Introduction and Epidemiology
Herpes simplex virus type 1 (HSV-1) constitutes the vast majority of herpetic ocular infections of the anterior segment. Diagnosis is typically made clinically, although serologic and molecular testing is available.
1,2 Humans are the only natural reservoir, and an estimated 50% to 80% of the adult population has antibodies to HSV-1.
3 After primary infection by HSV, which typically manifests with nonspecific upper respiratory symptoms, the virus may achieve latency in the trigeminal ganglion. Any structure in the anterior segment can be involved and the infection presents, sometimes simultaneously, in several major forms: blepharoconjunctivitis, infectious epithelial keratitis, neurotrophic keratopathy, stromal keratitis, endotheliitis, iridocyclitis, and trabeculitis.
There is considerable variation in the literature regarding the incidence, presentation, and recurrences of herpetic keratitis, which may be the result of differing study populations, disease definitions, length of follow-up, and/or other factors. In the United States, estimates from a relatively homogenous white population in the upper Midwest indicated the prevalence to be 149 per 100,000 population, with an incidence of 8.4 per 100,000 personyears.
4 Bilateral involvement is less common, usually associated with atopy or other systemic immunosuppression and, depending on the definition used, can range from 3% to 12%.
3,5 In one study, primary ocular HSV presented as infectious epithelial keratitis in 15% of patients and stromal keratitis in only 2% of patients.
6 Another study found that initial episodes involved the eyelids or conjunctiva in 54% of cases, the superficial cornea in 63%, the deep cornea in 6%, and the uvea in 4%.
4 In susceptible individuals, recurrence of the virus can lead to blinding keratitis or uveitis. In patients who suffered from primary ocular HSV followed up from 2 to 15 years, 32% had recurrences, with 51% of those patients having multiple recurrences,
7 but most of the recurrences did not involve the cornea. Recurrence rates for any form of ocular HSV have been estimated at 9.6% at 1 year, 22.9% to 33% at 2 years, 36% to 40% at 5 years, and 63.2% at 20 years.
4,8,9,10The Herpetic Eye Disease Studies (HEDS) I and II were a set of six trials, supported primarily by the National Eye Institute of the United States National Institutes of Health (NEI/NIH), whose goals were to answer clinical questions about the treatment and recurrence of HSV keratitis and uveitis (see
Tables 4.1,
4.2,
4.3,
4.4,
4.5 and
4.6). The studies were well designed and monitored, with intervention by the Data and Safety Monitoring Committee in three of the trials. One systematic review (see
Table 4.7) details the available therapeutic interventions for infectious epithelial keratitis.
11 Taken together, the HEDS and systematic review provide valuable insight into the clinical management of HSV keratitis (see
Table 4.8).
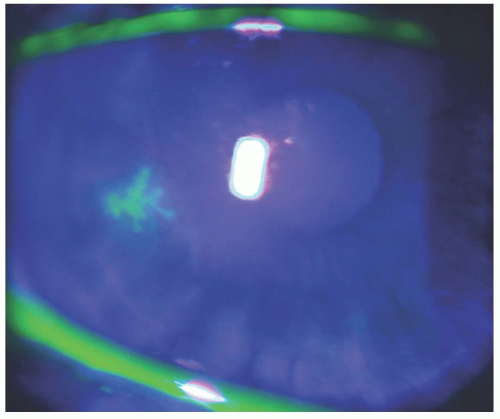
Infectious Epithelial Keratitis. The initial phase of HSV-1 epithelial disease presents as minute corneal vesicles that stain negatively with fluorescein dye.
1 This may progress to a dendritic keratitis (see
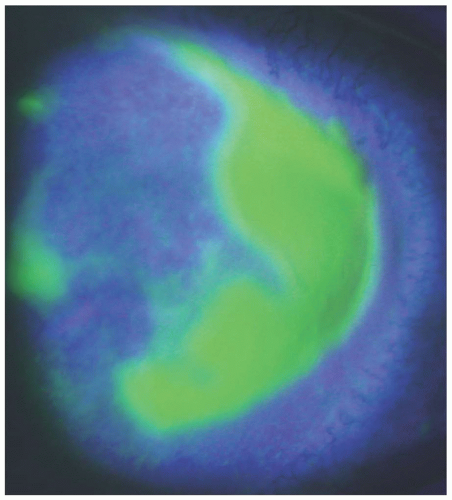
Fig. 4.1), a geographic
keratitis (see
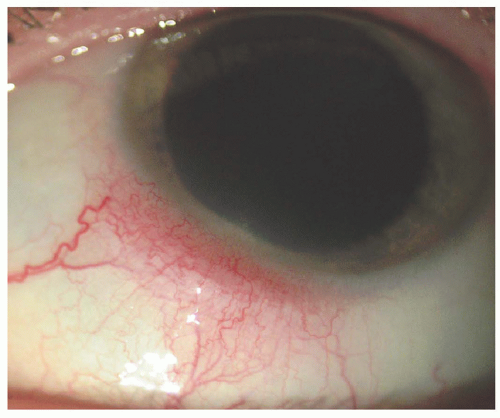
Fig. 4.2), or a marginal keratitis with limbitis (see
Fig. 4.3). Although these conditions may resolve spontaneously without therapy, antiviral therapy is generally indicated to accelerate resolution. Rates of healing appear equivalent between acyclovir (ACV), trifluridine, and vidarabine.
11 Debridement alone does not appear effective, but in conjunction with antiviral therapy may speed epithelial healing rates.
11 The addition of a 3-week course of oral ACV to trifluridine was found by the HEDS epithelial keratitis trial (EKT) (
Table 4.4) to provide no additional benefit in epithelial healing rates or prevention of stromal keratitis or iridocyclitis.
12
Topical ganciclovir ophthalmic ointment has been demonstrated to have noninferiority compared with topical trifluridine,
13,14,15 with some studies suggesting a trend to better tolerance and faster epithelial healing when compared with topical trifluridine.
14,16 In spite of the injury invoked by episodes of disease activity, most patients affected will have a final visual outcome that remains acceptable.
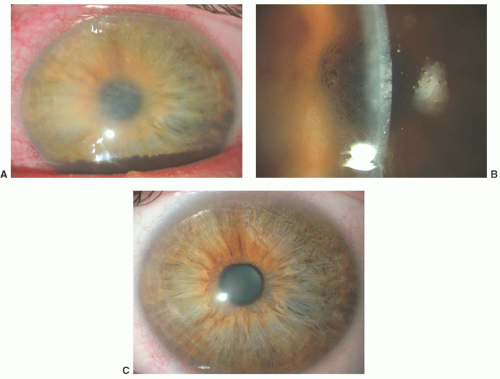
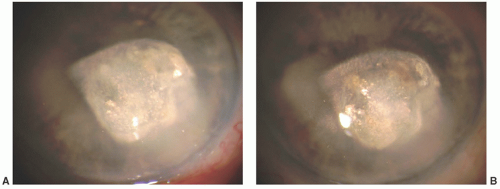
4Stromal Keratitis and Endotheliitis Manifestations of HSV-1 stromal disease include immune stromal keratitis (see
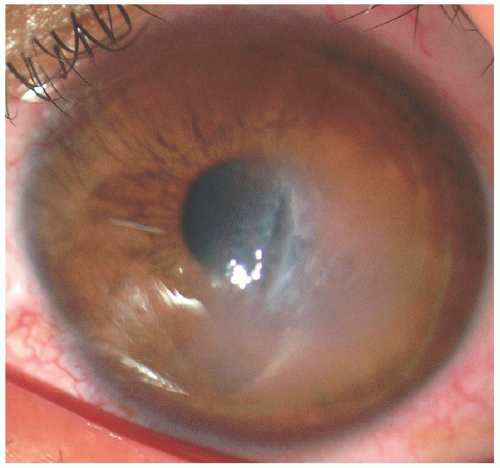
Fig. 4.4) and necrotizing keratitis. While the latter is potentially devastating in the acute period, immune stromal keratitis leads to corneal
blindness through a chronic relapsing and remitting course (see
Fig. 4.5). Endotheliitis can accompany stromal keratitis and manifests with microcystic corneal edema and keratic precipitates (
Fig. 4.4). The value of corticosteroid treatment of stromal keratitis was assessed in the HEDS stromal keratitis, not on the steroid (SKN) trial (
Table 4.1).
17 The main conclusion was that a 10-week course of topical corticosteroid treatment contributes to a faster visual recovery, although a delay in therapy does not affect final visual outcome at 6 months. The major question that remains unanswered by this study was whether a 10-week course was sufficient. Half of the patients in the corticosteroid group of the study who “failed treatment” did so in the 6 weeks after discontinuation of the topical steroid. Currently, in clinical practice, topical steroids may be continued for many months, and perhaps indefinitely at low dosages and frequencies, often in conjunction with chronic oral ACV therapy. Although the final visual outcome was not affected by delay in treatment, it should be noted that 76% of the placebo group failed treatment, and 72% of the placebo group that showed visual improvement was eventually treated with topical corticosteroids. In fact, by 16 weeks after randomization, the total duration of topical corticosteroid usage was similar in both the placebo and corticosteroid groups. It is important to note, however, that 22% of patients had resolution of stromal keratitis with only topical antiviral treatment.
Iridocyclitis and Trabeculitis. HSV iridocyclitis and trabeculitis are uncommon conditions. The HEDS iridocyclitis, receiving topical steroid (IRT) trial (
Table 4.3) was stopped because of low recruitment, with only 50 of the planned 104 patients recruited over 4 years.
18 These conditions can occur concomitantly with other forms of HSV infections, as noted in the HEDS-SKN trial in which 34% and 16% of the eyes with stromal keratitis had concomitant iridocyclitis and trabeculitis, respectively. The iridocyclitis can be either granulomatous or nongranulomatous. Intraocular pressure (IOP) increase from trabeculitis, when stromal keratitis or iridocyclitis is present, may easily be misinterpreted as being a steroid-induced glaucoma. In fact, HSV should be included in the differential diagnosis of any iridocyclitis associated with increase in IOP. Owing to its small sample size, the HEDS-IRT trial (
Table 4.3) suffered from low recruitment, between the ACV and placebo groups in the rates of treatment failure in patients treated with corticosteroids and trifluridine. There was a trend, however, toward a reduction of treatment failures in patients treated with oral ACV.
Prevention of Recurrence
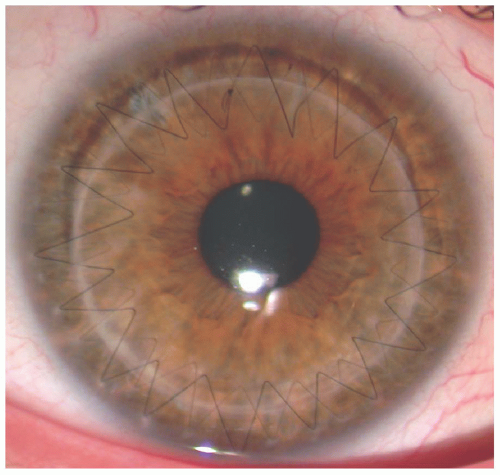
It had been previously demonstrated in a small, prospective randomized series that oral ACV reduced recurrences of HSV keratitis and improved graft survival after penetrating keratoplasty (PKP).
19 The reduction in recurrence rate was confirmed by the HEDS ACV prevention trial (APT) (
Table 4.5) and yielded, perhaps, the most important results from the HEDS. It demonstrated that not only was oral ACV 400 mg, taken twice daily, able to reduce the recurrence rate of any form of ocular HSV compared with placebo, it also reduced nonocular recurrences.
20 Given that recurrent stromal keratitis leads to progressive corneal scarring and potential corneal blindness, it was clinically significant that oral ACV reduced stromal recurrence by 50% among patients who had stromal keratitis in the previous year.
Lingering questions remain, such as whether a lower dosage would have been equally efficacious or whether a higher dosage would be more successful in preventing recurrences.
21 Likewise, the end point for treatment with oral ACV remains unclear, as recrudescence occurs upon discontinuation of the medication.
22 As the HEDS-EKT demonstrated a low risk of developing stromal keratitis or iridocyclitis after a primary episode of epithelial keratitis, it does not seem necessary to begin therapy, perhaps lifelong, with oral ACV in these patients. Additionally, ACV prophylaxis may be relatively cost-ineffective and a theoretic model for treatment, targeting patients with stromal keratitis, found no increase in cost-effectiveness compared with targeting any patient with a history of HSV ocular disease.
23 Long-term treatment may therefore be best reserved for patients with recurrent disease or
cases in which visual acuity is already threatened or compromised.
Although long-term oral ACV therapy was found helpful in the HEDS-APT, other HEDS trials could not definitely elicit a benefit of high-dose short-term therapy with oral ACV in patients already taking trifluridine 1% drops concomitantly. In the HEDS stromal keratitis, on steroid treatment (SKS) trial (
Table 4.2), no apparent benefit of a 10-week course of oral ACV (400 mg five times daily) was found over placebo.
24 Likewise, the HEDS-IRT and HEDS-EKT (
Tables 4.3 and
4.4, respectively) trials did not find significant advantages in using short-term courses of oral ACV in conjunction with trifluridine. It should also be noted that in the HEDS, some patients had recurrences in spite of treatment with oral ACV and/or topical trifluridine.
Alternative Therapies and Future Directions
Development of better diagnostic and therapeutic options for HSV, and other
herpesviruses, remains essential, given the morbidity of these viruses and the chronic nature of these infections. It is unknown as to how many cases of ocular HSV are undiagnosed or misdiagnosed. Likewise, although oral ACV is assumed to be an effective treatment for most patients, ACV-resistant HSV strains have been found in 7% of immunocompromised individuals.
27 As such, various medical and alternative therapies are under investigation. There is mixed evidence on the usage of oral or topical forms of lysine in the management of herpes labialis.
28,29 A proposed mechanism of action is that high intracellular concentrations of lysine competitively inhibit arginine, which is necessary for HSV reproduction.
30 Currently, there are no available topical ophthalmic preparations of lysine. If there is a beneficial effect from oral lysine supplementation, it will likely need to be administered as a chronic treatment at high dosages (1,000-3,000 mg/day) to help prevent recurrences. There have been some studies that have demonstrated efficacy of topical light-activated rose bengal in the reduction of extracellular herpes viral quantization, but more limited effects on intracellular viral load.
31,32 Considering the relatively innocuous nature of rose bengal, this may be a useful adjunct to current therapies, especially for HSV keratitis unresponsive to standard treatment. Other drugs that inhibit the ability of HSV to enter noninfected cells may offer hope for prevention of disease acquisition.
33Virus-specific Th1 cytokines and active innate immunity can prevent HSV recurrence.
34 This knowledge has been incorporated into vaccine strategies and one vaccine reduced the clinical symptoms of primary HSV-2 infection by over 70%, but only in women who were both HSV-1 and HSV-2 seronegative.
34,35,36 Although there are still no clinical vaccines available for HSV and significant challenges remain, these results suggest the eventual development of more effective options. Through a better understanding of the biology of HSV, either new medications or
vaccines should be able to interfere with the acquisition of the primary infection or recurrence of the infection or possibly eradicate the virus altogether.