Treatment of obstructive diseases of the major salivary glands has undergone a dramatic change in the last 10 to 15 years. New minimally invasive techniques have been developed, covering all different entities that are included in the complex of salivary gland obstruction, and can help the physician to find the right diagnosis and an adequate treatment plan and to perform a gland-preserving form of therapy. Sialolithiasis or stenosis is the cause of about 90% of all obstructive salivary gland diseases. The development of radiologically or fluoroscopically controlled methods, but especially the introduction of sialendoscopy, has led to changes in the treatment protocol. Knowledge from the authors’ experience and from a thorough investigation of the literature has been combined to elaborate algorithms for the treatment of the different obstructive diseases of the salivary glands. Sialoliths and stenoses can be successfully treated by radiologically or fluoroscopically controlled or sialendoscopically based methods in approximately 80% of cases. Extracorporeal shock-wave lithotripsy (ESWL) is successful in up to 50% of cases. Transoral duct slitting is an important method for extraparenchymal submandibular stones, with a success rate of 90%. Operative duct procedures and the combined endoscopic-transcutaneous approach complete the spectrum of treatment modalities of the parotid gland. Sialendoscopy plays a central role in the treatment of obstructive salivary gland diseases, but maximum success can only be attained by the reasonable combination of all these new minimally invasive techniques. Altogether, in well over 95% of cases, resection of the gland can be prevented, thus reducing morbidity and the surgical risks for patients.
Chronic sialadenitis is commonly associated with an acute chronic inflammation and obstruction of the excretory duct. The differentiation between chronic sialadenitis and obstruction of the excretory duct is difficult. The main causes of obstructive disorders are stones in about 60% to 70%, stenosis in about 15% to 25%, inflammation of the duct (sialodochitis) in about 5% to 10%, and other obstructions, such as anatomic variations or foreign bodies, in about 1% to 3%.
Until just a few years ago, the operative removal of the glands was recommended as the therapeutic method of choice in as many as 40% of all cases after unsuccessful conservative treatment. The development of a variety of minimally invasive techniques has led to a fundamental change in therapeutic perspectives. Various forms of therapy for obstructive disorders are meanwhile reported in the literature: interventional sialography and other radiologically controlled methods, such as ultrasound-guided techniques, and sialendoscopy. Sialendoscopy has received broad acceptance in the diagnostic examination and management of obstructive disorders of the salivary glands because of its direct visualization of findings without the use of contrast medium and with the lack of exposure to radiation, combined with a high success rate. Other gland-preserving techniques, such as transoral duct slitting or transcutaneous stone retrieval, have found their way into the therapeutic spectrum for obstructive sialadenitis.
The aim of this article is to present algorithms for the treatment of obstructive diseases of the salivary glands. Experience gained by the authors’ study group and the results gleaned from a thorough research and analysis of the literature form the basis for these algorithms.
Pretherapeutic diagnostic examinations
Ultrasound and sialendoscopy are the authors’ methods of choice for diagnosing sialadenitis. In the absence of ultrasound, sialography is still regarded as a standard technique. Ultrasound allows a presumptive diagnosis to be made quickly, safely, cost effectively, and with great precision. Sialendoscopy serves to provide a direct demonstration of the obstruction and thus allows confirmation of the diagnosis. Furthermore, it can also lead to endoscopy-controlled treatment (interventional sialendoscopy) during the same session.
Algorithm for the treatment of sialolithiasis
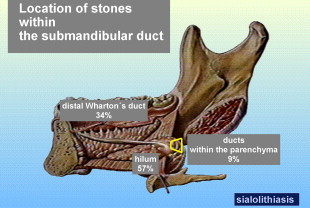
With an incidence of approximately 60% to 70%, stones are the most common cause of all salivary-duct obstructions; their prevalence in the general population is approximately 1%. Conservative measures of treatment like massage of the gland, sialgogues, antiinflammatories, and where indicated, antibiotic medication should precede more invasive measures.
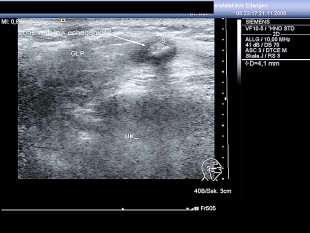
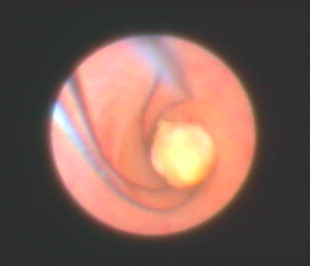
Decisive parameters for the further management are size, location (distal duct, hilar region, intraparenchymal ductal system), number and positional relationship of the stones to the surrounding tissue (adhesive, impacted, mobile). Stone impaction may, for example, be suspected sonographically ( Fig. 1 ) but can only be demonstrated with certainty by sialendoscopy ( Fig. 2 ).

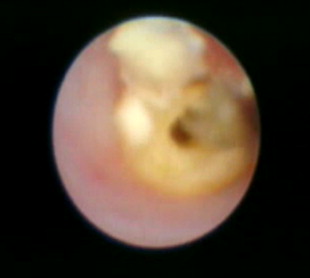
Small (≤5 mm) and mobile stones located in the main excretory duct as far as the hilar region, and possibly even as far as first- and second-order ducts, can be extracted primarily by endoscopically controlled means, in the submandibular and in the parotid gland, with a success rate of 70% to 90% ( Fig. 3 , Video 1 ). Video 1 of a sialendoscopic extraction is found online at http://www.oto.theclinics.com .
Stones of soft consistency with a size of up to 5 to 7 mm may initially be fragmented within the ducts during interventional sialendoscopy and the fragments then retrieved by endoscopically controlled means. Fragmentation may alternatively be accomplished using microinstruments ( Fig. 4 , Video 2 [ Video 2 of intraductal sialendoscopically controlled instrumental fragmentation is found online at http://www.oto.theclinics.com ]) or laser technique ( Fig. 5 ).

Radiologically controlled or fluoroscopic methods are performed with a success rate of up to 80%. Stones that are not accessible using the sialendoscope, those that are impacted, and intraparenchymal stones are disintegrated and fragmented using extracorporeal shock-wave lithotripsy (ESWL). ESWL represents the therapeutic alternative of first choice in many cases of stones of the parotid gland. The mobile fragments can then once again be extracted in an endoscopically controlled manner.
Intractable stones of the papilla and the distal ductal system of the parotid gland can be retrieved by way of an extended papillotomy or distal duct slitting. The majority of these cases require the implantation of a stent to prevent the development of a stenosis. For the submandibular duct, the various modifications of transoral duct slitting are the methods of choice for larger or impacted stones; the success rate amounts to more than 90%. The incision can be done beyond the hilar region as far as intraparenchymal areas.
The combined endoscopic-transcutaneous stone retrieval was developed for therapy-resistant stones of the parotid gland and carries a success rate of as high as 90%. As an alternative to the removal of the gland, repeat injections of botulinum toxin may be administered as the therapy of last choice.
Therapeutic Strategy for Stones of the Submandibular Gland
Only approximately 10% of all stones have an intraparenchymal location ( Fig. 6 ). As a rule, conservative measures are sufficient for stones without symptoms.
Distal Stones and Those in the Main Excretory Duct
Small mobile stones (≤5 mm) are retrieved primarily by interventional sialendoscopy or other interventional methods (sialography, ultrasound-controlled). Concomitant papillotomy may be necessary.
Transoral duct slitting is the treatment of first choice for impacted stones and stones with a size of more than 5 mm. Endoscopic mobilization or fragmentation may be considered for a stone size of 5 to 7 mm, but this is regarded as treatment of second choice.
If several stones are present, they are treated similarly according to their size and may need to undergo a combined form of management.
Stones in the Hilar Region
Small mobile stones (≤5 mm) may be retrieved by interventional techniques. Stones of borderline sizes (5–7 mm) may undergo attempts at endoscopic mobilization and fragmentation, followed by fragment extraction. Transoral-duct slitting is primarily indicated for larger stones or impacted stones ( Fig. 7 ).
Sonographic localization is very helpful for planning the management of smaller impacted stones located deep in the hilar region (from a sialendoscopic view, ducts of the first order) ( Figs. 8–10 ). If the stone can be visualized during sialendoscopy and is palpable, then transoral duct slitting is performed ( Fig. 11 ). ESWL is indicated in visible and impacted stones in the duct system from first order, which are not palpable (in most cases calculi of 5 mm or less in size, Video 3 ), or if the stone is not visible during sialendoscopy. Video 3 of an impacted stone in hilum is found online at http://www.oto.theclinics.com . The indication for ESWL is for impacted, nonpalpable stones in a duct of the first order (usually smaller calculi up to 5 mm in size) or for stones which cannot be visualized during sialendoscopy. If several stones are present, they are treated similarly and may need to undergo a combined form of management. Residual fragments may be retrieved using interventional means.
Intraparenchymal Stones
If the calculi can be visualized during endoscopy, an attempt may be made to extract small mobile stones by endoscopy, mobilization, or fragmentation. Transoral duct slitting with opening of the gland is indicated for large stones, which are palpable from inside the mouth.
If a small stone cannot be visualized endoscopically or cannot be removed endoscopically, then ESWL is indicated. The success rate is significantly reduced with stones larger than 10 mm in size.
Removal of the gland should be undertaken as a therapeutic option if at least three ESWL sessions were unsuccessful or for stones larger than 10 mm in size that cannot be retrieved by the transoral route or for several intraparenchymal stones. [CR] illustrates the algorithm for the management of submandibular stones.
Therapeutic Strategy for Stones of the Parotid Gland
Twenty percent to twenty-five percent of all stones have an intraparenchymal location ( Fig. 12 ). The stones are more commonly impacted (see Fig. 2 ).
Conservative measures may be sufficient for stones with no symptoms (see earlier discussion).
Stones in the Papilla and the Distal Excretory Duct
For visible small stones in the papilla, spontaneous passage may be provoked with the aid of bougienage. Small mobile stones (≤5 mm) are retrieved by interventional sialendoscopy or other interventional methods (sialography, ultrasound controlled). Endoscopic mobilization or fragmentation may be considered for a stone size between 5 to7 mm. Major operative manipulations to the papilla are obsolete as a primary therapeutic measure, as they frequently result in stenosis. A mini-papillotomy may be performed without the risk of creating a stenosis for stones/fragments that have been grasped by various instruments during interventional sialendoscopy, but have proved to be too large for passage through the papilla. A mini-papillotomy consists of a superficial incision in the papilla, not involving the duct epithelium and extending maximally 3 to 4 mm ( Fig. 13 ).
Regardless of the stone location, ESWL is the therapy of choice for impacted stones or stones with a size greater than 5 mm that are not retrievable even by interventional means. Extraction using interventional sialendoscopy is indicated for persistent fragments in the ductal system. If ESWL is not available, stone retrieval may be achieved by a combined endoscopic and transcutaneous approach in the distal excretory duct. If several stones are present, they are treated similarly according to their size and may need to undergo a combined form of management.
Stones in the Middle, Proximal Duct, and Hilar Region
Small mobile stones (≤5 mm) are primarily treated using available interventional methods (sialendoscopy, sialography, or ultrasound controlled) while preserving the gland. ESWL is primarily indicated for small stones that are not amenable to sialendoscopy or for impacted stones. Residual fragments, on the other hand, may be extracted by interventional means.
Patients who have therapy-resistant calculi or a contraindication to ESWL (cardiac pacemaker) are treated by a combined endoscopic-transcutaneous approach. The prerequisite for this is the endoscopic accessibility of the stone.
If several stones are present, they are treated similarly and may need to undergo a combined form of management.
Intraparenchymal Stones
If the calculi can be visualized during endoscopy, an attempt may also be made to extract small mobile stones by endoscopy, mobilization, or fragmentation (see earlier discussion). Alternatively, and in all other cases in which a small stone cannot be visualized during endoscopy, ESWL is performed. Residual fragments, on the other hand, may be retrieved by a combined use of interventional means. Therapy-resistant stones, or patients who have a contraindication to ESWL, are indications for the combined endoscopic-transcutaneous approach. The prerequisite for this is the endoscopic accessibility of the stone.
Parotidectomy is indicated when minimally invasive measures, including ESWL, have not been successful after at least three sessions or several intraparenchymal stones are present (n >3). [CR] illustrates the current therapeutic strategy.
Algorithm for the treatment of sialolithiasis
With an incidence of approximately 60% to 70%, stones are the most common cause of all salivary-duct obstructions; their prevalence in the general population is approximately 1%. Conservative measures of treatment like massage of the gland, sialgogues, antiinflammatories, and where indicated, antibiotic medication should precede more invasive measures.
Decisive parameters for the further management are size, location (distal duct, hilar region, intraparenchymal ductal system), number and positional relationship of the stones to the surrounding tissue (adhesive, impacted, mobile). Stone impaction may, for example, be suspected sonographically ( Fig. 1 ) but can only be demonstrated with certainty by sialendoscopy ( Fig. 2 ).
Small (≤5 mm) and mobile stones located in the main excretory duct as far as the hilar region, and possibly even as far as first- and second-order ducts, can be extracted primarily by endoscopically controlled means, in the submandibular and in the parotid gland, with a success rate of 70% to 90% ( Fig. 3 , Video 1 ). Video 1 of a sialendoscopic extraction is found online at http://www.oto.theclinics.com .



