20-Gauge Sutured Wound Construction and Closure
 Whereas 25-gauge vitrectomy is usually performed transconjunctivally with trocar-cannula systems, 20-gauge vitrectomy usually requires conjunctival incision, exposure of the anterior sclera, and sclera closure and conjunctival reapproximation with sutures. Despite performing nearly all of their vitrectomies with 25-gauge techniques, the authors still find the need for creation of 20-gauge incisions. These may be required, for example, to introduce a 20-gauge fragmenter handpiece to remove pieces of dropped dense nucleus in the vitreous or to introduce diamond-coated 20-gauge forceps to remove intraocular foreign bodies. This chapter will focus on techniques of creation and closure of 20-gauge incisions.
Whereas 25-gauge vitrectomy is usually performed transconjunctivally with trocar-cannula systems, 20-gauge vitrectomy usually requires conjunctival incision, exposure of the anterior sclera, and sclera closure and conjunctival reapproximation with sutures. Despite performing nearly all of their vitrectomies with 25-gauge techniques, the authors still find the need for creation of 20-gauge incisions. These may be required, for example, to introduce a 20-gauge fragmenter handpiece to remove pieces of dropped dense nucleus in the vitreous or to introduce diamond-coated 20-gauge forceps to remove intraocular foreign bodies. This chapter will focus on techniques of creation and closure of 20-gauge incisions.CONJUNCTIVAL INCISIONS
Care should be taken to avoid highly scarred or vascular areas, filtering blebs, setons, and flaps for sutured intraocular lenses (IOLs). Two temporal incisions are made, one superotemporal for the cutter, scissors, forceps, fragmenter, laser, etc. and another inferotemporal for the infusion cannula. They should be limbus-parallel, 1 mm posterior to the limbus, and at the superior and inferior border of the lateral rectus. The superonasal incision is usually for the endoilluminator and should be limbus-parallel, 1 mm posterior to the limbus, and centered at the superior border of the medial rectus. A small radial extension of the limbus-parallel incisions at one end resulting in an L-shaped flap facilitates better exposure and single suture closure.
For any vitreous surgery in which scleral buckling is anticipated, it is best to make a continuous incision 1 mm posterior to the limbus including each quadrant requiring buckling. A limbal peritomy tends to bleed under the contact lens, causes conjunctival retraction and redundancy problems in the postoperative course, and makes postoperative contact lens fitting difficult and dellen more common. Incisions more than 1 mm behind the limbus increase the risk of exposure of scleral sutures and make visualization of the sclerotomies difficult because of the anterior flap.
TRACTION SUTURES
Traction sutures under the muscles are of no value in vitrectomy because the instruments move the eye. Only if scleral buckling is anticipated should traction sutures be used, and then they should be placed beneath the muscles directly, using a short-handled fenestrated muscle hook with chamfered hole. Large sutures (0 to 2-0 silk or cotton) do not cut the muscle tendons and provide a good grip for the assistant. Only the muscles absolutely required for access to the sclera should be trapped to reduce postoperative pain, ptosis, and strabismus. The superior rectus should be avoided if possible to avoid or reduce vertical strabismus as well as ptosis secondary to levator and Mueller’s muscle damage. It is never necessary to remove muscles for scleral buckling or trauma repair in the author’s experience.
20-GAUGE SCLERAL INCISIONS
Sclerotomies for the endosurgical instruments will be focal points for the remainder of the operation (1). If they are incorrectly placed or constructed, the entire course of the operation can be adversely influenced. The incisions should be placed in the anterior pars plana to reduce the risk of damage to the peripheral retina. Contrary to customary teaching, bleeding of the ciliary body is infrequent and rarely serious when it does occur. Except in children, patients with an abnormal pars plana, and microphthalmic patients, the sclerotomies should be placed 3 mm posterior to the limbus if the lens is absent or to be removed and 4 mm posterior if the lens is to be retained (Fig. 10.1). Some surgeons use 3.5 mm for all cases as the authors do for 25-gauge cases. The authors use 25-gauge, sutureless, transconjunctival surgery for almost all cases; the following techniques apply only to sutured 20-gauge surgery.
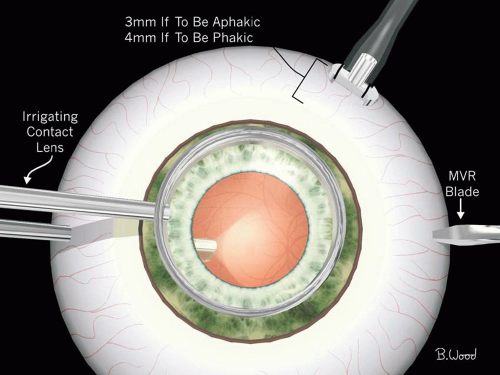 Figure 10.1 ▪ All sclerotomies are made with MVR blade, 3 mm posterior to the limbus if aphakic or lens is to be removed and 4 mm posterior to the limbus if lens is to be retained. |
The disposable microvitreoretinal (MVR) blade is ideal for making 20-gauge sclerotomies. The blade is lancet shaped to ensure that the incision is centered at the initial entry point (Fig. 10.2). The blade is 1.4 mm in width, which makes a linear incision that becomes 0.89 mm (20 gauge) in diameter when deformed to a circular shape by the instruments. The nontapered, 20-gauge shank and 25-mm length correspond to the dimensions of the other endosurgical instruments. Stilettos, myringotomy blades, illuminated stab needles, 20-gauge needles, and transilluminators are unnecessary with this method. Prefirming prior to use of the MVR blade is unnecessary because the tip of a high-quality MVR blade is typically as sharp as a 30-gauge needle and provides a correct size incision if a subsequent fluid injection is required.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


