Purpose
To test whether the minimum rim area assessed by spectral domain optical coherence tomography (SD-OCT), based on the shortest distance from the Bruch membrane opening (BMO) to the inner limiting membrane, corresponds more closely to retinal nerve fiber layer (RNFL) thickness and visual field mean deviation (MD) than current rim measures in early glaucoma.
Design
Prospective cross-sectional study.
Methods
We studied 221 participants with non-endstage glaucoma or high-risk ocular hypertension and performed standard automated perimetry. We received SD-OCT and confocal scanning laser ophthalmoscopy (CSLO) scans on the same day. Rim area measured by CSLO was compared with 3 SD-OCT rim measures from radial B-scans: horizontal rim area between BMO and inner limiting membrane within the BMO plane; mean minimum rim width (BMO-MRW); and minimum rim area (BMO-MRA) optimized within sectors and then summed. Correlations between these measures and either MD from perimetry or RNFL thickness from SD-OCT were compared using the Steiger test.
Results
RNFL thickness was better correlated with BMO-MRA (r = 0.676) or BMO-MRW (r = 0.680) than with either CSLO rim area (r = 0.330, P < 0.001) or horizontal rim area (r = 0.482, P < 0.001). MD was better correlated with BMO-MRA (r = 0.534) or BMO-MRW (r = 0.546) than with either CSLO rim area (r = 0.321, P < 0.001) or horizontal rim area (0.403, P < 0.001). The correlation between MD and RNFL thickness was r = 0.646.
Conclusions
Minimum rim measurements from SD-OCT are significantly better correlated to both RNFL thickness and MD than rim measurements within the BMO plane or based on the clinical disc margin. They provide new structural parameters for both diagnostic and research purposes in glaucoma.
Understanding the relationship between structural and functional damage in glaucoma has been a key aim for many years. For example, in the United States, the National Eye Institute and the Food and Drug Administration indicated that structural measures could be used as endpoints in clinical trials for glaucoma treatments if they demonstrated a strong correlation with functional measures, with R 2 ≈ 0.9. While this may seem unrealistic, better understanding of this relationship would aid attempts to combine structural and functional measures to improve assessment of disease stage and progression. However, advances on this front have been limited by 2 key factors. First, inter-individual variability in both structural and functional measures is considerable. The non-neural (vascular and glial) component of both the optic nerve head rim tissue and the retinal nerve fiber layer varies with individuals, and the manner in which each changes with age and disease may differ. In normal, healthy human eyes, there is little correlation between retinal nerve fiber layer (RNFL) thickness and contrast sensitivity, and in healthy eyes of nonhuman primates there is little correlation between RNFL thickness and total optic nerve axon count. Second, both structural and functional tests contain significant intra-individual inter-test variability. For example, when visual field sensitivity measured by standard automated perimetry has declined to 15 dB, test-retest variability is reported to have a standard deviation of up to 8 dB, so the 95% confidence interval for retest sensitivity covers the majority of the perimeter’s effective dynamic range. This means that even if the underlying structure-function association were perfect, its strength would be masked by this substantial variability.
Much previous work has relied on performing functional testing with standard automated perimetry and structural testing with confocal scanning laser ophthalmoscopy (CSLO). Recently, Reis and associates have demonstrated that CSLO does not measure the neuroretinal rim area accurately because important subsurface structures are not readily identifiable on CSLO scans. They showed that “the basis for current rim measurements lacks a solid anatomical foundation because (1) the clinical DM (disc margin) is not a consistent outer border of the rim tissue and (2) the orientation of neural tissue in the optic nerve head is not accounted for.” This could be a significant contributing factor to the variability of the structure-function relation when structure is assessed using CSLO. Improving the structure-function relation therefore requires new and improved testing methodologies that have stronger links to anatomy and hence lower variability, for structural as well as functional testing.
Recently, optical coherence tomography (OCT) has been developed. It has been widely used to measure RNFL thickness at a specific angular eccentricity from the center of the optic disc. The RNFL thickness and retinal nerve fiber layer cross-sectional area measures from CSLO are suboptimal because they are based on the vertical distance between the tomographically determined retinal height and a reference plane, and hence are actually measures of relative height rather than the true thickness of any retinal layer. By contrast, the RNFL thickness measure is the distance between the anterior and posterior borders of the highly reflective nerve fiber layer so should reflect the targeted anatomy better.
OCT can also be used to perform scans through the optic nerve head. OCT reveals subsurface structures that are not evident using previous techniques, such as CSLO or stereophotography. Time-domain OCT has been shown to improve the correlation between global RNFL thickness and functional measures from 0.33 (using CSLO) to 0.48 (using OCT). The more recent development of spectral-domain OCT (SD-OCT) could improve this relationship even further, given its greater axial resolution and that its faster speeds can reduce motion artifact within denser scan patterns. Better methods to quantify SD-OCT images are being developed. Povazay and associates suggested that rim could be better defined as the area of a surface extending from the Bruch membrane opening (BMO) to the inner limiting membrane. Strouthidis and associates demonstrated, using SD-OCT, that this rim parameter was both reliable and sensitive in a longitudinal study of nonhuman primates with experimental glaucoma and in studies of acute intraocular pressure elevation. Reis and associates also measured this using SD-OCT, and showed that it reflected the anatomy of the optic nerve head better than the clinically visible disc margin. This would prevent the problem noted above, whereby current clinical measurements of the rim were not consistently referenced to any given anatomic structure. By removing this large source of anatomic variability, this type of SD-OCT–based assessment of the neuroretinal rim should be more easily comparable among individuals, improving the ability to detect the presence of glaucomatous damage and its progression.
Different variants of neuroretinal rim assessment are considered in this article, as detailed in the Methods section. First, a horizontal rim area measurement is considered, giving the most direct analogous measurement to current rim assessment. For example, this is the same method used by the Cirrus SD-OCT instrument (Carl Zeiss Meditec, Dublin, CA, USA) to generate a rim area measurement. Second, a mean minimum rim-width measurement from BMO (BMO-MRW) is considered, along an angle that varies in radial scans, in order to represent the minimum distance from the BMO to the inner limiting membrane within each radial scan around the optic nerve head rim, similar to the technique proposed by Povazay and associates and Chen. Unlike the clinical disc margin, BMO is an actual anatomic boundary of the neuroretinal rim tissue. BMO-MRW therefore represents an accurate estimate of the minimum width of the neural tissues relative to each BMO point within the plane of each radial B-scan. Finally, this minimum rim width is used to estimate the minimum rim area (BMO-MRA) through which the axons must pass. This adjusts for the fact that the BMO-MRW will be related to disc size and not just the number of axons.
This study compares current disc-margin–based rim area measurements from CSLO with these new BMO-based measurements from SD-OCT. The starting point for the comparison is the principle that a sound measurement of the neuroretinal rim should correlate well with RNFL thickness (since the same axons compose both) and with function (since glaucomatous loss of RNFL thickness is associated with concomitant loss of function). This article aims first to determine whether horizontal or minimum measurements of the rim based on BMO as assessed by SD-OCT are better correlated with RNFL thickness than are the current rim area measurements based on CSLO. Second, the article aims to determine whether these new measures of optic nerve head neuroretinal rim tissue also result in a stronger correlation between visual field mean deviation (MD) and optic disc rim structure.
Methods
Participants
Data from 221 participants with non-endstage glaucoma (ie, with remaining measurable visual function) or with ocular hypertension plus risk factors for glaucoma were taken from the ongoing Portland Progression Project, a prospective study of the course and risk factors for glaucomatous progression. All protocols were approved and monitored by the Legacy Health Institutional Review Board and adhere to the Health Insurance Portability and Accountability Act of 1996 and the tenets of the Declaration of Helsinki. All participants provided written informed consent for their participation in the study once all of the risks and benefits of their involvement were explained to them.
At study entry, participants had either a clinical diagnosis of early glaucoma, or they had ocular hypertension (untreated IOP greater than 22 mm Hg) and their physicians had determined that they had glaucomatous optic neuropathy and/or suspicious optic nerve head appearance (cup-disc ratio asymmetry >0.2; neuroretinal rim notching or narrowing; or disc hemorrhage) and/or one or more other risk factors for glaucoma (eg, age >70, systemic hypertension, migraine, diet-controlled diabetes, peripheral vasospasm, African ancestry, or self-reported family history of glaucoma). Participants were excluded if they had other factors (diseases and/or medications) likely to affect the visual field or if they had undergone ocular surgery (except for uncomplicated cataract surgery). Eyes with visual acuity worse than 20/40 were also excluded so as to remove participants with worse-than-mild media change or cataract.
Testing Protocol
Participants underwent functional testing using standard automated perimetry, structural testing using CSLO, stereo-optic disc photography (3-Dx; Nidek, Gamagori, Japan), and structural testing using SD-OCT, all on the same day. Demographic data and intraocular pressure were also recorded. Data were used from the earliest visit at which testing was carried out, and reliable results (as defined below) were obtained for all 3 tests. When suitable data were available for both eyes of a participant, the eye with the better quality SD-OCT scan was chosen, or 1 eye was arbitrarily chosen if they were equal.
Visual field testing was performed using a Humphrey Field Analyzer II (Carl Zeiss Meditec, Dublin, CA, USA), employing the 24-2 testing pattern and conventional test procedures. The Swedish Interactive Testing Algorithm was used for all testing. An optimal lens correction was placed before the tested eye, and the fellow eye was occluded by a white plastic eye patch. All participants had previous experience with visual field testing prior to entering the study, and most had undergone multiple previous tests. Only reliable tests were included; they were defined as ≤33% false-negatives and ≤15% false-positives, and either ≤20% fixation losses or confirmation by the monitoring technician that eye position remained stable throughout the test (because fixation losses can be erroneously reported when the perimeter’s initial automated mapping of the blind spot is inaccurate). The mean deviation (MD) index was used to characterize the degree of functional damage.
CSLO optic nerve head scanning was performed using a Heidelberg Retina Tomograph Classic (Heidelberg Engineering, Heidelberg, Germany) following standard operating procedures. Scans of acceptable quality as judged by the experienced operator were included. The topography standard deviation was always better than 40 μm. The disc margin was marked by an experienced clinician (author C.F.B.) guided by stereophotographs that were acquired on the same day. The CSLO neuroretinal rim area was generated using the instrument’s standard reference plane, defined as 50 μm below the average topography value at positions between 350 degrees and 356 degrees on the marked disc margin.
Standard SD-OCT imaging was performed using a Heidelberg Spectralis (Heidelberg Engineering) with an 870 nm light source. All SD-OCT datasets had a quality score above 15. A peripapillary circle scan with a fixed 6 degree radius centered on the optic nerve head was performed, and the automated delineation of the resulting image was examined and refined by experienced technicians. This was used to calculate the average RNFL thickness measurement. In addition, 48 radial B-scans centered on the optic nerve head were captured, and a subset of 24 scans (every alternate B-scan) were manually delineated using custom multiview software using a single delineator for each eye (1 of 2 delineators for the entire dataset) to determine the positions of the inner limiting membrane and the BMO, as seen in Figure 1 . These delineated landmarks were combined to provide a 3-dimensional representation of the inner limiting membrane and BMO. Neuroretinal rim measurements were then calculated.
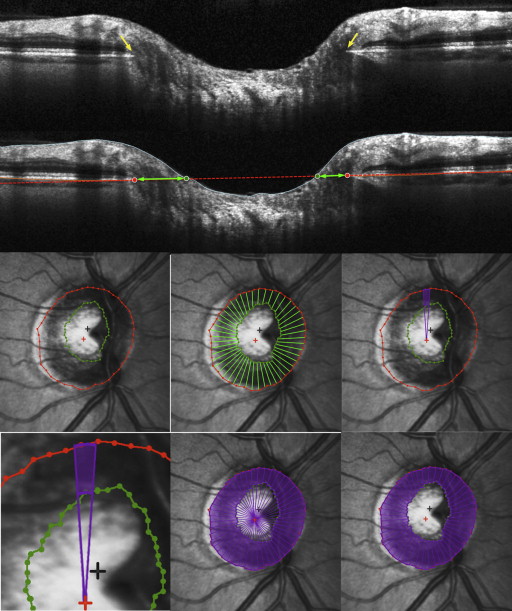
Optical Coherence Tomography Parameterization
The horizontal rim area was designed to resemble conceptually the parameter CSLO rim area and the current SD-OCT rim assessment and to mimic most closely a clinician’s rim assessment. It was based on the distance from the BMO to the inner limiting membrane along the plane of the BMO within each radial B-scan (horizontal), as indicated by the green arrows in Figure 1 . This gives 48 horizontal rim-width measurements (2 for each of the 24 delineated B-scans). For each of these measurements, the corresponding area was calculated using a circular section 7.5 degrees wide and an appropriate diameter, r (based on the distance from the BMO centroid to the BMO in that radial B-scan), as shown by the green outline in Figure 1 . Specifically, the sectoral horizontal rim area equals the difference between the areas of two 7.5 degree circular sectors, one of radius r and one of radius (r – horizontal rim width). These sectoral areas were added to give the overall horizontal rim area measure. For eyes in which the cup was so shallow that the inner limiting membrane never crossed the plane of the BMO, the horizontal rim area was set to equal the entire area enclosed by the BMO. This measure is similar to the rim area measure produced by the Cirrus SD-OCT research software, which performs the same calculation using a reference plane 200 μm anterior to the BMO. BMO points from locations around the optic nerve head generally do not all lie within a single plane (unlike the single depth used to define the CSLO reference plane), but instead form a 3-dimensional elliptical ring with varying axial depths.
The BMO-MRW was based on the distance from the delineated BMO point to the closest point on the inner limiting membrane within each radial B-scan, as first described by Povazay and associates and as indicated by the yellow arrows in Figure 2 . This minimum will occur at an angle θ to the BMO plane (as marked in blue) that can vary between the different radial scans in a given eye. Note that this represents the MWR from each delineated BMO point within 1 side of the radial B-scan, within the plane of the acquired B-scan rather than the global minimum distance to the inner limiting membrane from that BMO location (which would require interpolation of the inner limiting membrane surface between the available B-scans). These rim widths were then averaged across sectors to give the global measure BMO-MRW.
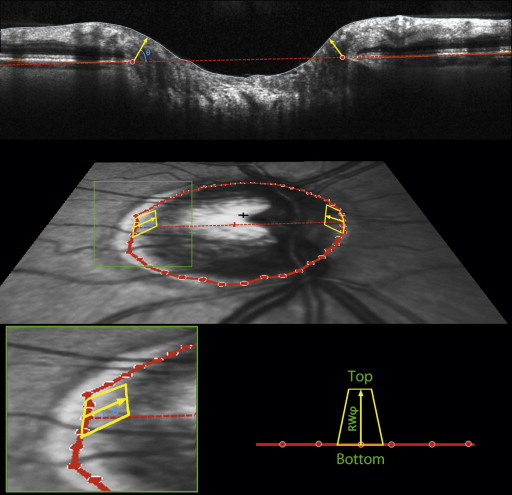
The motivation for assessing this minimum distance is that it approximates the smallest cross-sectional area through which nerve fibers must pass en route from the retina to the optic nerve for a particular part of the optic nerve head. However, it does not provide a true surrogate measure for the number of axons because the same BMO-MRW would correspond to a larger cross-sectional area in eyes with larger discs. Thus, the number of axons would likely better correlate with the minimum cross-sectional area (BMO-MRA) through which the axons pass than with BMO-MRW.
BMO-MRA was estimated as the sum of the areas of 48 trapeziums, each extending from a delineated BMO point to the inner limiting membrane at angle φ above the BMO plane, as indicated by the yellow outlines in Figure 2 . One such trapezium is associated with each delineated BMO point, defined as being at radius r from the BMO centroid. The base of the trapezium then extends halfway to the adjacent radials, so it has a length of 2πr/48. The height of the trapezium is set to equal the rim width at angle φ above the BMO plane in that radial, RW φ , as shown by the yellow arrows in Figure 2 . The top of the trapezium is then at horizontal distance (r − RW φ *cos(φ)) from the BMO centroid. This means that the length of the top is given by 2πr/48*(r − RW φ *cos(φ)). Within each radial, the angle φ was optimized to give the smallest rim area. This means that φ does not necessarily equal θ, the angle of the MRW measurement. They are shown as being the same in Figure 2 for simplicity. For example, consider the case where the rim width perpendicular to the BMO plane (ie, φ = 90°) is 100 μm, and the width parallel to the BMO plane (ie, φ = 0°) is 105 μm, with radius r = 1000 μm. The corresponding sectoral area from the above formulas measured perpendicular to the BMO plane is then 13090 μm 2 , whereas the area parallel to the BMO plane is 13023 μm 2 . In this example, this sector’s contribution to BMO-MRW would be measured at θ = 90 degrees, whereas for BMO-MRA it would be measured at φ = 0 degrees. θ is chosen to minimize the rim width, whereas φ is chosen to minimize the rim area. Supplementary Figure S1 shows a demonstration of this in schematic form. The areas of the sectoral trapeziums were calculated based on these dimensions and added together to give the global minimum rim area measure BMO-MRA. Unlike the horizontal rim area above, these minimum rim measures are not affected by the possibility that the cup may not break than the BMO plane.
The relationship between the mean RNFL thickness and the corresponding cross-sectional area does not depend on the disc circumference, with one being a multiple of the other. Even though we report an RNFL thickness measure, it can be treated the same as an area measure, in particular allowing the relationship between the RNFL thickness and the rim area to be modeled using a linear fit. We chose to use RNFL thickness because it has been more commonly used in the literature, whether using temporal domain or (as in this study) or SD-OCT.
Data Analysis
The primary outcome measures were the correlations between each of the neuroretinal rim measures (CSLO rim area, horizontal rim area, BMO-MRW, and BMO-MRA) and either RNFL thickness or function (MD). Pearson correlations were used and were compared using the Steiger Z 2 * test for nonindependent data.
It has been suggested that structure and function are better correlated when the functional measures are expressed on a linear, rather than a logarithmic (dB) scale. Therefore, this analysis was repeated after transforming the functional data onto a linear scale proportional to 1/Contrast. To achieve this, pointwise total deviation values (TD) were converted to 10 TD/10 , and then these values were averaged to give the index linearized MD. We have previously reported that this transformation may exaggerate variability at locations with above-normal sensitivities. Therefore, another index was calculated in the same manner after first capping all TD values at zero, capped linearized MD = mean (10 min(TD, 0)/10 ).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


