Purpose
To describe, apply, and test a new ocular grading system for assessing keratoconjunctivitis sicca (KCS) using lissamine green and fluorescein.
Design
Prospective, observational, multicenter cohort study.
Methods
The National Institutes of Health-funded Sjögren’s Syndrome International Registry (called Sjögren’s International Collaborative Clinical Alliance [SICCA]) is developing standardized classification criteria for Sjögren syndrome (SS) and is creating a biospecimen bank for future research. Eight SICCA ophthalmologists developed a new quantitative ocular grading system (SICCA ocular staining score [OSS]), and we analyzed OSS distribution among the SICCA cohort and its association with other phenotypic characteristics of SS. The SICCA cohort includes participants ranging from possibly early SS to advanced disease. Procedures include sequenced unanesthetized Schirmer test, tear break-up time, ocular surface staining, and external eye examination at the slit lamp. Using statistical analyses and proportional Venn diagrams, we examined interrelationships between abnormal OSS (≥3) and other characteristics of SS (labial salivary gland [LSG] biopsy with focal lymphocytic sialadenitis and focus score >1 positive anti-SS A antibodies, anti-SS B antibodies, or both).
Results
Among 1208 participants, we found strong associations between abnormal OSS, positive serologic results, and positive LSG focus scores ( P < .0001). Analysis of the overlapping relationships of these 3 measures defined a large group of participants who had KCS without other components of SS, representing a clinical entity distinct from the KCS associated with SS.
Conclusions
This new method for assessing KCS will become the means for diagnosing the ocular component of SS in future classification criteria. We find 2 forms of KCS whose causes may differ.
Phenotypic characteristics of the eye in Sjögren syndrome (SS) have been a key component in diagnosing the syndrome since its first description by Sjögren in 1933. Rose Bengal (the 4,5,6,7-tetrachloro 2,′4,′5,′7′-tetraiodo form of fluorescein) was used by Sjögren to demonstrate changes in the cornea and interpalpebral areas of the conjunctiva in patients with a form of dry eyes he named keratoconjunctivitis sicca (KCS). Although the use of vital dyes to stain the ocular surface was first reported by Pfluger in 1882, Sjögren was the first to recognize the diagnostic significance of the staining pattern by rose Bengal.
In 1949, Holm attempted to categorize Sjögren’s observations by dividing the pattern into grades A (clinically severe), B (moderate), and C (mild). This scheme was followed in 1969 by a semiquantitative method reported by van Bijsterveld, whose observations became the basis for subsequent grading systems. In 1973, Norn was the first to report the use of lissamine green, an acidic synthetically produced organic food dye, for vital staining of the cornea and conjunctiva. Norn and others noted that although lissamine green had staining properties very similar to rose Bengal, it did not cause the ocular irritation so prominent with rose Bengal.
A 1995 report from the National Eye Institute workshop on clinical trials involving participants with dry eyes outlined a comprehensive new grading system for KCS using fluorescein dye to stain the cornea and rose Bengal to evaluate the conjunctiva. The underlying principle of using different stains for the cornea and conjunctiva provided a significant advance, but the system was not readily adopted because of its complexity. This was followed in 2003 by the Oxford grading scheme developed by Bron and associates, in which fluorescein was used to stain the cornea and either rose Bengal or lissamine green was used to stain the conjunctiva. By counting the number of dots stained with each dye, Bron and associates’ grading scheme became the first quantitative method of accessing ocular changes in patients with KCS; however, the scoring system was never validated with patient data.
The Sjögren’s International Collaborative Clinical Alliance (SICCA) is a National Institutes of Health-funded international registry created to develop standardized classification criteria for SS and to store clinical data and biospecimens collected from the SICCA cohort that range from those with possibly early SS to those with advanced disease, disseminating those data and specimens for future SS research. As part of SICCA, we have adapted from the previous grading systems cited above to develop a new, simplified, quantitative dry eye grading scheme that yields the SICCA ocular staining score (OSS). The SICCA OSS is novel in that it uses lissamine green dye to grade the conjunctiva and fluorescein dye to grade the cornea and is easily applied in clinical practice. The OSS gives equal numerical weight to corneal and conjunctival changes, is less time consuming than previous grading systems, and emphasizes clinical relevance. It is the product of a collaborative effort between SICCA ophthalmologists and researchers in Argentina, China, Denmark, Japan, the United Kingdom, and the United States and represents a new international standard for identifying and grading KCS in these patients.
The objectives of this article are (1) to describe the grading system that produces the OSS; and (2) to analyze the distribution of the OSS among the current participants in the SICCA registry and its association with other phenotypic characteristics of SS (e.g., other ocular, oral, and serologic measures).
Methods
Sjögren’s International Collaborative Clinical Alliance Registry Participant Cohort
To be eligible for the SICCA registry, participants must be at least 21 years of age and have one of the following: (1) a report of dry eyes or dry mouth; (2) bilateral parotid enlargement; (3) a recent increase in dental caries; (4) a previous diagnosis of SS; or (5) elevated titers of antinuclear antibodies, rheumatoid factor, or anti-SS A or anti-SS B antibodies. Participants are recruited through local or national SS patient support groups, healthcare providers, public media, and populations served by all 6 SICCA locations.
Exclusion criteria include known diagnoses of hepatitis C infection, HIV infection, sarcoidosis, amyloidosis, active tuberculosis, graft-versus-host disease, autoimmune connective tissue diseases other than rheumatoid arthritis or lupus, past head and neck radiation treatment, current treatment with daily eye drops for glaucoma, corneal surgery in the last 5 years to correct vision, cosmetic eyelid surgery in the last 5 years, or physical or mental condition interfering with successful participation in the study.
Contact lens wearers are asked to discontinue wear for 7 days before the SICCA examination. We do not exclude participants who are taking prescription drugs that may affect salivary or lacrimal secretion, but do record the use and all other medications currently taken. Those taking cholinomimetic drugs (approximately 10% of the cohort) are asked to discontinue use 1 day before the SICCA clinical evaluation.
Sjögren’s International Collaborative Clinical Alliance Registry Ocular Examination Sequence
The sequence and intervals of these ocular tests are of critical importance to their accuracy and reproducibility. The application of a vital dye or any other substance to the ocular surface can alter the tear film and adversely affect subsequent results. For this reason, the Schirmer test I (without anesthesia) is performed first, followed by instillation of fluorescein dye, determining the TBUT, and grading the corneal fluorescein staining pattern. After fluorescein grading of the cornea, lissamine green dye is applied and the conjunctiva is examined quickly and graded before the dye diffuses or the intensity of staining diminishes. The total time for the complete eye examination is approximately 20 minutes.
The Schirmer test
The Schirmer test I (without anesthesia) is carried out before any drops are instilled in the eye. Standardized Schirmer strips are bent at the notch and placed carefully over the lower lid margin as far toward the temporal angle of the lids as possible. The patient is instructed to keep her or his eyelids closed during the test. Strips remain in place for 5 minutes, or until they are completely saturated with tears. After 5 minutes, wetting of the strips is measured using the millimeter scale on each strip (Eagle Vision, Memphis, Tennessee, USA; cat no. 0039). It is generally agreed that a Schirmer I test of 5 mm or less in 5 minutes is abnormal, but the variability of the test, even in normal eyes, invalidates any direct comparison between individual patients with KCS and normal controls. Immediately after removing the strips, 1 drop of 0.5% fluorescein (Leiter’s Pharmacy, San Jose, California, USA) is applied to the conjunctival fornix of each eye, and the participant told to squeeze the eyelids tightly to remove excess dye. During this interval, the tear strips are processed by cutting them lengthwise and placing them in cryovials to be frozen and banked.
Tear break-up time
Two minutes after the application of fluorescein dye the TBUT is measured at the slit lamp. The oculars are set at ×10 magnification and the illumination is set on high, using the cobalt blue filter over the light source. The patient is asked to blink once and then keep her or his eyes open. The TBUT, defined as the time in seconds between the patient’s last blink and the first appearance of a random dry spot on the corneal surface, is measured 3 times and the mean value is recorded. It is generally accepted that a TBUT of less than 10 seconds is abnormal. Mengher and associates confirmed this observation by comparing TBUT values in 33 KCS patients with 66 normal controls. The value of 10 seconds proved to be the critical level separating the 2 groups with a sensitivity of 82% and specificity of 86%. The presence or absence of mucus shreds, debris, or both in the tear film is noted.
Corneal fluorescein staining pattern (step 1 of the ocular Sjögren’s International Collaborative Clinical Alliance grading)
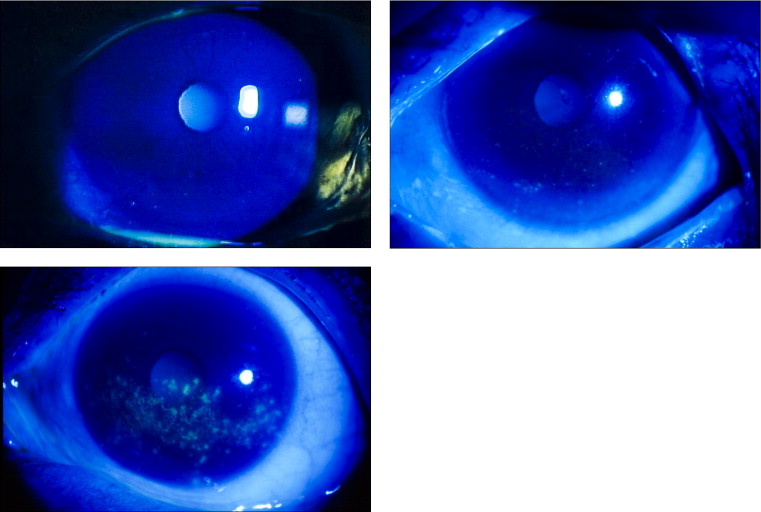
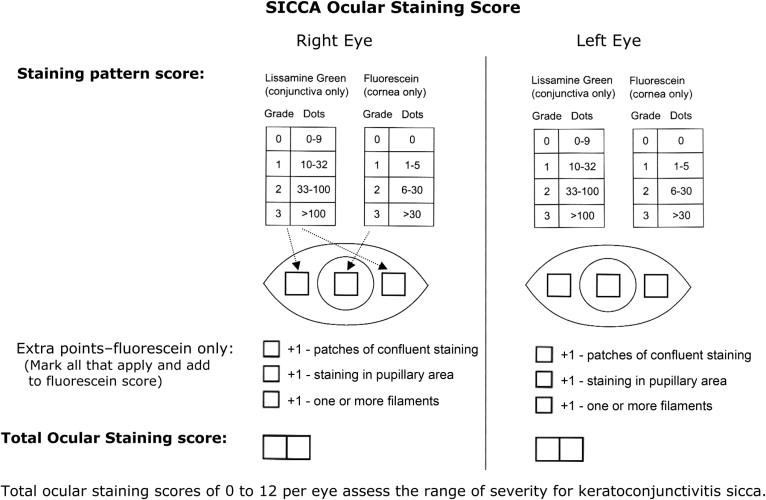
Each cornea is examined at the slit lamp using the cobalt blue filter. Corneal epithelial staining is a dynamic and time-sensitive process; therefore, to insure reproducibility, grading of the fluorescein pattern is initiated consistently between 4 and 8 minutes after instillation. Punctate epithelial erosions (PEEs) that stain with fluorescein are counted and scored. If there are no PEE, the score is 0. If 1 to 5 PEEs are seen, the corneal score is 1 ( Figure 1 , Top left); 6 to 30 PEEs are scored as 2; and more than 30 PEEs are scored as 3. An additional point is added if: (1) PEE occurred in the central 4-mm diameter portion of the cornea ( Figure 1 , Top right); (2) 1 or more filaments is seen anywhere on the cornea; or (3) 1 or more patches of confluent staining, including linear stains, are found anywhere on the cornea ( Figure 1 , Bottom). The total fluorescein score for the cornea (the PEE grade plus any extra points for modifiers) is noted in the central square of the SICCA ocular staining score form ( Figure 2 ). The maximum possible score for each cornea is 6.
External eye examination at the slit lamp
Examination of the external eye is performed after fluorescein instillation but before the application of lissamine green. The slit lamp is used with the same magnification but with decreased illumination using a neutral density filter. Because this portion of the eye examination is not time dependent, it is performed slowly and carefully, noting the presence or absence of abnormalities of the lids, conjunctiva, and cornea, as well as specific diseases that may affect the OSS, such as lagophthalmos, entropion, pterygium, and pingueculum. Special attention is directed toward recognizing clinical signs of blepharitis (ulceration around the base of the lashes, collarettes, misdirected lashes, absent lashes, poliosis, and tylosis) as well as evidence of meibomitis (inflammation of the meibomian glands, plugging of the orifices with inspissated secretions, expression of thick material from the glands, lid telangiectasia, and signs of rosacea).
Conjunctival lissamine green staining pattern (step 2 of the ocular Sjögren’s International Collaborative Clinical Alliance grading)
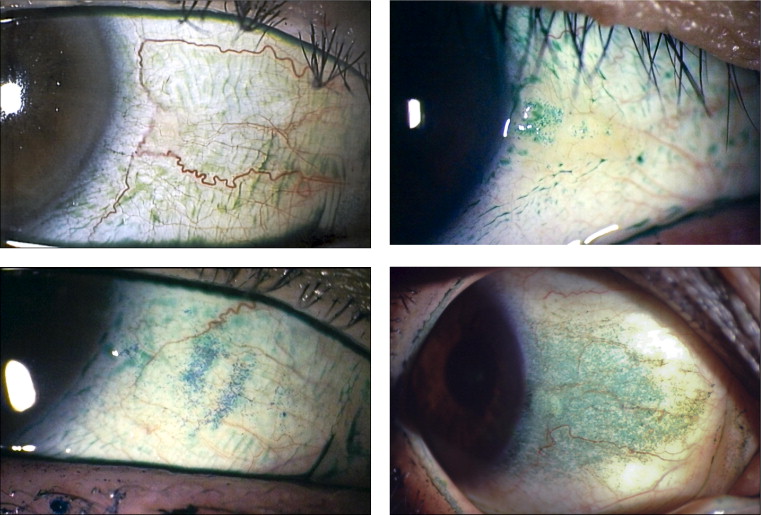
After the external examination, 1 drop of 1% lissamine green dye (Leiter’s Pharmacy) is applied to the inferior conjunctival fornix of both eyes. The conjunctivae are examined with the slit lamp at ×10 magnification, using a neutral density filter over the light source to avoid blanching of the conjunctiva. It is important to examine and grade the eyes immediately after instilling lissamine green dye because the intensity and extent of the ocular staining diminishes rapidly after the first 2 minutes. It is also important for the patient to blink several times to keep dye from pooling in the conjunctival folds, which can mimic conjunctival staining. If adequate dye is not instilled initially, a second drop can be given and the examination performed immediately thereafter. In the OSS, grade 0 ( Figure 3 , Top left) is defined as 0 to 9 dots of lissamine green staining of the interpalpebral bulbar conjunctiva (nasal and temporal bulbar conjunctivae graded separately); grade 1 ( Figure 3 , Top right) is defined by the presence of 10 to 32 dots; grade 2 ( Figure 3 , Bottom left) is defined by the presence of by 33 to 100 dots; and grade 3 ( Figure 3 , Bottom right) is defined by the presence of more than 100 dots. Because of the difficulty of counting individual dots in a moving eye at the slit lamp, any area of confluent staining of 4 mm 2 or more is considered to be more than 100 dots. A fourth grade consisting of totally confluent staining initially was considered, but later was determined not to add quantitatively to the diagnostic grading scheme, although it could be qualitatively meaningful for monitoring treatment in patients with KCS. Nasal and temporal areas of the conjunctiva are graded separately with a maximum score of 3 for each area or a total maximum score of 6 for each eye (nasal plus temporal). The total OSS for each eye is the summation of the fluorescein score for the cornea and the lissamine green scores for the nasal and temporal bulbar conjunctiva. Therefore, the maximum possible score for each eye is 12. The eyes are graded separately and the scores are recorded on the SICCA ocular staining score form ( Figure 2 ) at each patient visit. Staining of pinguecula, pterygia, and artifacts caused by Schirmer strips are not included in the score.
Interpretation of the Ocular Staining Score
An OSS higher than 0 is considered to be abnormal and may be a sign of KCS, but scores of 1 or 2 also can represent a late staining artifact if interpretation of the fluorescein corneal staining pattern is delayed beyond 8 minutes. Because this could lead to a high level of misclassification, an abnormal OSS is defined as being a score of 3 or more.
Statistical Analyses
We computed standard summary statistics to describe the SICCA cohort characteristics with respect to eye symptoms, use of ophthalmic drops, use of systemic anticholinergic drugs, diseases affecting the bulbar conjunctiva or lids, results from the Schirmer test, TBUT, and the OSS. We used a signed-rank test to evaluate the difference between right and left eye with respect to those tests performed on both eyes (i.e., Schirmer, TBUT, OSS) to determine if it would be appropriate to use either the mean or the maximum score between the right and left eye.
We used a proportional Venn diagram to visualize the interrelationships between an abnormal OSS (≥3) or KCS and the other 2 main phenotypic characteristics of SS (an LSG biopsy yielding a diagnosis of focal lymphocytic sialadenitis and a focus score of more than 1, and positive serologic results for anti-SS A or anti-SS B antibodies). This also allowed visualization of the extent of overlap between cohort participants with one or more of these 3 characteristics.
We explored specific factors that may be associated with KCS (with or without the other 2 main phenotypic characteristics of SS). Factors such as lid and conjunctival diseases and anticholinergic medications may cause dry eyes in the absence of SS. It is thus important to explore their association with KCS (with or without the other 2 main phenotypic characteristics of SS). We used contingency table methods, or nonparametric tests when relevant, to explore these associations.
Results
Eye-Related Characteristics Among Participants in the Sjögren’s International Collaborative Clinical Alliance Registry
Among the 1208 participants for whom data were available as of September 15, 2008, the vast majority were women (93%), with a median age of 55 years (range, 21 to 90 years). The cohort was predominantly white (43%) and Asian (38%). A large proportion (85%) reported symptoms of dry eyes, and among those, 43% reported that they had had these symptoms for more than 5 years ( Table 1 ). A quarter of the participants (24%) reported having eye redness half of the time or more, and the same proportion reported an inability to produce tears. There was a widespread use of artificial tears, with 32% reporting use 1 to 3 times per day and 29% reporting use 4 or more times per day. Only 8% reported using cyclosporine drops, and 5% reported using corticosteroid drops. With respect to lid and conjunctival diseases, the most common condition was the presence of a pingueculum (28%), followed by meibomitis (15%) and blepharitis (11%), either unilaterally or bilaterally.
| Eye-Related Characteristics | No. | % a |
|---|---|---|
| Symptoms | ||
| Reported symptom of dry eyes | 1025 | 85 |
| Duration since onset of dry eyes (yrs) b | ||
| ≤1 | 156 | 16 |
| 1; ≤2 | 119 | 12 |
| >2; ≤5 | 280 | 29 |
| >5; ≤10 | 214 | 22 |
| >10 | 207 | 21 |
| Reported eye redness | ||
| Never | 441 | 37 |
| Sometime | 470 | 39 |
| Half of the time or more | 289 | 24 |
| Inability to produce tears | 290 | 24 |
| Use of ophthalmic drops | ||
| Frequency of artificial tear use: | ||
| Never | 468 | 39 |
| 1 to 3 times/day | 381 | 32 |
| 4 times/day or more | 348 | 29 |
| Use of medicated drops c | ||
| None | 851 | 71 |
| Cyclosporine | 80 | 8 |
| Antibiotic | 99 | 10 |
| Steroid | 45 | 5 |
| Other | 99 | 10 |
| Lid and conjunctiva diseases (unilateral or bilateral) d | ||
| Pingueculae | 334 | 28 |
| Meibomitis | 184 | 15 |
| Blepharitis | 134 | 11 |
| Punctal occlusion (lower) | 93 | 8 |
a Column percent may not sum to 100% for some variables because of rounding.
b Median duration since onset of dry eyes: 51 months (6.7 years); range, < 1 to 723 months.
c Column percent does not add up to 100% because participants may use more than 1 type of medicated drops.
d Other conditions affecting lid or conjunctiva, such as lagophthalmos, entropion, or ectropion, were diagnosed in < 2% of participants.
As described earlier, the OSS may have a value ranging from 0 (no corneal or conjunctival staining detected) to 12 for each eye. We used the maximum OSS between the right and left eye because 80% of participants had a minimal difference of 0 or 1 between the 2 eyes. However, the TBUT and Schirmer test had skewed distributions and higher variability between right and left eyes; therefore, we used the mean TBUT and Schirmer test values between the 2 eyes for each participant.
Interrelationship Between Abnormal Ocular Staining Score, Labial Salivary Gland Biopsy Focus Score > 1, and Presence of Anti-Sjögren Syndrome A or B Antibodies
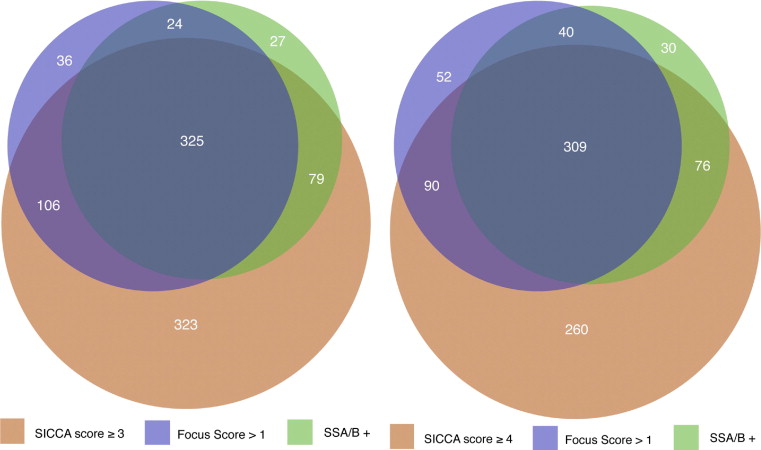
A total of 920 participants in the SICCA registry had at least 1 of 3 phenotypic characteristics thought to be associated with SS: an abnormal OSS of 3 or more, focal lymphocytic sialadenitis with a focus score of more than 1, positive serologic results for anti-SS A or B antibodies, or a combination thereof. These participants were included in a proportional Venn diagram, which revealed that 28% had all 3 characteristics, whereas 28% had an abnormal OSS only, 3% had an abnormal focus score only, and 2% had a serologic results for anti SS A or B antibodies in the absence of the other 2 characteristics ( Figure 4 , Left). To explore whether the level at which we defined an abnormal OSS may explain the much larger proportion of participants with a positive OSS only (as compared with those with either a focus score of more than 1 or with positive serologic results for anti-SS A or B antibodies or both), we also constructed a Venn diagram with an abnormal OSS defined as 4 or more ( Figures 4 , Right). Although the overlap between groups shifted slightly, the large proportion of participants with abnormal OSS only remained (at 22%).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


