Purpose
To assess the role of androgen receptor detection in diagnosing eyelid sebaceous carcinomas and to compare it with that of adipophilin.
Design
Retrospective, clinicopathologic study.
Methods
Ten sebaceous carcinomas (8 invasive, 2 intraepithelial only) were stained immunohistochemically for androgen receptors and were compared with adipophilin staining. Receptor staining also was performed on benign sebaceous tumors (a sebaceoma and an adenoma) and as controls on eyelid basal cell carcinomas, eyelid squamous cell carcinomas, conjunctival squamous dysplasias, and conjunctival melanomas.
Results
All 8 patients with an invasive component of sebaceous carcinoma underwent a biopsy in which the tumor cells showed diffusely positive results for androgen receptors (>20% of cells and usually >40%) and positive results for adipophilin. Eight cases displaying an intraepithelial (or pagetoid) component of spread also showed diffusely positive results for androgen receptors and adipophilin in at least 1 of multiple biopsy samples from each patient. However, in 8 of 21 separate conjunctival biopsy specimens with intraepithelial cytologic atypia, adipophilin results were negative. A sebaceoma and a sebaceous adenoma also showed positive results for both of these biomarkers. Among the controls, squamous carcinomas and melanomas showed negative results for androgen receptors and adipophilin. Basal cell carcinomas displayed focal receptor positivity in fewer than 5% of cells and showed negative results for adipophilin.
Conclusions
Androgen receptors and adipophilin can separate sebaceous tumors immunohistochemically from squamous carcinomas and melanomas, which showed negative results for both, and from basal cell carcinomas, which showed positive receptor results in a distant minority of cells. Regarding intraepithelial (or pagetoid) spread, androgen receptor detection was more sensitive and reliable than adipophilin in highlighting this component of the disease.
Apart from their role in regulating sexual and reproductive functioning, androgen receptors also are present in many tissues and affect important aspects of the body’s nonsexual economy. Dermatopathologists have correlated male pattern baldness with androgen receptors, which have been identified in the pilosebaceous-apocrine unit. Work with androgen receptors has been limited in ophthalmology to elucidating their impact on the regulation of Meibomian gland functioning that assists in maintaining the integrity of the ocular surface. Among tumors, androgen receptor physiology in tumors has been studied most thoroughly in prostatic neoplasms. Only a few nonophthalmic skin tumors have been evaluated immunohistochemically for androgen receptors, such as basal cell carcinomas, trichoblastic lesions, chondroid syringomas, and benign and malignant sebaceous tumors.
Although sebaceous malignancies of the eyelids logically by extrapolation may be expected to have similar immunohistochemical properties to those found elsewhere in the skin, this presumption has not yet been clearly proved scientifically. Indeed, the Meibomian glands are unique in the skin for not being associated with either a strong or vellus hair (only the Zeis glands are attached to the eyelashes). Furthermore, intraepithelial (or pagetoid) spread is seen rarely in nonophthalmic skin examples, which may alter tumor cell biomarker expression and obscure the correct diagnosis. In the current article, we explore the diagnostic value of androgen receptors with respect to benign and malignant ocular adnexal sebaceous tumors and compare the immunostaining results with those obtained with adipophilin. We also investigated whether sebaceous tumors can be distinguished with androgen receptors from other tumors, such as squamous and basal carcinomas and melanomas.
Methods
This retrospective study was conducted under the auspices of the Massachusetts Eye and Ear Infirmary Institutional Review Board (protocol no. 13-056H) and in compliance with the rules and regulations of the Health Insurance Portability and Accountability Act, in adherence to the tenets of the Declaration of Helsinki, and according to all relevant federal and state laws.
Eight of the 10 selected patients had infiltrating eyelid sebaceous cell carcinomas and 8 had a component of intraepithelial spread. Seven cases have been reported previously for adipophilin expression, but not for androgen receptors, and therefore have been included in this study. These cases were acceptable because there was adequate tissue remaining in the paraffin blocks for further immunostaining. Three new patients not previously reported also are included in this series. The glass slides from all of the earlier biopsies were reviewed. For invasive disease, the paraffin block of the most representative section stained with hematoxylin and eosin, mucicarmine and periodic acid Schiff was chosen for additional immunostaining for androgen receptors and adipophilin. A total of 21 separate tissue specimens from all 8 patients manifesting intraepithelial spread were immunostained for androgen receptors and adipophilin to establish their variable rates of expression and their relative values as biomarkers for diagnosis (if discernible).
As controls, an eyelid sebaceoma that has been published, but without androgen receptor testing, and an unreported caruncular sebaceous adenoma with papillary features also were evaluated for comparison. Additionally, 5 eyelid-infiltrating epidermoid (squamous)-cell carcinomas, 5 basal-cell carcinomas, and 5 conjunctival melanomas were investigated for androgen receptors. Seven conjunctival juxtalimbal epidermoid (squamous) dysplasias, including 5 that have been reported previously without investigating androgen receptors, also were used as controls.
Immunohistochemical evaluations were performed on archived formalin-fixed, paraffin-embedded tissue blocks after 5-μm tissue sections were obtained. Infiltrating lesions were judged to have overall positive results for sebaceous carcinoma if androgen receptors and adipophilin (either in its vesicular or granular forms) each were discovered in 5% or more of cells or stated otherwise, the lesions were regarded as having negative results if 95% or more of cells were nonimmunoreactive. All tumors reached the level of positivity. Immunohistochemical stains were processed in the standard manner with appropriate nonophthalmic tissue controls on a Leica Bond III autostainer (Leica Biosystems, Melbourne, Australia) at the Diagnostic Immunopathology Laboratory of the Massachusetts General Hospital (Boston, Massachusetts, USA). The tissue controls validated the quality and specificity of antibody staining. The antibody probes for detecting the following biomarker antigens were used: androgen receptor (mouse monoclonal, clone AR441, 1:50; Dako, Carpinteria, California, USA) detectable in the nucleus; adipophilin (mouse monoclonal, clone AP125, 1:75; Fitzgerald Industries International, Acton, Massachusetts, USA) for cytoplasmic lipid; and microphthalmia-associated transcription factor for the nuclei of melanoma cells (mouse monoclonal, clone D5, ≥ 1:120; Cavendish Scott Ltd, Hertforshire, United Kingdom). For androgen receptors, heat-induced epitope retrieval was carried out before immunohistochemical staining using Bond epitope retrieval solution 2 (ph, 9.0; Leica Biosystems, Newcastle-upon-Tyne, United Kingdom) for 20 minutes. All immunohistochemical stains were developed using the chromogen diaminobenzidine, and tissues were counterstained with hematoxylin. The tissue slides were visualized using routine light microscopy.
Results
Sebaceous Carcinomas
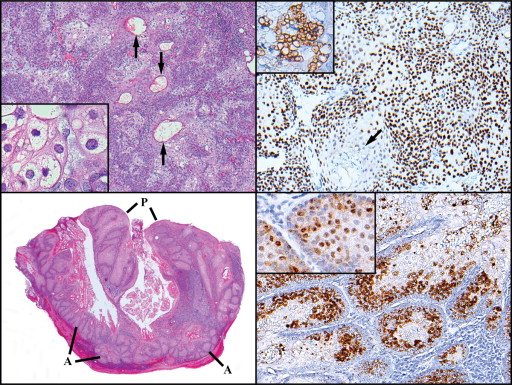
Of the 10 patients in this study with sebaceous carcinoma of the eyelids, 8 were women and 2 were men. Their ages ranged from 44 to 98 years, with a mean of 76 years. The lower eyelids were involved in 6 cases and the upper eyelid in 4 cases. Three patients (30%) experienced recurrences, but there have been no tumor-associated deaths. Six patients (60%) underwent biopsies or excisions that showed evidence of infiltrating sebaceous carcinoma ( Figure 1 , Top left), 2 patients (20%) had infiltrating disease alone, and 2 patients had only intraepithelial disease. Two benign sebaceous lesions also were studied for androgen receptor expression: a caruncular sebaceous adenoma in a 68-year-old woman ( Figure 1 , Top right) and a sebaceoma in a 53-year-old man (this case was published previously without androgen receptor analysis ).
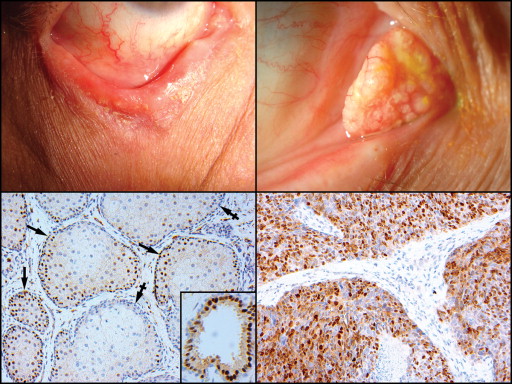
For a background of normal eyelid adnexal glandular immunostaining, 10 normal uninvolved regions of full-thickness eyelid specimens, removed for the treatment of basal cell and epidermoid carcinomas, sebaceous tumors, floppy eyelids, or ectropion or entropion, were evaluated. The epidermis and palpebral conjunctival epithelium showed negative results for androgen receptors and adipophilin. Androgen receptor nuclear positivity was noted among many basal and occasional suprabasal cells in the Meibomian and Zeis glands ( Figure 1 , Bottom right), but not in the nonkeratinizing squamous duct cells ( Figure 1 , Bottom left). The smaller lobules (alveoli) exhibited more positive nuclei centrally than the larger ones. The most intense staining was found in the inner secretory cells of the apocrine glands of Moll ( Figure 1 , Bottom left inset), which was consistently observed in 7 separate specimens. Five accessory lacrimal glands of Wolfring (tarsus) were present in surgical excisions and showed negative results for androgen receptors.
A summary of the main histopathologic diagnostic categories and their immunostaining characteristics is provided in the Table . The 6 cases showing both infiltrating and intraepithelial sebaceous carcinoma displayed vacuolated cells in each component, with oval or round nuclei manifesting a fine stippling of the chromatin and a small punctate nucleolus, as has been reported previously and illustrated in detail. The invasive component in these cases was composed of variably sized lobules without peripheral palisading or clefting. All patients who had infiltrative tumors demonstrated positive nuclear androgen receptor immunoreactivity, usually in 20% to 40% of the constituent cells ( Figure 1 , Bottom right). In 1 patient, however, the first infiltrative lesion showed negative results, but a second recurrent one separated in time showed positive results, probably because of a defect in the testing process or a defective antibody reagent.
| Sebaceous Carcinoma Components and Other Tumors | No. of Patients | No. of Specimens Tested a | No. of Androgen Receptor-Positive Specimens b | No. of Adipophilin-Positive Specimens c |
|---|---|---|---|---|
| Invasive sebaceous carcinoma | 8 | 11 | 10 d | 11 |
| Intraepithelial (pagetoid) sebaceous carcinoma | 8 | 21 | 21 | 13 |
| Sebaceoma | 1 | 1 | 1 | 1 |
| Sebaceous adenoma | 1 | 1 | 1 | 1 |
| Eyelid squamous cell carcinoma | 5 | 10 | 0 | 0 |
| Conjunctival squamous cell dysplasia | 7 | 7 | 1 e | 0 |
| Basal cell carcinoma | 5 | 5 | 5 f | 0 |
| Conjunctival melanoma | 4 | 5 | 0 | 0 |
a Multiple blocks or separate specimens including map biopsies from the same patient (up to 8 in 1 patient) were often sampled.
b Nuclear staining of more than 20% of cells.
d From the same patient, of 2 biopsies separated in time. The first showed negative results (probably because of an artifact of testing) and the second showed positive results.
e Aberrant expression in 1 lesion that was adipophilin negative.
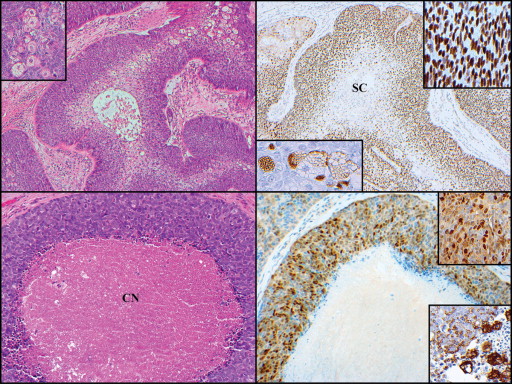
Seven tumors contained units with highly differentiated (fully vacuolated) cells (sebocytes) in the central regions with an outer zone of multilaminar, basaloid germinative cells (seboblasts) ( Figure 2 , Top left). Positive staining results for androgen receptors were discovered only in the outer basaloid region ( Figure 2 , Top right [main panel and inset upper right]); the clear central cells occasionally showed focal immunoreaction for adipophilin ( Figure 2 , Top right [inset bottom left]). Likewise, lobules with central comedonecrosis ( Figure 2 , Bottom left) manifested androgen receptor positivity restricted to the outer rim of encircling viable basaloid cells ( Figure 2 , Bottom right [upper inset]). Adipophilin in this pattern was most pronounced in the transition between the rim of viable basaloid cells and the central necrotic zone ( Figure 2 , Bottom right [lower inset]). There were different patterns and densities of androgen receptor-positive nuclei and cytoplasmic adipophilin positivity from field to field and lesion to lesion.
Intraepithelial disease was observed in 8 of the 10 cases: in 6 it was associated with infiltrative nodules and in 2 it was found without an infiltrative component. The latter may have been present, but was not biopsied or else was present in a biopsy that had been sampled incompletely. The pagetoid pattern was defined as the presence of individual cells or small clusters scattered within a background of normal epithelium. The carcinoma in situ pattern represented a complete replacement of the pre-existent normal epithelium by malignant oval or vaguely spindled cells with variably vacuolated or clear cytoplasm and a nucleus that was approximately one and a half times larger than that of a normal keratinocyte. The epidermis of the skin and the epithelium of the eyelid margin displayed only the pagetoid pattern, whereas the conjunctival epithelium exhibited either a pagetoid pattern or carcinoma-in-situ pattern.
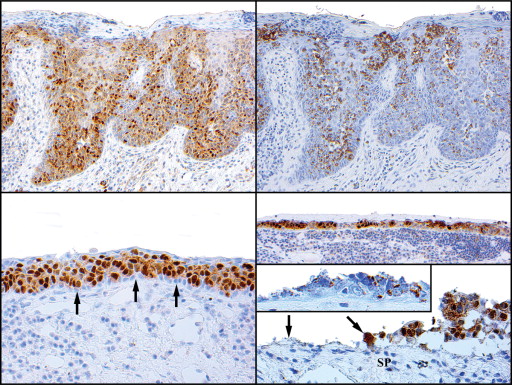
The tumor cells harbored within the epidermis always showed positive androgen receptor results ( Figure 3 , Top left) and usually positive adipophilin results ( Figure 3 , Top right). In the conjunctival epithelium, there was a striking regularity in androgen receptor positivity ( Figure 3 , Bottom left). Adipophilin positivity, however, was more spotty and erratic. A frequently encountered phenomenon was clefting and shedding of neoplastic sebaceous intraepithelial cells ( Figure 3 , Bottom right), beneath which there was an especially dense band of mononuclear inflammatory cells. Androgen receptor positivity was detected in the remaining cells in these zones ( Figure 3 , Bottom right [top and bottom panels]) up to the edge, where denudation of epithelium was complete. Adipophilin typically was identified only weakly or was not present at all in these zones ( Figure 3 , Bottom right [bottom panel inset]). Overall, 8 of 21 biopsies showing intraepithelial spread failed to immunostain for adipophilin, and these were obtained from the conjunctiva, whereas all showed positive androgen receptor results.
Benign Sebaceous Tumors
The sebaceoma displayed small ductular formations with cuticles within cell clusters with epidermoid features. There was a prominent population of small hematoxylinophilic basaloid cells, among which were irregularly distributed, well-differentiated, highly vacuolated sebocytes in the basaloid cells ( Figure 4 , Top left and inset). Androgen receptors were strikingly positive with basaloid cells (seboblasts; Figure 4 , Top right). The sebocytic elements tended to be arranged in small groups and showed negative androgen receptor results, but consistently showed positive adipophilin results ( Figure 4 , Top right inset). The adenoma displayed papillary features with multiple layers of basaloid cells growing on fibrovascular cores. Progressive differentiation was evidenced as the cells proceeded toward the surface ( Figure 4 , Bottom left). At the lateral edges and base of the tumor, there were solid lobular (adenomatous) units. Both adipophilin ( Figure 4 , Bottom right) and androgen receptor ( Figure 4 , Bottom right inset) results were markedly positive.