
| Parameters | Mean ± SD (Range) | P Value | |
|---|---|---|---|
| Preoperative | Postoperative | ||
| Corneal | |||
| Spherical-like aberrations (S 4 + S 6 ) (μm) | 0.08 ± 0.03 (0.04 to 0.16) | 0.12 ± 0.03 (0.06 to 0.21) | <.001 a |
| Coma-like aberrations (S 3 + S 5 ) (μm) | 0.10 ± 0.04 (0.04 to 0.23) | 0.17 ± 0.05 (0.06 to 0.31) | <.001 a |
| Ocular | |||
| Spherical-like aberrations (S 4 + S 6 ) (μm) | 0.07 ± 0.05 (0.03 to 0.35) | 0.09 ± 0.12 (0.02 to 0.89) | .17 |
| Coma-like aberrations (S 3 + S 5 ) (μm) | 0.14 ± 0.08 (0.04 to 0.47) | 0.18 ± 0.07 (0.07 to 0.34) | .03 a |
The power corrected by LASIK was correlated significantly with the postoperative corneal THOA (r = −0.314, P = .03). No correlation was identified between the power corrected by LASIK and the postoperative ocular THOA (r = −0.210, P = .16) ( Table 3 ). The postoperative corneal coma-like aberrations (S 3 + S 5 ) were not significantly correlated with the amounts of correction (r = −0.222, P = .14); however, they were significantly (r = −0.378, P = .01) correlated with the corneal spherical-like aberrations (S 4 + S 6 ). Increases in add power were not correlated significantly ( P > .05) with the corneal and ocular HOAs ( Table 3 ).
| HOA Values (μm) | Correlation Coefficient | |
|---|---|---|
| With Power Corrected by LASIK | With Increase in Add Power | |
| Postoperative value | ||
| Corneal | ||
| Spherical-like aberrations (S 4 + S 6 ) | −0.378 a ( P = .01) | 0.128 ( P = .40) |
| Coma-like aberrations (S 3 + S 5 ) | −0.222 ( P = .14) | 0.039 ( P = .80) |
| Total aberrations (S 3 +S 4 +S 5 +S 6 ) | −0.314 a ( P = .03) | 0.083 ( P = .58) |
| Ocular | ||
| Spherical-like aberrations (S 4 + S 6 ) | −0.038 ( P = .80) | 0.033 ( P = .83) |
| Coma-like aberrations (S 3 + S 5 ) | −0.420 a ( P = .01) | 0.179 ( P = .24) |
| Total aberrations (S 3 +S 4 +S 5 +S 6 ) | −0.210 ( P = .16) | 0.126 ( P = .40) |
| Increment value | ||
| Corneal | ||
| Spherical-like aberrations (S 4 + S 6 ) | −0.179 ( P = .24) | 0.093 ( P = .54) |
| Coma-like aberrations (S 3 + S 5 ) | −0.177 ( P = .24) | 0.099 ( P = .51) |
| Total aberrations (S 3 +S 4 +S 5 +S 6 ) | −0.198 ( P = .19) | 0.120 ( P = .43) |
| Ocular | ||
| Spherical-like aberrations (S 4 + S 6 ) | 0.045 ( P = .77) | 0.095 ( P = .54) |
| Coma-like aberrations (S 3 + S 5 ) | −0.270 ( P = .08) | 0.209 ( P = .17) |
| Total aberrations (S 3 +S 4 +S 5 +S 6 ) | −0.139 ( P = .36) | 0.178 ( P = .24) |
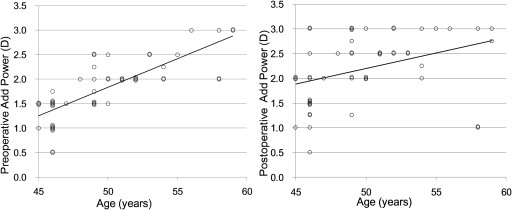
Increases in Add Power After Laser In Situ Keratomileusis
Figure 1 shows the relationship between patient age and the preoperative and the postoperative add powers. The preoperative and postoperative add powers were significantly (r = 0.785, P < .001, and r = 0.374, P = .01, respectively) positively correlated with patient age.