Anatomy and Physiology
Phyllis Peng
Gady Har-El
Head and neck anatomy is a compact organization of neural, vascular, epithelial, and musculoskeletal elements that functionally integrate to pose a constant challenge to the otolaryngologist.
THE EAR
Anatomy
External Ear
The external ear consists of the auricle and the external auditory canal. Except for the lobule, the entire auricle is composed of elastic cartilage and skin (Fig. 2-1). This skin is thin and densely adherent in the front and more loosely attached behind. The auricle is attached to the head by the external auditory canal and several small muscles innervated by the facial nerve.
External Auditory Canal
The external auditory canal (Fig. 2-2) is cartilaginous in the lateral third (continuous with that of the auricle) and bony in the inner two-thirds. The skin lining the cartilaginous portion contains hair follicles, sebaceous glands, and cerumen glands. Small dehiscences in the anterior portion of this cartilage (fissures of Santorini) provide potential pathways for the spread of tumor and infection from the canal into the parotid gland. The thin skin lining of the bony canal is continuous with the external epithelial layer of the tympanic membrane.
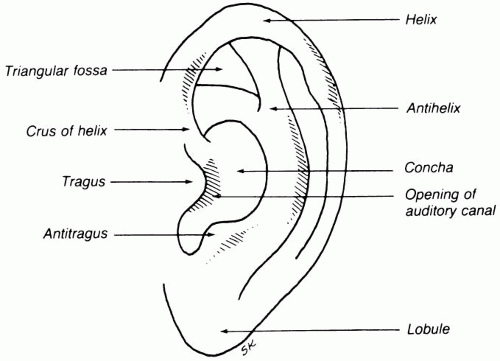 FIG. 2-1. Lateral view of auricle. |
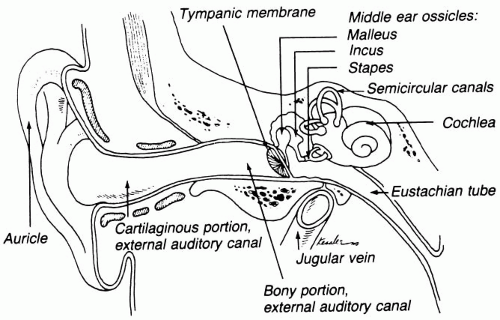 FIG. 2-2. Coronal section of ear. |
The borders of the external ear canal are the temporal lobe of the brain superiorly, the mastoid posteriorly, the temporomandibular joint and parotid gland anteriorly, and the tympanic membrane medially. The auricle and external auditory canal receive their arterial supply from the superficial temporal and posterior auricular branches of the external carotid artery.
Middle Ear
The middle ear (Fig. 2-2) is an air-containing space with bony walls except for the tympanic membrane laterally. Anteriorly the eustachian tube leads downward and medially to the nasopharynx. The medial border is the bony promontory that encloses the basal turn of the cochlea. The middle ear space opens posterosuperiorly through the aditus ad antrum into the mastoid antrum, which is the largest of the mastoid air cells. Three ossicles (malleus, incus, and stapes) conduct sound from the tympanic membrane to the oval window, which is located in a niche just posterior and superior to the promontory (Fig. 2-3). The round window is contained within its own niche just inferior and anterior to the oval window. The malleus is the largest bone. Its handle (manubrium) is embedded in the upper half of the tympanic membrane, and its head, slung from the roof of the middle ear, articulates with the body of the incus. The long process of the incus articulates with the head of the stapes. The stapes foot-plate fits snugly in the oval window.
The tympanic membrane is essentially a three-layered structure composed of an external squamous epithelium, a middle fibrous layer (with radial and circumferential fibers), and an inner mucosal layer. It has a conical configuration and is surrounded by a fibrous annulus (except in the flaccid superior area) that rests in a bony sulcus. The blood supply of the middle ear and mastoid is from branches of the internal maxillary artery. The nerve supply is through the tympanic plexus on the promontory, which contains branches of cranial nerves (CN) V, VII, IX, and X. Abnormalities in the anatomic regions supplied
by these nerves (including teeth, tongue, tonsils, and larynx) may cause pain referred to the ear.
by these nerves (including teeth, tongue, tonsils, and larynx) may cause pain referred to the ear.
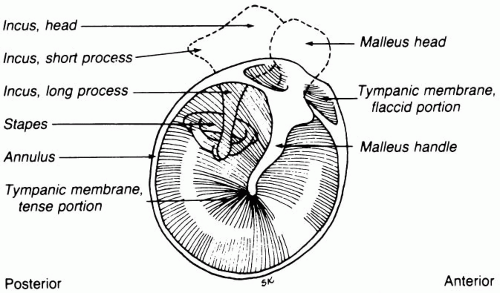 FIG. 2-3. Tympanic membrane and middle ear ossicles. |
Eustachian Tube
The eustachian tube connects the middle ear space with the nasopharynx. Two-thirds are cartilaginous (nearest the nasopharynx) and one-third is bony nearest the middle ear. It is lined with respiratory epithelium. The function of the eustachian tube is to provide air passage from nasopharynx to middle ear to equalize pressure on both sides of the tympanic membrane. It is passively closed at rest and is opened by the action of the tensor veli palatini muscle (innervated by CN V) and thus opens briefly during swallowing. It also can be opened forcibly by means of increasing air pressure in the nasopharynx during Valsalva maneuver. Eustachian tube dysfunction may result in negative pressure and accumulation of serous fluid in the middle ear space.
Inner Ear
The inner ear is composed of the end organs of hearing (cochlea) and equilibrium (labyrinth). Both are contained within a compact bony capsule (otic capsule) within the temporal bone. The snail-shaped cochlea makes two-and-one-half turns. The bony labyrinth is comprised of the vestibule, three semicircular canals, and the vestibular aqueduct. Endolymph, which resembles intracellular fluid in its electrolyte composition, is contained within a continuous closed system within the cochlea and membranous labyrinth. Perilymph, which resembles extracellular and cerebral spinal fluid in its electrolyte composition, surrounds the endolymph containing membranes and does not communicate with the endolymph except under pathologic conditions.
Membranous Cochlea
The membranous cochlea contains three compartments (Figs. 2-4 and 2-5). Two of these, the scala vestibuli (associated with
the oval window) and the scala tympani (associated with the round window), contain perilymph. The third compartment, the cochlear duct, contains endolymph and is bordered by the basilar membrane, on which lies the delicate organ of hearing (organ of Corti) and the thin Reissner’s membrane. Within the organ of Corti are thousands of hair cells that project from the neuroepithelium. The hair cells are responsible for converting mechanical force into an electrochemical impulse interpreted as sound. The hair cells are spatially organized along the basilar membrane in a specific frequency-responsive distribution.
the oval window) and the scala tympani (associated with the round window), contain perilymph. The third compartment, the cochlear duct, contains endolymph and is bordered by the basilar membrane, on which lies the delicate organ of hearing (organ of Corti) and the thin Reissner’s membrane. Within the organ of Corti are thousands of hair cells that project from the neuroepithelium. The hair cells are responsible for converting mechanical force into an electrochemical impulse interpreted as sound. The hair cells are spatially organized along the basilar membrane in a specific frequency-responsive distribution.
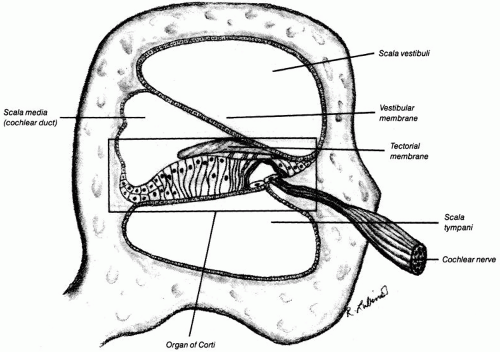 FIG. 2-4. Section through the cochlea. |
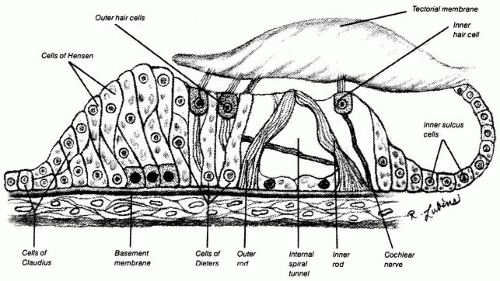 FIG. 2-5. Detail of spiral organ of Corti. (Modified from The ear: organs of hearing and balance. Chicago: Anatomical Chart Company, 2001, with permission.) |
Membranous Labyrinth
The membranous labyrinth consists of the utricle and saccule (sensory end organs responsive to linear acceleration) within the bony vestibule and three semicircular canals (sensory organs responsive to angular acceleration) within their respective bony canals situated at right angles to one another. The membranous semicircular canals are within the bony canals supported in the perilymph by small fibrous strands. The specialized neuroepithelium within the crista of each semicircular canal is located within a bony enlargement known as the ampulla. Both the cochlea and labyrinth receive their blood supply from terminal branches of the basilar artery.
Cranial Nerves
The axons from the hair cells of the cochlea join to form the cochlear portion of the acoustic nerve (CN VIII) while the axons from the specialized epithelium within the labyrinth (utricle, saccule, and semicircular canals) join to form the vestibular portion of the acoustic nerve. Both portions enter the internal acoustic meatus with the facial nerve and separate again to terminate in their respective nuclei.
The facial nerve (CN VII) is intimately related to the ear. The facial nerve courses from the brainstem through the internal auditory meatus between the labyrinth and the cochlea, turns and descends along the medial wall of the middle ear just superior
and posterior to the oval window, and exits through the stylomastoid foramen. In the middle ear, it has a branch to the stapedius muscle and a second branch to the chorda tympani which courses between the incus and malleus and exits anteriorly near the temporomandibular joint. In addition, Jacobsen’s nerve, a branch of the glossopharyngeal nerve (CN IX), runs in a groove across the promontory to provide secretory stimulation to the neighboring parotid gland.
and posterior to the oval window, and exits through the stylomastoid foramen. In the middle ear, it has a branch to the stapedius muscle and a second branch to the chorda tympani which courses between the incus and malleus and exits anteriorly near the temporomandibular joint. In addition, Jacobsen’s nerve, a branch of the glossopharyngeal nerve (CN IX), runs in a groove across the promontory to provide secretory stimulation to the neighboring parotid gland.
Physiology
The function of the ear is to transform mechanical sound energy to bioelectric signals. With two functional ears, sounds can be localized since sound waves reach each ear at slightly different times and intensities. Sound waves strike the tympanic membrane and are transmitted along the intact ossicular chain to the oval window. This sets the perilymph into motion within the cochlea causing a rhythmic vibration of the basilar membrane, which stimulates the hair cells of the neuroepithelium and sets the stage for transmission of a bioelectric signal.
Transfer of sound energy from a gaseous medium (air) to a liquid medium (endolymph) involves a net loss of energy. To overcome this loss, the tympanic membrane and ossicles provide a transformer system composed of a hydraulic action (based on ratio of the area of the vibratory portion of the tympanic membrane to that of the stapes footplate) and a lever system (ossicles). Approximately 30 dB are lost when sound waves pass from air to liquid, but the middle ear recovers 27 dB by the transformer action. The presence of a window on both sides of the basilar membrane allows the pressure wave to pass through a relatively noncompressible liquid housed in a bony chamber (cochlea), such that the round window acts as a relief valve.
Stimulation of the vestibular labyrinth under normal circumstances occurs when the movement of the endolymph within the bony semicircular canal stimulates the hair cells of the cristae located in the ampullae of these semicircular canals. Distortion of the hair cells within the cristae results in a chain of reflexes that produce contraction in the ocular muscles and the muscles of the neck, trunk, and extremities. These responses are responsible for maintaining equilibrium when balance is altered.
Nystagmus is rhythmic, slow, conjugate movement of the eyes in one direction followed by rapid compensatory conjugate movement in the opposite direction. Nystagmus may represent a normal response to specific forms of vestibular stimulation, but when accompanied by vertigo, it may signify a disturbance in the labyrinth, vestibular nerves, or the central nervous system. Vertigo itself represents the sensation of motion and may occur after artificial stimulation of the labyrinth or from a pathologic condition that causes an imbalance between the two labyrinths.
THE NOSE AND PARANASAL SINUSES
Anatomy
External Nose
The skeleton of the external portion of the nose consists of bony and cartilaginous elements. The paired nasal bones that help define the root of the nose articulate superiorly with the
frontal bones and laterally with the nasal processes of the maxillary bone. The rest of the nose derives its configuration from four external nasal cartilages. The two upper lateral cartilages articulate in the midline with the dorsal portion of the nasal septum, and the two lower lateral cartilages provide the structure of the tip. The columella is made of the medial crurae of the lower cartilages (Fig. 2-6).
frontal bones and laterally with the nasal processes of the maxillary bone. The rest of the nose derives its configuration from four external nasal cartilages. The two upper lateral cartilages articulate in the midline with the dorsal portion of the nasal septum, and the two lower lateral cartilages provide the structure of the tip. The columella is made of the medial crurae of the lower cartilages (Fig. 2-6).
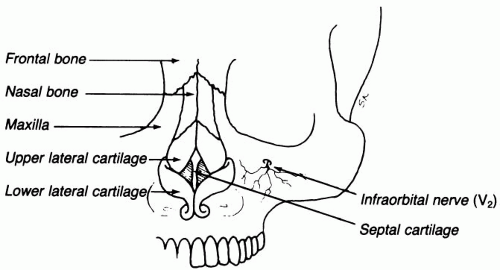 FIG. 2-6. External view of nose. |
BLOOD SUPPLY.
The external nose receives its main blood supply from branches of the facial artery and their anastomoses with the infraorbital artery and the supraorbital and supratrochlear arteries. Venous blood from the external nose drains through the anterior and posterior facial veins into the internal jugular system and through the angular veins that communicate with the orbital and ophthalmic veins that drain into the cavernous sinus. Deep venous connections exist between the infraorbital vein and the pterygoid venous plexus. The veins in this part of the face have no valves; therefore, infections in this region tend to spread centrally more quickly than other regions of the body.
NERVE SUPPLY.
The nerve supply to the external nose is derived from three terminal branches of the trigeminal nerve (CN V), which are the infratrochlear nerve (V1), external nasal nerve (anterior ethmoidal branch of V1), and the infraorbital nerve (V2).
Internal Nose
The internal portion of the nose is divided into two cavities by the nasal septum. The septum is composed of two bones posteriorly (the perpendicular plate of the ethmoid and the vomer) and the quadrangular septal cartilage anteriorly. The entire septum is contained within a mucoperichondrial and mucoperiosteal envelope continuous with the remaining lining of the nasal floor and lateral walls.
The lateral wall of the nose (Fig. 2-7) is complicated in anatomy. Most prominent are the superior, middle, and inferior turbinates (a fourth supreme turbinate is sometimes present). The inferior turbinate is the largest and is rich in vascularity. The middle turbinate is rich in mucous glands and often contains air cells. The nasal meati are named according to the
turbinates that overlie them. The inferior meatus contains the opening of the nasolacrimal duct. The middle meatus contains the ostia of the maxillary, frontal, and anterior ethmoid sinuses. The posterior ethmoid cells and the sphenoid sinus drain into the superior meatus or sphenoethmoidal recess.
turbinates that overlie them. The inferior meatus contains the opening of the nasolacrimal duct. The middle meatus contains the ostia of the maxillary, frontal, and anterior ethmoid sinuses. The posterior ethmoid cells and the sphenoid sinus drain into the superior meatus or sphenoethmoidal recess.
 FIG. 2-7. Lateral wall of nasal cavity. |
BLOOD SUPPLY.
The blood supply of the internal nose is derived from both the external and internal carotid artery systems. The vessels most often involved in epistaxis (Kiesselbach’s area) on the anterior nasal septum are the terminal branches of the anterior and posterior ethmoid arteries, septal branches of the sphenopalatine artery, branches from the nasopalatine artery, and terminal branches of the superior labial artery. The lateral wall of the nose derives its blood supply from both ethmoid arteries and the lateral nasal branches of the sphenopalatine branch of the internal maxillary artery. The venous drainage of the internal nose, like the external nose, can drain into the facial, ophthalmic, and pterygoid systems.
Excluding olfaction, sensation to the internal nose is carried through branches of the first and second divisions of the trigeminal nerve. Sympathetic fibers innervating the blood vessels within the nose are derived from the carotid plexus traveling with the external carotid and from the deep petrosal portion of the vidian nerve. Postganglionic parasympathetic fibers innervating the secretory glands within the nose have their cell bodies within the sphenopalatine ganglion and preganglionic fibers traveling with the vidian nerve. Under normal circumstances, the nose is lined by a respiratory epithelium, which is pseudostratified, ciliated, and columnar.
The paranasal sinuses are paired air-filled spaces lined by mucous membrane. The sinuses develop as outpockets of the nasal mucous membrane at different rates throughout infancy and childhood. The maxillary sinus is the largest and is located within the maxilla just inferior to the orbit. The multiple ethmoid sinuses are located medial to the orbits separated by the
thin lamina papyracea. The ethmoid sinuses are divided into anterior, middle, and posterior groups, all of which are divided into many cells by a network of small bony septa. The frontal sinuses are located anterior to and above the ethmoid sinuses and are divided by a septum. Behind the posterior ethmoid sinuses lie the sphenoid sinuses, which are usually unequally divided by a septum. Vital structures intimately related to the sphenoid sinuses include the pituitary gland, which is located posterosuperiorly, and the internal carotid arteries and the optic nerves, which are located laterally.
thin lamina papyracea. The ethmoid sinuses are divided into anterior, middle, and posterior groups, all of which are divided into many cells by a network of small bony septa. The frontal sinuses are located anterior to and above the ethmoid sinuses and are divided by a septum. Behind the posterior ethmoid sinuses lie the sphenoid sinuses, which are usually unequally divided by a septum. Vital structures intimately related to the sphenoid sinuses include the pituitary gland, which is located posterosuperiorly, and the internal carotid arteries and the optic nerves, which are located laterally.
Physiology
The four vital nasal functions are olfaction, temperature control, humidity control, and particle filtration.
Olfaction
Olfaction occurs through the sensory hairs of CN I, which penetrate the cribriform plate. Although several disorders of olfaction may exist, the most common cause of anosmia (absence of sense of smell) is simple nasal obstruction, as seen in the common cold or nasal polyposis, in which air currents are prevented from reaching the olfactory area.
Air Temperature Control
Inhaled air temperature control is regulated as it passes over the broad surface of the turbinates. The rich capillary network contained within the semierectile tissue allows for effective caloric exchange. Regardless of the temperature of inspired air, air temperature within the nasopharynx rarely fluctuates more than 3°F from normal body temperature.
Humidity Control
The dense mucous blanket provided by the large number of mucous glands within the nasal mucosa allows constant humidification of inspired air. It has been estimated that as much as 1 liter of fluid may be lost through the nose during normal breathing in a 24-hour period.
Particle Filtration
The mucociliary system of the nose provides a protective filtration function against inhaled particulate matter. The submucosal glands and the goblet cells of the respiratory epithelium supply a continuous flow of secretion that forms a viscous blanket (producing over 1 liter per day). The pH of the secretion remains fairly constant at 7 and also contains lysozyme and the secretory immunoglobulin IgA. The rhythmic beating of the epithelial cilia moves this mucous blanket at a rate of several millimeters per minute, which is replaced approximately every 20 minutes.
Other functions of the paranasal sinuses include lightening the skull weight, providing supplemental nasal function, providing an air temperature buffer for the brain, contributing to olfaction, adding resonance to the voice, and providing a bumper-like support to protect the face in trauma.
THE ORAL CAVITY
Anatomy
Lips
The lips form the anterior sphincteric entrance to the oral cavity. The sphincteric function is derived from the orbicularis oris muscle which is innervated by the marginal mandibular and buccal branches of the facial nerve.
Tongue
The most prominent structure in the oral cavity is the tongue, which has a dorsal surface (top) and a ventral surface (bottom). The dorsal surface of the tongue is divided into an anterior two-thirds and a posterior one-third (base) by an inverted V at the posterior portion of the tongue, the apex of which is at the foramen cecum. The anterior two-thirds of the tongue is covered by an abundance of filiform papillae and scattered fungiform papillae. The larger circumvallate papillae are scattered at the base of the tongue. The tongue is comprised of the genioglossus (largest) and paired hyoglossus, styloglossus, and palatoglossus muscles innervated by the hypoglossal nerve (CN XII). Unilateral paralysis of one CN XII results in deviation of the tongue to the ipsilateral side.
The ventral surface of the tongue is continuous with the floor of the mouth and is divided in the midline by the frenulum. A shortened frenulum results in ankyloglossia (“tongue tie”). On either side of the frenulum, are small papillae containing the orifices of the submandibular (Wharton’s) ducts. The mucosa of the floor of the mouth is continuous with the gingiva, which in turn is continuous with the labial and buccal mucosa anteriorly and laterally.
Lateral Walls
The lateral walls of the oral cavity are formed by the buccinator muscle, which lies lateral to the mucosa and is innervated by the buccal branch of CN VII. The parotid (Stensen’s) duct opens into the buccal mucosa opposite the upper second molar bilaterally.
Roof
The roof of the oral cavity is formed by the hard palate (anterior two-thirds) and the soft palate (posterior one-third). The uvula is the muscular organ that hangs from the midline of the soft palate. The palate muscles (levator palatini, tensor veli palatini, and palatopharyngeus) are responsible for most of the motion of the soft palate and are innervated by the vagus nerve except the tensor, which is innervated by the trigeminal nerve. Paralysis of one side of the soft palate results in deviation of the uvula to the opposite side.
Blood Supply
The blood supply to the oral cavity is through branches of the external carotid artery, including the facial and lingual arteries. Venous drainage occurs through the facial veins into the internal jugular vein.
Physiology
The tongue has an important role in deglutition and taste. The peripheral taste receptors are the taste buds in the papillae on the tongue and palate. The fungiform and circumvallate papillae are the most sensitive in terms of taste sensation. The filiform papillae, while most numerous, are considered noncontributory to taste sensation. The conversion of a taste stimulant to a neural response has yet to be elucidated. Afferent taste sensation of the anterior two-thirds of the tongue is carried by chorda tympani, which then travels with the facial nerve, whereas taste sensation of the posterior third of the tongue is transmitted via the glossopharyngeal nerve. In addition to the tongue, taste buds exist on the palate, oropharynx, and hypopharynx. Salty and sweet sensations are detected mostly on the tongue, while the palate is most sensitive to sour and bitter tastes.
THE PHARYNX
Anatomy
The pharynx is divided into the nasopharynx (above the soft palate), the oropharynx (between the tonsillar pillars laterally, the soft palate superiorly, and the epiglottis inferiorly), and the hypopharynx (the portion from the base of the tongue and epiglottis to the cricopharyngeus muscle inferiorly) (Fig. 2-8).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


